Embed Size (px)
Citation preview

8/3/2019 Invited Lecture 25 ES Complications
http://slidepdf.com/reader/full/invited-lecture-25-es-complications 1/25
Short-Term and Long-term
Complications of EndoscopicSphincterotomy for CBD Stones
Ahmad Nassar
Monklands HospitalScotland

8/3/2019 Invited Lecture 25 ES Complications
http://slidepdf.com/reader/full/invited-lecture-25-es-complications 2/25
ES for CBD Stones
Classen and Kawai- mid 70’s
Safrany L, Lancet, Nov 1978: ‘ES isincreasingly replacing surgery in the
treatment of choledocholithiasis’
Manegold BC, Langenbecks Arch Chir, Nov 1978: ‘ Late complications after EST
are unknown and not to be expected

8/3/2019 Invited Lecture 25 ES Complications
http://slidepdf.com/reader/full/invited-lecture-25-es-complications 3/25
Early Complications of ES
Sedation
Basket impaction
Pancreatitis
Bleeding
Cholangitis
Perforation
Failure
Early papillary stenosis

8/3/2019 Invited Lecture 25 ES Complications
http://slidepdf.com/reader/full/invited-lecture-25-es-complications 4/25
Late Complications of ES
Recurrent stones
Acute cholecystitis
Recurrent pancreatitis Re-stenosis of papilla
Cholangiocarcinoma
Rare complications: new GB stones,gallstone ileus, Ascaris in CBD

8/3/2019 Invited Lecture 25 ES Complications
http://slidepdf.com/reader/full/invited-lecture-25-es-complications 5/25
Study No. Early Comp. Late Comp. Mortality
Seifert
1982
9041 7.5% 5.7% recurr
3.1 restenosis
1.12%
Escourou
1984
443
43%
7% 12% chole
6% rec Pancr
1.5%
Liquory
1985
409
57%
13% 4%
Leese
1985
394 10.4%
Surgery 3.8%
3.3%
Dresemann
1988
185
3.8%
Surgery 0.5%
16.9%
Surgery 5.6%
2.8%
Kullman
1989
128
ALL
164 ES 16.5%
Surgery 3.1%
3.1%

8/3/2019 Invited Lecture 25 ES Complications
http://slidepdf.com/reader/full/invited-lecture-25-es-complications 6/25
Pre-Laparoscopic Era
Great majority cholecystectomised
Almost all those with GB in situ unfit for
surgery Few specialised, skilled, high-volume
centres
Morbidity and mortality go with thepathology

8/3/2019 Invited Lecture 25 ES Complications
http://slidepdf.com/reader/full/invited-lecture-25-es-complications 7/25
Risk Factors in ES
Clinical:
Acute cholangitis
Sphincter of Oddi Dysfunction
Coagulopathy
Technical:
Difficult cannulation
Pre-cut Small ducts
Wide ducts

8/3/2019 Invited Lecture 25 ES Complications
http://slidepdf.com/reader/full/invited-lecture-25-es-complications 8/25
Lessons: pre-laparoscopic era
Neoptolemos J P, et al
Br Med J. 1987;294:470-4 Prospective
randomised study of preoperative endoscopic
sphincterotomy versus surgery alone for commonbile duct stones
No advantage for ES+cholecystectomy over BDE
‘Routine preoperative ES is of questionable value’

8/3/2019 Invited Lecture 25 ES Complications
http://slidepdf.com/reader/full/invited-lecture-25-es-complications 9/25
Neoptolemos 438 patients 5 years
Group Number Morbidity Mortality
ES +
surgery
59 23.7% *
p<0.001
5.1%
Surgery
alone
248 8.5% 4%
ES alone
GB in situ
114 19.3% *
p<0.003
7.9%
ES alone
NO GB
17 17.6% 17.6%

8/3/2019 Invited Lecture 25 ES Complications
http://slidepdf.com/reader/full/invited-lecture-25-es-complications 10/25
The ‘new’ concepts of the
laparoscopic era
Clear the CBD before cholecystectomy !
Laparoscopic IOC is time-consuming !
Laparoscopic CBDE is difficult !
‘Plan operating lists’ !
Limited facilities for urgent biliary surgery ! Gallstone surgery is minimally invasive !?

8/3/2019 Invited Lecture 25 ES Complications
http://slidepdf.com/reader/full/invited-lecture-25-es-complications 11/25
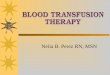
0
500
1000
1500
2000
2500
3000
3500
4000
4500
5000
1989/90 1990/91 1991/92 1992/93 1993/94 1994/95 1995/96 1996/97 1997/98 1998/99
ERCPs (OPCS4 J38:J45) recorded in any position
Laparoscopic cholecystectomy (OPCSJ08.8, J18+Y50.8)
Cholecystectomy & exploration of common bile duct (J18.2) recorded in any position
Calculus of bile duct with/without cholangitis or cholocystitis recorded in any position* with any or no procedure recorded

8/3/2019 Invited Lecture 25 ES Complications
http://slidepdf.com/reader/full/invited-lecture-25-es-complications 12/25
ERCP in England 1990-1999
90/91 98/99 Increase %
Diagnostic; Surgery 5027 10400
Medicine 6169 11252
Total 11196 21652 190 %
Therapeutic; Surgery 2037 8162
Medicine 1980 8197
Total 4017 16359 400 %
All ERCP’s 15213 38011 250 %

