Embed Size (px)
Citation preview

Accuracy of IRAS GT interferometerand potential acuity meterprediction of visual acuityafter phacoemulsificationProspective comparative study
Cecile Le Sage, MD, Christian Bazalgette, DBO, Bernard Arnaud, MD,Clair-Florent Schmitt-Bernard, MD, PhD
ABSTRACT
Purpose: To assess and compare the accuracy of 2 methods of predicting visual acuityafter phacoemulsification.
Setting: Department of Ophthalmology, Montpellier, France.
Methods: This prospective study evaluated 47 eyes of 47 patients having uneventfulphacoemulsification over a 1-month period. All the patients had mild to moderatecataract. Visual acuity recovery was predicted using the white-light IRAS GT� inter-ferometer on the 3- and 8-degree wide test area and the Guyton-Minkowski potentialacuity meter (PAM). Best corrected visual acuity was evaluated 1 day before and1 month after surgery.
Results: Both the interferometer and PAM underestimated the retinal visual capacity.Three-degree white-light interferometry gave significantly better mean predicted resultsthan 8-degree interferometry and the PAM. There was no statistically significant dispar-ity between predicted and postoperative results with 3-degree interferometry (1.04 �
0.57 logMAR; –0.09 � 0.27 decimal) (P � .0647) and a statistically significant disparitywith 8-degree interferometry (0.89 � 0.59 logMAR; –0.13 � 0.27 decimal) and the PAM(0.66 � 0.62 logMAR; –0.22 � 0.24 decimal) (P � .0001). The predicted values werewidely dispersed; the correlation indices were 0.38 with the PAM (P � .091), 0.39 with3-degree interferometry (P � .001), and 0.49 with 8-degree interferometry (P � .0005).
Conclusions: Three-degree white-light interferometry gave more accurate results than8-degree interferometry and the PAM. The wide dispersion of results and unsatisfactorycorrelation indices show the tests are poor predictors of individual acuity. They shouldbe used semiquantitatively and the results interpreted in relation to the clinical data.Qualitative methods may be useful in confirming or refuting visual recovery capacityascertained by quantitative systems. J Cataract Refract Surg 2002; 28:131–138© 2002 ASCRS and ESCRS
© 2002 ASCRS and ESCRS 0886-3350/02/$–see front matterPublished by Elsevier Science Inc. PII S0886-3350(01)01118-X

The considerable contribution of cataract surgery tothe patient’s quality of life began with its early de-
velopment. Phacoemulsification further improved thepopularity of this surgery as its duration is short andvisual rehabilitation is fast. Thus, patients expect earlyand reliable visual recovery, and a poor visual outcome isdisappointing to patients and surgeons, especially afteruneventful phacoemulsification.
Poor visual recovery after phacoemulsification is fre-quently linked to undiagnosed retinal disease, which canbe related to fundoscopy difficulty in cases of severecataract, or to retinal or corneal pathology, which makesprediction of visual recovery unreliable.
Various methods to predict retinal acuity and therisk/benefit ratio after extracapsular cataract extraction(ECCE) have been developed. Several are based on ret-inal qualitative indices. These include electroretinogra-phy,1–3 visual evoked potentials,1,2,4,5 color visiontests,6 blue-field entoptic tests,7–9 and B-scan ultra-sonography.2 Others are based on quantitative criteriausing pinhole techniques (J. Lowry, “Pinhole Tech-niques Are Called Reliable, Easy, and Inexpensive,”Ophthalmology Times, September 1, 1986, pages 1, 31,35), laser or white-light interferometry,10–13 and poten-tial acuity meter (PAM) assessment.14,15
In this prospective study, we analyzed the predictedresults of visual recovery after phacoemulsification using2 technologically different quantitative methods: white-light interferometry and the PAM assessment. We sta-tistically estimated the results of both systems. To ourknowledge, no similar comparison of these methods hasbeen published.
Patients and Methods
This study comprised 47 eyes of 47 patients(30 men, 17 women) having cataract surgery over a1-month period, the single criterion for their inclusion.No patient had previous ocular surgery. All patientshad phacoemulsification with in-the-bag intra-ocular lens implantation by the same surgeon (B.A.)with no postoperative complications over a 2-monthfollow-up.
