Embed Size (px)
Citation preview

Pleural effusion is a common clinicalproblem and may present to a wide rangeof specialties. Accurate aetiological diag-nosis is key to subsequent management,requiring a multidisciplinary approachand knowledge of the correct investiga-tion pathway. This article will focus onappropriate staged investigations for thepatient presenting with pleural effusionrather than on its causes or treatment.
Clinical syndromes
Pleural effusion is often detected onplain chest radiography as an incidentalfinding and patients may be asympto-
matic. Clinical symptoms are variable,depending on the size and aetiology ofthe effusion and rarely specific enough tosuggest a diagnosis in the absence of fur-ther investigations. Large effusions arelikely to be associated with dyspnoea, butthis is often a late finding and oxygen sat-urations may not be severely lowered.Dyspnoea is the result of impairedmechanics and increased intrapleuralpressure swings.
The presence of chest pain impliesinvolvement of the parietal pleura whichis heavily innervated. Inflammation,infection and malignant involvementmay produce pain, including shouldertip symptoms associated with diaphrag-matic involvement. Weight loss, anorexiaand malaise may imply malignancy orinfection (eg empyema).
Causes
Pleural effusions are divided into tran-sudative and exudative (Table 1). Theyare diagnosed according to pleural fluidbiochemical characteristics (see below).However, transudates occur with struc-turally normal pleura, in which oncoticor hydrostatic pressure results in fluidleak. In contrast, exudates occur withdamaged or altered pleura, resulting inloss of tissue fluid and protein causingfluid formation.1
Differentiation of transudate fromexudate is key to further management.Treatment for transudative effusion relieson treatment of the underlying disease,and uncommonly requires specificpleural intervention. In contrast, exuda-tive effusion usually needs further inves-tigation and often requires intervention.
Initial diagnostic approach
The presence of bilateral, symmetricaleffusions in the appropriate clinical con-text is highly suggestive of transudativeeffusion, and in general requires no fur-ther investigation.2 However, it should benoted that about 50% of heart failure
CME Respiratory medicine
174 Clinical Medicine Vol 9 No 2 April 2009
© Royal College of Physicians, 2009. All rights reserved.
NM Rahman BM BCh MA MRCP, MRC Training
Fellow and Specialist Registrar, Oxford
University, Oxford Centre for Respiratory
Medicine, Churchill Hospital, Oxford
M Munavvar MD DNB FRCP, Consultant
Chest Physician, Lancashire Teaching
Hospital NHS Foundation Trust, Preston
Clin Med 2009;9:174–8
Investigation of the
patient with pleural
effusion
Transudates Exudates
Biochemical definition
Protein <30 g/l* Protein >30 g/l*
Causes
Left ventricular failure Infection (empyema/parapneumonic effusion/TB)
Renal failure Malignancy (primary and secondary)
Liver failure Inflammation (vasculitis, autoimmiune disease)
Low protein states Pulmonary embolus (with infarction)
Oesophageal perforation
Hypothyroidism
Chylothorax/pseudochylothorax
Post-cardiac surgery
Drugs
Light’s criteria
An exudate is diagnosed if one or more of the following criteria are met:
• pleural fluid protein/serum protein >0.5
• pleural fluid LDH/serum LDH >0.6
• pleural fluid LDH more than two-thirds of the upper limit of normal serum LDH
* If pleural fluid protein is 25–35 g/l or serum protein level is abnormal, apply Light’s criteria.
LDH = lactate dehydrogenase; TB = tuberculosis.
Table 1. Causes of exudative and transudative effusions and biochemical parameters.
Unilateral pleural effusion requiresfurther aetiological investigation,with pleural fluid analysis as theusual first investigative step
All effusions in the context ofpneumonic illness should besampled to assess for the presenceof complicated parapneumoniceffusion (pH<7.2) or empyema(frank pus)
Ultrasound is a far more sensitivetechnique for the diagnosis ofpleural effusion than chestradiography. In cases where initial‘blind’ aspiration has failed, or inthe presence of an anatomicallycomplex collection, image guidance(ultrasound or computedtomography) should be sought
Drainage of undiagnosed pleuraleffusions ‘to dryness’ is notrecommended, as this makesfurther investigation techniquesmore difficult. In the case of abreathless patient, removal of1–1.5 litres of pleural fluid willusually alleviate symptoms
Pleural fluid cytology is positive inonly 60% of malignant pleuraleffusions. A negative fluid cytologyin the absence of another clearcause for pleural effusion shouldprompt further investigations via arespiratory specialist
Key Points
KEY WORDS: empyema, investigation,malignant pleural effusion, pleuralbiopsy, pleural effusion
effusions are unilateral and where bilat-eral may be larger on one side.3 In thiscircumstance or if the clinical course isatypical (eg lack of response to therapy),further investigations should be considered.