8/3/2019 Invited Lecture 25 ES Complications
http://slidepdf.com/reader/full/invited-lecture-25-es-complications 13/25
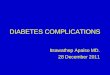
Number of deaths and mortality rate for patients undergoing ERCP procedures and diagnosed with benign gallstone dis
Time period: January 1992 to December 2001 p
Year
Number
of deaths
Mortali
rate (
1992 48 3.4
1993 66 3.5
1994 79 3.7
1995 63 2.6
1996 107 4.2
1997 105 4.1
1998 119 4.3
1999 76 2.7
2000 88 3.2
2001p 60 2.3
Source: ISD linked data set
30 January 2003
p provisional

8/3/2019 Invited Lecture 25 ES Complications
http://slidepdf.com/reader/full/invited-lecture-25-es-complications 14/25
We are not alone

8/3/2019 Invited Lecture 25 ES Complications
http://slidepdf.com/reader/full/invited-lecture-25-es-complications 15/25
Berci G,
J Laparoendosc Surg,1993:4:427
‘.. Surgeons performing LC should
nowadays consider advancing their
technique in learning how to do
laparoscopic choledocho-lithotomy
‘.. I think it is the wrong philosophy to
divide biliary stone disease to be treated
in two sessions or even by two disciplines’

8/3/2019 Invited Lecture 25 ES Complications
http://slidepdf.com/reader/full/invited-lecture-25-es-complications 16/25
Cetta F, CBD stones in the era of LC:
changing treatments and new pathological
entities. J Laparoendosc Surg 1994; 4:41-4
Need to preserve the Sphincter of Oddi
SS & ES — 9-11% stone recurrence within 6years increasing with time. Recurrent brown
stones due to stasis & infection
High rate of long term complications of ES
Resist ES without proper indication even at
expense of risk of increased complications
in the first phases of LCBDE

8/3/2019 Invited Lecture 25 ES Complications
http://slidepdf.com/reader/full/invited-lecture-25-es-complications 17/25
AND Endoscopists!Cotton P BIs your sphincterotomy really safe - and necessary?Gastrointest endosc; 1996 44:752-5
‘It could be that too many people have found themselvesinadequately trained and are stretching the indications to
maintain their experience and income’
Baillie J
Biliary sphincterotomy: less benign than once thought?curr gastroentrol rep;1999 2:102-6
‘ Endoscopists must re-evaluate their use of endoscopicsphincterotomy in light of long-term complications in thedata’

8/3/2019 Invited Lecture 25 ES Complications
http://slidepdf.com/reader/full/invited-lecture-25-es-complications 18/25
But, what about the patient ?
19 year olds having sphincterotomies
34 year old, mother of three, dying after an
ERCP for mild derangement of LFT’s
Anecdote or reality?
General ERCP mortality is NOT 0.5-1%

8/3/2019 Invited Lecture 25 ES Complications
http://slidepdf.com/reader/full/invited-lecture-25-es-complications 19/25
ES in the Laparoscopic Era
Is it any different?
What are the indications?
Perhaps there are no complications!! May be we do not hear of them!
Most do not WANT to know

8/3/2019 Invited Lecture 25 ES Complications
http://slidepdf.com/reader/full/invited-lecture-25-es-complications 20/25
Study No. Late Complications Conclusions
Boytchev
2000
169;
139 5 yr FU
14%. Late complications after ES for CBD
stones with GB in situ are rare(2%/year)Cholecystectomy does not seem to be warranted
Saito
2001
371
7.7 yr FU
Chole 5.9%, Recurr 9.7%. Long-term
outcome of ES is relatively favourable.
Cholecystectomy is not always necessary
Schreurs
2002
447
164 ES only
16%.
Sugiyama
2002
145, 60 yrs
or younger
12%. Can also be treated with ERCP. ES
is reasonable even in young patients
Costamagna
2002
529
334 5 yr FU
11%, 2.8% multiple. ES is safe at
long-term follow-up !!

8/3/2019 Invited Lecture 25 ES Complications
http://slidepdf.com/reader/full/invited-lecture-25-es-complications 21/25
No need for cholecystectomy?
Boerma et al, Lancet 2002 7;360: 739-40
Wait and see policy or laparoscopic
cholecystectomy after ES for bile duct
stones: a randomised trial.
‘ cannot be recommended as standard
treatment’

8/3/2019 Invited Lecture 25 ES Complications
http://slidepdf.com/reader/full/invited-lecture-25-es-complications 22/25
The cost of two-session management
Longer waiting
Interval complications
Multiple emergency admissions Longer presentation to resolution periods
ERCP
The economic cost can not be estimated
INCIDENCE OF REPEAT ERCP

8/3/2019 Invited Lecture 25 ES Complications
http://slidepdf.com/reader/full/invited-lecture-25-es-complications 23/25
INCIDENCE OF REPEAT ERCP
(During the same admission)
0
1000
2000
3000
4000
5000
6000
1989/90 1990/91 1991/92 1992/93 1993/94 1994/95 1995/96 1996/97 1997/98 1998/99
ERCPs (OPCS4 J38:J45) recorded in any position
ERCP as main operation with ERCP recorded also as secondary procedure

8/3/2019 Invited Lecture 25 ES Complications
http://slidepdf.com/reader/full/invited-lecture-25-es-complications 24/25
DEATHS IN ERCP FOR BENIGN GALLSTONE DISEASE
0
1
2
3
4
5
1992 1993 1994 1995 1996 1997 1998 1999 2000 2001p
E R
C P M O R T A L
I T Y ( % )

8/3/2019 Invited Lecture 25 ES Complications
http://slidepdf.com/reader/full/invited-lecture-25-es-complications 25/25
Conclusions
ES still has complications and mortality
Even if the rates are the same, 2-3 times asmany patients are exposed to the risk
Main indication in laparoscopic era!?
We should not forget the patient
Evidence for one-session management is
stronger Guidelines, Training and Specialisation