The patients’ demographics are shown in Table 1.The mean age of the patients was 70.38 years � 15.84(SD) (range 19 to 92 years); 70% were older than70 years, fitting the general population requestingcataract surgery. All patients had mild to moderate cat-aract. Five patients (#2, 5, 10, 19, 33) had high myopia(range –9.0 to –15.0 diopters [D]); 4 (#3, 23, 31, 45)had posterior subcapsular cataract; 4 (#9, 15, 28, 42)had atrophic age-related macular degeneration(ARMD) and 1 (#16) exudative ARMD; 2 (#13, 35)had retinitis pigmentosa; 1 (#43) was amblyopic;1 (#40) had a complex syndrome comprising cornealdystrophy, aniridia, and nystagmus; and 1 (#47) hadopen-angle glaucoma.
Preoperatively, a single evaluator performed aclinical examination. This included slitlamp and fundo-scopic evaluations and intraocular pressure measure-ment. The best corrected visual acuity (BCVA) wasevaluated using the decimal scale 1 day before and1 month after surgery.
Prediction of visual acuity recovery was per-formed by a single trained examiner by the 2 meth-ods available in the Department of Ophthalmology:the white-light IRAS GT� interferometer (RandwallInstruments) on the 3- and 8-degree wide test area orthe Guyton-Minkowski PAM (Mentor O&O Inc.).One drop of tropicamide was instilled 30 minutes beforeto obtain adequate pupil dilation in photopic condi-tions. To ensure their cooperation, all patients receiveda thorough description of the instrument and itstechnique.
The IRAS GT is a white-light interferometer. Thelight emitted from an incandescent source is focused ona holographic grating that splits the single coherentsource into 2 equally strong coherent lights. A relay lenssystem projects the 2 slit sources near the nodal point ofthe eye, where coherent light waves emanating from
Accepted for publication July 30, 2001.
From Service d’Ophtalmologie, CMC Gui de Chauliac, Montpellier,France.
Gaston Le Sage, Institut National des Statistiques et des EtudesEconomiques, Montpellier, France, provided statistical analysis and Mi-kael Tritz, Ecole d’Ingenierie, Bourges, France, helped translate fromGerman.
None of the authors has a financial or proprietary interest in any materialor method mentioned.
Reprint requests to Dr. Clair-Florent Schmitt-Bernard, Antigone Oph-talmologie, Le Jardin Du Centre, Rue De L’Epire, 34000 Montpellier,France. E-mail: [email protected]/[email protected].
VISUAL ACUITY RECOVERY AFTER PHACOEMULSIFICATION
J CATARACT REFRACT SURG—VOL 28, JANUARY 2002132

Table 1. Patient characteristics and visual acuities.
PatientAge
(Years) Sex
Decimal VA (LogMAR VA)
Preop IF-3 IF-8 PAM Postop
1 75 M 0.40 (0.40) 0.80 (0.10) 0.67 (0.17) 0.80 (0.10) 0.90 (0.05)
2 64 F 0.40 (0.40) NA 1.00 (0.00) 0.50 (0.30) 0.80 (0.10)
3 64 F 0.20 (0.70) 0.33 (0.48) 0.33 (0.48) 0.40 (0.40) 0.90 (0.05)
4 80 F 0.40 (0.40) 1.00 (0.00) 0.67 (0.17) 0.50 (0.30) 0.90 (0.05)
5 70 F 0.40 (0.40) 0.67 (0.17) 0.67 (0.17) 0.50 (0.30) 0.60 (0.22)
6 70 F 0.40 (0.40) 0.50 (0.30) 0.67 (0.17) 0.80 (0.10) 0.60 (0.22)