Unilateral effusions require furtherassessment. The initial investigation ofchoice is diagnostic pleural aspiration.Large effusions (>1⁄2 hemithorax volume)may be aspirated easily without imageguidance, but in the presence of a smalleffusion, or where initial ‘blind’ aspira-tion is unsuccessful, image guidance (usu-ally ultrasound) should be sought. In theabsence of a diagnosis (unless clearlyinfected), intercostal drain insertion andcomplete drainage of the chest is not recommended as this makes more difficult any further investigations thatmay be required. In symptomatic breath-lessness with large effusions, large volume(eg 1 litre) thoracentesis for diagnostic/therapeutic purposes is usually sufficientto control symptoms until initial investi-gation results are obtained. These patientscan in general be investigated in the out-patient setting.
Pleural fluid diagnostic tests
Appearance
Frankly purulent pleural fluid is diag-nostic of empyema; it may also be mal-odorous. Turbid pleural fluid may beseen in infected pleural effusion or inoesophageal perforation. ‘Milky’ pleuralfluid should prompt consideration ofempyema or a lipid abnormality.
Biochemical parameters
Fluid should be sent in all cases formeasurement of:
• protein level
• lactate dehydrogenase (LDH), and
• glucose.
These parameters allow reliable differ-entiation of exudate from transudate byapplying Light’s criteria4 (for whichsimultaneous sampling of venous bloodfor protein and LDH is required)(Table 1). Pleural fluid pH measurementis recommended in cases of suspectedinfected pleural effusion (see below).
Special tests
Guidelines recommend biochemicalanalysis of pleural fluid in all sampledeffusions as above, with microbiology(including specific requests for stainingand culture of acid-fast bacilli) andcytology where indicated.5 Certain morespecific tests should be undertaken, dic-tated by clinical circumstances, forexample:
• amylase in suspected oesophagealperforation or pancreatitis-associated effusion, or
• lipid profile in suspectedchylothorax or pseudochylothorax.
Pleural fluid autoantibody level mea-surement (eg antinuclear antibodies,rheumatoid factor) are representative ofserum levels and add little diagnosticvalue.
Radiological investigations
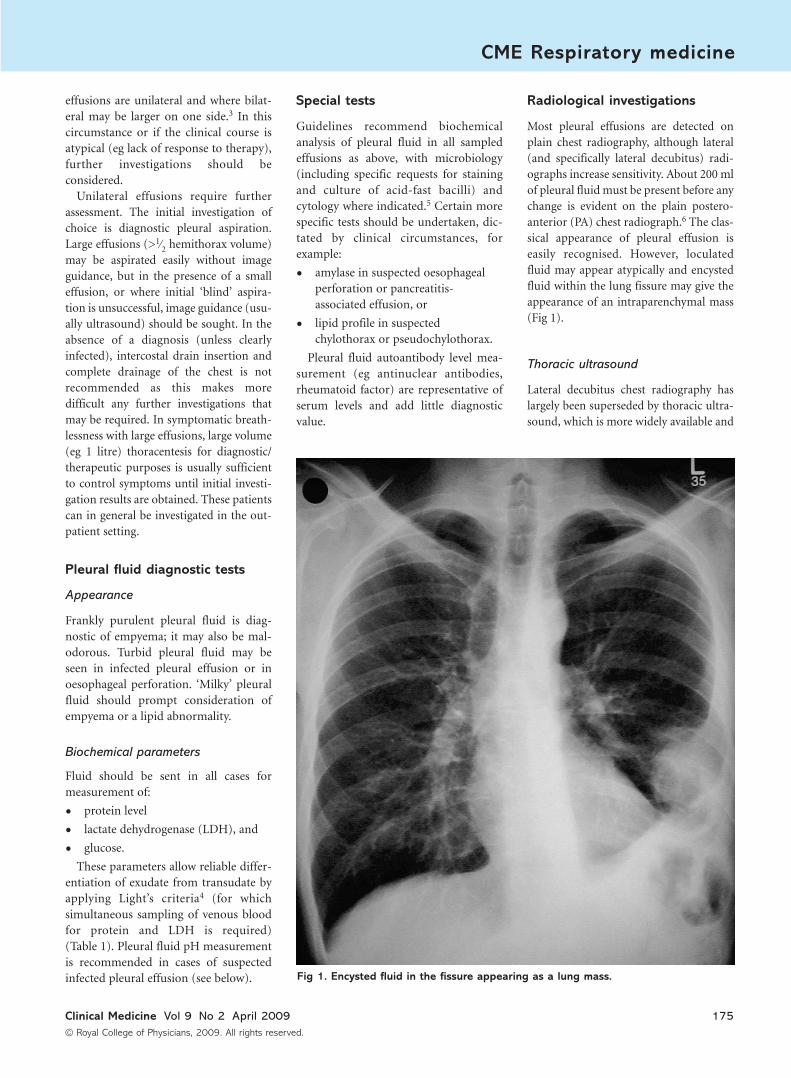
Most pleural effusions are detected onplain chest radiography, although lateral(and specifically lateral decubitus) radi-ographs increase sensitivity. About 200 mlof pleural fluid must be present before anychange is evident on the plain postero-anterior (PA) chest radiograph.6 The clas-sical appearance of pleural effusion iseasily recognised. However, loculatedfluid may appear atypically and encystedfluid within the lung fissure may give theappearance of an intraparenchymal mass(Fig 1).