7 80 F 0.30 (0.52) 0.80 (0.10) 0.67 (0.17) 0.33 (0.48) 0.90 (0.05)
8 63 F 0.40 (0.40) 1.00 (0.00) 1.00 (0.00) 0.40 (0.40) 0.80 (0.10)
9 92 F 0.10 (1.00) NA 0.05 (1.30) 0.50 (0.30) 0.10 (1.00)
10 61 F 0.20 (0.70) 0.80 (0.10) 0.33 (0.48) 0.25 (0.60) 0.30 (0.52)
11 69 F 0.40 (0.40) 0.80 (0.10) 0.67 (0.17) 0.80 (0.10) 0.80 (0.10)
12 28 M 0.40 (0.40) 1.00 (0.00) 1.00 (0.00) 0.80 (0.10) 1.00 (0.00)
13 68 M 0.10 (1.00) 0.02 (1.60) 0.02 (1.60) 0.10 (1.00) 0.10 (1.00)
14 88 M 0.40 (0.40) 1.00 (0.00) 0.80 (0.10) 0.50 (0.30) 0.80 (0.10)
15 82 F 0.20 (0.70) NA 0.05 (1.30) 0.10 (1.00) 0.30 (0.52)
16 78 F 0.40 (0.40) 1.00 (0.00) 1.00 (0.00) 0.40 (0.40) 0.50 (0.30)
17 64 F 0.30 (0.52) 0.67 (0.17) 0.40 (0.40) 0.50 (0.30) 0.70 (0.15)
18 77 F 0.20 (0.70) 0.50 (0.30) 0.50 (0.30) 0.28 (0.55) 0.50 (0.30)
19 78 F 0.40 (0.40) 0.80 (0.10) 0.40 (0.40) 0.50 (0.30) 0.70 (0.15)
20 79 F 0.30 (0.52) 0.67 (0.17) 0.67 (0.17) 0.33 (0.48) 0.90 (0.05)
21 74 F 0.40 (0.40) 0.80 (0.10) 1.00 (0.00) 0.66 (0.18) 0.90 (0.05)
22 77 M 0.50 (0.30) 0.80 (0.10) 0.67 (0.17) 0.80 (0.10) 0.90 (0.05)
23 30 M 0.05 (1.30) 0.02 (1.60) 0.02 (1.60) 0.50 (0.30) 0.80 (0.10)
24 57 M 0.40 (0.40) 0.50 (0.30) 0.50 (0.30) 0.33 (0.48) 1.00 (0.00)
25 74 M 0.40 (0.40) 0.80 (0.10) 0.80 (0.10) 0.50 (0.30) 1.00 (0.00)
26 85 M 0.40 (0.40) 0.80 (0.10) 0.80 (0.10) 0.66 (0.18) 0.80 (0.10)
27 76 F 0.20 (0.70) 0.50 (0.30) 0.50 (0.30) 0.40 (0.40) 1.00 (0.00)
28 78 F 0.30 (0.52) 0.02 (1.60) 0.33 (0.40) 0.50 (0.30) 0.50 (0.30)
29 79 F 0.40 (0.40) 0.33 (0.40) 0.20 (0.70) 0.50 (0.30) 0.80 (0.10)
30 85 M 0.40 (0.40) 1.00 (0.00) 0.80 (0.10) 0.80 (0.10) 1.00 (0.00)
31 62 F 0.16 (0.80) 0.25 (0.60) 0.30 (0.52) 1.00 (0.00) 0.70 (0.15)
32 73 F 0.40 (0.40) 1.00 (0.00) 0.80 (0.10) 0.66 (0.18) 1.00 (0.00)
33 75 M 0.10 (1.00) 0.33 (0.40) 0.25 (0.60) 0.28 (0.55) 0.60 (0.22)
34 76 M 0.40 (0.40) 0.67 (0.17) 0.67 (0.17) 0.50 (0.30) 0.70 (0.15)
35 80 F LP NA NA NA LP
36 80 F 0.16 (0.80) 0.67 (0.17) 0.67 (0.17) 0.50 (0.30) 1.00 (0.00)
37 62 M 0.40 (0.40) 0.80 (0.10) 0.67 (0.17) 0.66 (0.18) 0.60 (0.22)
38 73 F 0.40 (0.40) 1.00 (0.00) 0.80 (0.10) 0.80 (0.10) 0.80 (0.10)
39 78 F 0.10 (1.00) 0.67 (0.17) 0.40 (0.40) 0.20 (0.70) 1.00 (0.00)
40 23 F 0.05 (1.30) 0.40 (0.40) 0.80 (0.10) NA 0.10 (1.00)
VISUAL ACUITY RECOVERY AFTER PHACOEMULSIFICATION
J CATARACT REFRACT SURG—VOL 28, JANUARY 2002 133

each source interfere and form a series of black-and-white lines on the retina. Orientation of the lines can beset vertically, horizontally, or diagonally by rotating theholographic grating. The equivalent acuity depends onthe interaction angle between the interfering wavefronts. The distance between these lines defines Snellenvisual acuity from 20/800 to 20/20 independent of thepatient’s refraction. The gratings and Snellen letters donot have direct correlation because of the higher fre-quency components of the Snellen letters. A 3- or 8-de-gree area of central retina can be evaluated depending onthe diaphragm aperture.
The Guyton-Minkowski PAM projects a Snellenchart ranging from 20/400 to 20/20 in a small beamof light (0.15 mm diameter aperture). The light beamis aimed through the less opaque area of the lens. Thediopter control is set at the spherocylindrical equiva-lent of the patient’s refraction (–10.0 to �13.0 D).In patients with myopia greater than –10.0 D, themeasurement was done with the best spectaclecorrection.
Statistical AnalysisPreoperative and postoperative visual acuities were
compared with the results of the predictive tests, andtheir statistical significance was analyzed using the Wil-coxon matched test as the distribution did not fit aGaussian pattern. The Altman and Bland test was usedto determine the dispersion of results, and their correla-tion was calculated by the Spearman correlation test.Decimal visual acuity was expressed as a logMAR equiv-alent for data analysis.16
Results
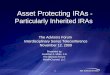
The mean preoperative BCVA was 0.57 � 0.27logMAR (range light perception [LP] to 0.30) and0.27 � 0.54 decimal (range LP to 0.50). The meanpostoperative BCVA was (0.19 � 0.25) logMAR (rangeLP to 0.00) and 0.64 � 0.56 decimal (range LP to 1.0).The predicted visual acuity was significantly closer to thefinal visual acuity with 3-degree interferometry (0.27 �0.40 logMAR; 0.54 � 0.40 decimal) than with 8-degreeinterferometry (0.33 � 0.39 logMAR; 0.47 � 0.41 dec-imal) or the PAM (0.31 � 0.23 logMAR; 0.49 � 0.59decimal) (Figure 1).
The 3 methods of prediction displayed a non-Gaus-sian curve of distribution of results. There was no statis-tically significant disparity between predicted andpostoperative results with 3-degree interferometry(1.04 � 0.57 logMAR; –0.09 � 0.27 decimal) (P �.0647) and a statistically significant disparity with 8-de-gree interferometry (0.89 � 0.59 logMAR; –0.13 �0.27 decimal) and the PAM (0.66 � 0.62 logMAR;–0.22 � 0.24 decimal) (P � .0001). Therefore, themean predictive results with 3-degree interferometrysignificantly matched the final visual acuity, and all3 tests underestimated postoperative visual acuity. Themean underestimation was less than 1 line (decimalscale) with 3-degree interferometry, making it the mostaccurate method of predicting visual acuity recovery.
There was no significant difference in the level ofdispersion of results between 3-degree interferometry(–0.81 to 0.60 logMAR) and 8-degree interferometry(–0.79 to 0.51 logMAR) (P � .0001), 3-degree inter-
Table 1. (cont.)
PatientAge
(Years) Sex
Decimal VA (LogMAR VA)
Preop IF-3 IF-8 PAM Postop
41 74 F 0.30 (0.52) 0.67 (0.17) 0.50 (0.30) 1.00 (0.00) 0.90 (0.05)
42 76 F 0.40 (0.40) 1.00 (0.00) 1.00 (0.00) 1.00 (0.00) 0.80 (0.10)
43 19 M 0.05 (1.30) 0.50 (0.30) 0.40 (0.40) 0.28 (0.55) 0.50 (0.30)
44 81 M 0.30 (0.52) 0.67 (0.17) 0.67 (0.17) 0.50 (0.30) 0.60 (0.22)
45 78 F 0.40 (0.40) 0.20 (0.70) 0.40 (0.40) 0.66 (0.18) 0.50 (0.30)
46 80 F 0.40 (0.40) 0.80 (0.10) 0.67 (0.17) 1.00 (0.00) 0.90 (0.05)
47 73 M 0.40 (0.40) 1.00 (0.00) 1.00 (0.00) 0.80 (0.10) 0.90 (0.05)
VA � visual acuity; IF-3 � 3-degree interferometry; IF-8 � 8-degree interferometry; PAM � potential acuity meter; LP � light perception; NA �
not applicable
VISUAL ACUITY RECOVERY AFTER PHACOEMULSIFICATION
J CATARACT REFRACT SURG—VOL 28, JANUARY 2002134

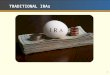
ferometry and the PAM (–0.58 to 0.30 logMAR) (P �.0216), or 8-degree interferometry and the PAM (P �.003) (Figure 2). Therefore, even though 3-degree inter-ferometry appeared to be the best predictor, the disper-
sion test showed that individual prediction may beoverestimated or underestimated from �0.25 to –0.15lines on the decimal scale around the mean result. Thiswas also true with 8-degree interferometry (�0.31 to–0.16 lines, decimal) and the PAM (�0.50 to –0.26lines, decimal). The PAM had a wider dispersion ofresults than either interferometry method when individ-ually results were considered; the difference was not sta-tistically significant, however.
There was a significantly poor individual correla-tion between predicted and postoperative visual acuitieswith all 3 methods: 3-degree interferometry (r � 0.39,P � .01); 8-degree interferometry (r � 0.49, P �.0005); PAM (r � 0.38, P � .0091).
DiscussionIn this comparative study, 3-degree white-light in-
terferometry was more reliable in predicting postopera-tive visual acuity than 8-degree interferometry or thePAM; the mean prediction with 3-degree white-lightinterferometry was approximately 1 line (decimal scale)from the final visual acuity. However, all 3 methodsunderestimated postoperative visual acuity, which mayhave relatively little effect on patient satisfaction. It maybe of concern to surgeons evaluating the risk/benefitratio of cataract surgery. All 3 methods had a tendencytoward poor prediction of individual acuity as the dis-persion of results was significantly wide and the correla-tion indices unsatisfactory. Thus, none of the methodscan predict final visual acuity in a linear mode and aprediction of poor visual recovery may not reflect anindividual’s visual capacity.
All the patients in our study had mild to moderatecataract. There were no cases of mature cataract, whichis more likely to induce a false negative (underestimated)
Figure 1. (Le Sage) Variation be-tween predicted and actual postoper-ative visual acuity (black bar �
3-degree interferometry; white bar �
8-degree interferometry; gray bar �
PAM; y-axis � acuity, decimal scale).
Figure 2. (Le Sage) Dispersion of predicted versus final visualacuity. Top: 3-degree interferometry (IF-3°). Middle: 8-degree inter-ferometry (IF-8°). Bottom: PAM (x- and y-axis � logMAR scale).
VISUAL ACUITY RECOVERY AFTER PHACOEMULSIFICATION
J CATARACT REFRACT SURG—VOL 28, JANUARY 2002 135

predicted visual acuity. Other conditions reported toinduce inaccurate prediction of visual recovery are pos-terior subcapsular cataract, high myopia, ARMD, cys-toid macular edema, retinal detachment, amblyopia,nystagmus, glaucoma, and miosis.17–23
In our study, 4 of the 5 myopic patients displayed astrong disparity in predicted visual acuity and final vi-sual acuity between the 2 interferometry tests and be-tween the interferometer and the PAM. The orientationof the light rays reaching adjacent areas of the retina maybe a cause of this disparity.19,20 Thus, the 3 methodsseemed inaccurate in predicting final acuity in eyes withhigh myopia. This is in contrast to the results of Datileset al.,24 who report accurate predicted acuity in 3 casesof high myopia. Datiles et al. stress that the low preop-erative visual acuity in high myopia may be the result ofamplified distortion when the light passes through evena moderate cataract.
The predicted acuity was underestimated by inter-ferometry in all 4 patients with posterior subcapsularcataract and by the PAM in 3 of the patients. The resultssupport the findings of Lasa and coauthors21 andSchraub and coauthors,23 who used a Rodenstock� reti-nometer and the PAM to predict acuity. Both groupshypothesize that this underestimation is linked to theincreased central density of the opacity in a nuclear cat-aract; the opacity is more diffuse and regular, givingmore reliable values.
As previously described,17,18,21,25 interferometryaccurately predicted visual acuity in patients with atro-phic ARMD and overestimated it in the patient withexudative ARMD. The PAM results were more accuratein the case of exudative ARMD.
The postoperative visual acuity matched the pre-dicted outcome with all 3 methods in patients with pig-ment epithelium retinopathy, which agrees with thefindings in a previous study.26 The results in the patientwith amblyopia were also accurate, which is in contrastto previous studies showing overestimation in such cas-es.9 In the patient with nystagmus, interferometry over-estimated and the PAM underestimated final visualacuity, as reported in a previous study.27 However, con-clusions cannot be made based on the evaluation of asingle individual.
There was a significant disparity among the 3 meth-ods in predicting visual acuity recovery after phacoemul-sification. The best results were obtained with 3-degree
interferometry. This in agreement with the results ofGoldmann and coauthors,20 who suggest that smallfields are more accurately centered on the fovea and maybe more accurate in patients suspected of having macu-lar disease. This prevents test recognition from theparafoveal retina.
In our study, a single trained examiner performed allvisual acuity prediction tests after providing patients adetailed explanation. This increased the reliability of theresults. Miller et al.29 propose that the poor correlationindices in their series of 82 patients obtained with bothinterferometry (r � 0.03) and the PAM (r � 0.07) werethe result of the technician’s lack of experience as well asthe patients’ ages and associated diseases, which lead topoor cooperation. These biases result in a poor estima-tion of visual acuity recovery and thus contradictoryoutcomes among studies.25,28–31
Few studies have compared the use of interferom-etry and the PAM in ECCE. Most did not providea statistical analysis to determine whether interferom-etry or the PAM is significantly accurate. Spurny andcoauthors25 compared a white-light interferometer(Lotmar visometer, Haag-Streit) with the PAM in54 eyes having cataract surgery or neodymium:YAGlaser capsulotomy. Predictions were more accuratewith the visometer than the PAM, supporting ourresults. Strong30 compared the Rodenstock laserinterferometer, Lotmar visometer, and white-lightIRAS interferometer in 14 eyes. The laser interferome-ter was the most accurate, but no statistical analysiswas reported. Graney et al.28 found laser interferometryand the PAM less accurate than a clinical index based onage, preoperative visual acuity, number of current pre-scription medications, and the ability to read a newspa-per. Nevertheless, these studies had several biases asdifferent ophthalmologists performed the predictiontests and all patients were from middle- or upper-classfamilies. However, the PAM was statistically more accu-rate in predicting acuity than laser interferometry. In aprospective study of 35 eyes, Datiles et al.24 found thatthe PAM and laser interferometer were equally goodpredictors in cases of mild to moderate cataract. Gold-stein et al.31 found better results with the Lotmar vi-someter than with the IRAS interferometer. Therefore,it appears that these studies had several strong examinerand patient biases, which may account for the contra-dictory results.
VISUAL ACUITY RECOVERY AFTER PHACOEMULSIFICATION
J CATARACT REFRACT SURG—VOL 28, JANUARY 2002136

ConclusionOur findings suggest that the interferometer and
the PAM are accurate predictors of postoperative vi-sual acuity in healthy eyes with moderate cataract.Conversely, both instruments lack reliability in eyeswith retinal disorders. These methods are suited todaily practice as they are fast and easy and give reliableprediction of visual recovery in most patients havingphacoemulsification.
However, we believe that the instruments should beused semiquantitatively and the results be interpreted inrelation to the clinical data. The results must also beassessed on an individual basis considering their widedispersion, especially in patients with associated ocularpathology. In this respect, qualitative methods may helpconfirm or refute the capacity for visual recovery ascer-tained by quantitative systems.
References
1. Bertrand F, Delplace MP, Bertrand P. Interet de l’ERG etdes VEP en rouge dans le pronostic preoperatoire descataractes seniles. Bull Soc Ophtalmol Fr 1984;84:1321–1324
2. Sherman J, Davis E, Schnider C, et al. Presurgical predic-tion of postsurgical visual acuity in patients with mediaopacities. J Am Optom Assoc 1988; 59:481–488
3. Wu D-Z, Wu L, XU X, et al. The significance of testingpreoperative visual function in cataract using laser inter-ferometric visual acuity and ERG. Yen Ko Hsueh Pao1991; 7:21–24
4. Odom JV, Chao G-M, Weinstein GW. Preoperative pre-diction of postoperative visual acuity in patients withcataracts: a quantitative review. Doc Ophthalmol 1988;70:5–17
5. Van Lith GHM, Hekkert-Wiebenga W. Cataract, pat-tern stimulation and visually evoked potentials. DocOphthalmol 1983; 55:107–112
6. Kogure S, Iijima H, Tsukahara S. Assessment of potentialmacular function using a color saturation discriminationtest in eyes with cataract. J Cataract Refract Surg 1999;25:569–574
7. Grignolo FM, Moscone F, Sobrero C, Leone M. Evalu-ation of macular function by Lotmar’s visometer test andblue-field entoptic test in patients with cataract. AnnOphthalmol 1988; 20:247–250
8. Miris R, Missotten L. Evaluation of the macular functionin cataractous eyes by means of the blue field entopto-scope. Bull Soc Belge Ophtalmol 1982; 201:121–126
9. Sinclair SH, Loebl M, Riva CE. Blue field entoptic phe-
nomenon in cataract patients. Arch Ophthalmol 1979;97:1092–1095
10. Lotmar W. Apparatus for the measurement of retinalvisual acuity by moire fringes. Invest Ophthalmol Vis Sci1980; 19:393–400
11. Goldmann H, Lotmar W. Retinale Sehscharfenbestim-mung bei Katarakt. Ophthalmologica 1970; 161:175–179
12. Green DG. Testing the vision of cataract patients bymeans of laser-generated interference fringes. Science1970; 168:1240–1242
13. Rassow B, Ratzke P. Der prognostische Wert der Bestim-mung der retinalen Sehscharfe bei Patienten mit Kat-arakt. Klin Monatsbl Augenheilkd 1977; 171:643–650
14. Minkowski JS, Guyton DL. New methods for predictingvisual acuity after cataract surgery. Ann Ophthalmol1984; 16:511–516
15. Cavonius CR, Hilz R. A technique for testing visual func-tion in the presence of opacities. Invest Ophthalmol1973; 12:933–936
16. Holladay JT. Proper method for calculating average vi-sual acuity. J Refract Surg 1997; 13:388–391
17. Faulkner W. Laser interferometric prediction of postop-erative visual acuity in patients with cataracts. Am J Oph-thalmol 1983; 95:626–636
18. Bloom TD, Fishman GA, Traubert BS. Laser interfero-metric visual acuity in senile macular degeneration. ArchOphthalmol 1983; 101:925–926
19. Gstalder RJ, Green DG. Laser interferometric acuity inamblyopia. J Pediatr Ophthalmol Strabismus 1971;8:251–266
20. Goldmann H, Chrenkova A, Cornaro S. Retinal visualacuity in cataractous eyes; determination with interfer-ence fringes. Arch Ophthalmol 1980; 98:1778–1781
21. Lasa MSM, Datiles MB II, Freidlin V. Potential visiontests in patients with cataracts. Ophthalmology 1995;102:1007–1011
22. Rassow B, Wolf D. Die Messung der “retinalen Sehs-charfe” mit dem Laserinterferenzgerat als klinische Rou-tinemethode. Adv Ophthalmol 1977; 34:116–142
23. Schraub M, Flament J, Sahel J, Bronner A. Evaluation dela capacite fonctionnelle maculaire interferometrie au la-ser helium-neon. J Fr Ophtalmol 1985; 8:427–432
24. Datiles MB, Edwards PA, Kaiser-Kupfer MI, et al. Acomparative study between the PAM and the laser inter-ferometer in cataracts. Graefes Arch Clin Exp Ophthal-mol 1987; 225:457–460
25. Spurny RC, Zaldivar R, Belcher CD III, SimmonsRJ. Instruments for predicting visual acuity; a clinicalcomparison. Arch Ophthalmol 1986; 104:196–200
26. Kogure S, Iijima H. Preoperative evaluation by laser in-terferometry in cataractous eyes with retinitis pigmen-tosa. Jpn J Ophthalmol 1993; 37:282–286
27. Minkowski JS, Palese M, Guyton DL. Potential Acuity
VISUAL ACUITY RECOVERY AFTER PHACOEMULSIFICATION
J CATARACT REFRACT SURG—VOL 28, JANUARY 2002 137

Meter using a minute aerial pinhole aperture. Ophthal-mology 1983; 90:1360–1368
28. Graney MJ, Applegate WB, Miller ST, et al. A clinicalindex for predicting visual acuity after cataract surgery.Am J Ophthalmol 1988; 105:460–465
29. Miller ST, Graney MJ, Elam JT, et al. Predictions ofoutcomes from cataract surgery in elderly persons. Oph-thalmology 1988; 95:1125–1129
30. Strong N. Interferometer assessment of potential visualacuity before YAG capsulotomy: relative performance ofthree instruments. Graefes Arch Clin Exp Ophthalmol1992; 230:42–46
31. Goldstein J, Jamara RJ, Hecht SD, et al. Clinical com-parison of the SITE IRAS hand held interferometer andHaag-Streit Lotmar visometer. J Cataract Refract Surg1988; 14:208–211
VISUAL ACUITY RECOVERY AFTER PHACOEMULSIFICATION
J CATARACT REFRACT SURG—VOL 28, JANUARY 2002138