Thoracic ultrasound
Lateral decubitus chest radiography haslargely been superseded by thoracic ultra-sound, which is more widely available and
CME Respiratory medicine
Clinical Medicine Vol 9 No 2 April 2009 175
© Royal College of Physicians, 2009. All rights reserved.
Fig 1. Encysted fluid in the fissure appearing as a lung mass.
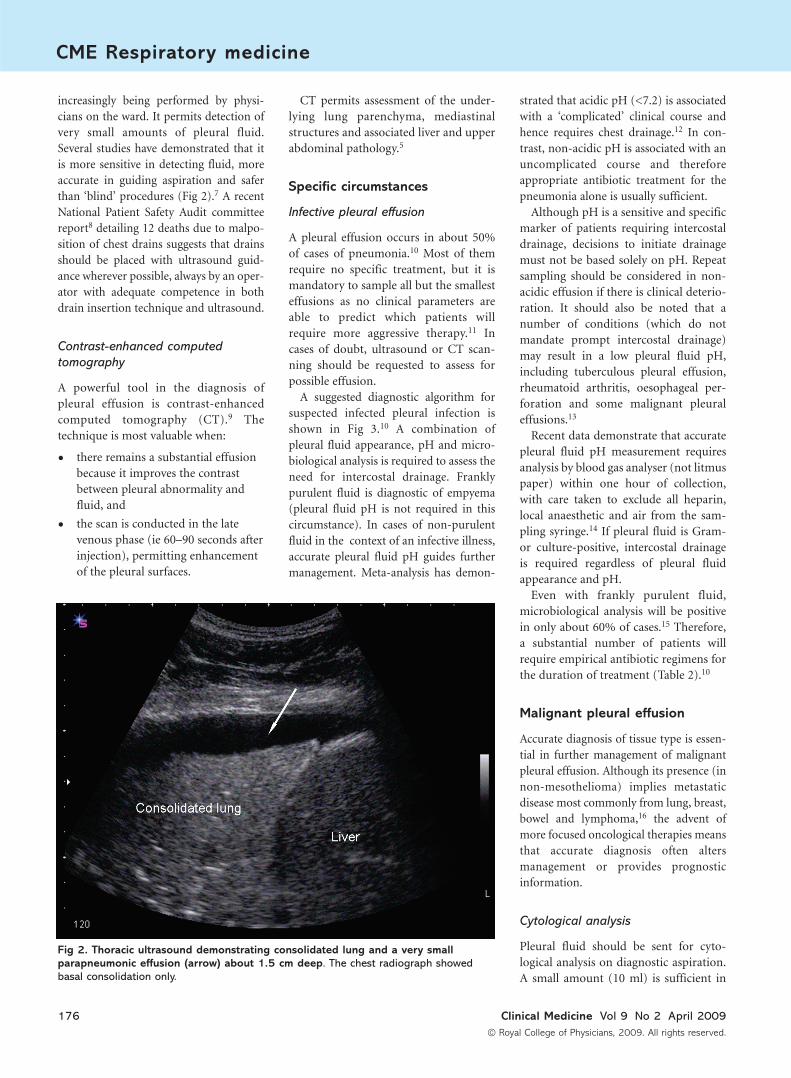
increasingly being performed by physi-cians on the ward. It permits detection ofvery small amounts of pleural fluid.Several studies have demonstrated that itis more sensitive in detecting fluid, moreaccurate in guiding aspiration and saferthan ‘blind’ procedures (Fig 2).7 A recentNational Patient Safety Audit committeereport8 detailing 12 deaths due to malpo-sition of chest drains suggests that drainsshould be placed with ultrasound guid-ance wherever possible, always by an oper-ator with adequate competence in bothdrain insertion technique and ultrasound.
Contrast-enhanced computed
tomography
A powerful tool in the diagnosis ofpleural effusion is contrast-enhancedcomputed tomography (CT).9 Thetechnique is most valuable when:
• there remains a substantial effusionbecause it improves the contrastbetween pleural abnormality andfluid, and
• the scan is conducted in the latevenous phase (ie 60–90 seconds afterinjection), permitting enhancementof the pleural surfaces.
CT permits assessment of the under-lying lung parenchyma, mediastinalstructures and associated liver and upperabdominal pathology.5
Specific circumstances
Infective pleural effusion
A pleural effusion occurs in about 50%of cases of pneumonia.10 Most of themrequire no specific treatment, but it ismandatory to sample all but the smallesteffusions as no clinical parameters areable to predict which patients willrequire more aggressive therapy.11 Incases of doubt, ultrasound or CT scan-ning should be requested to assess forpossible effusion.
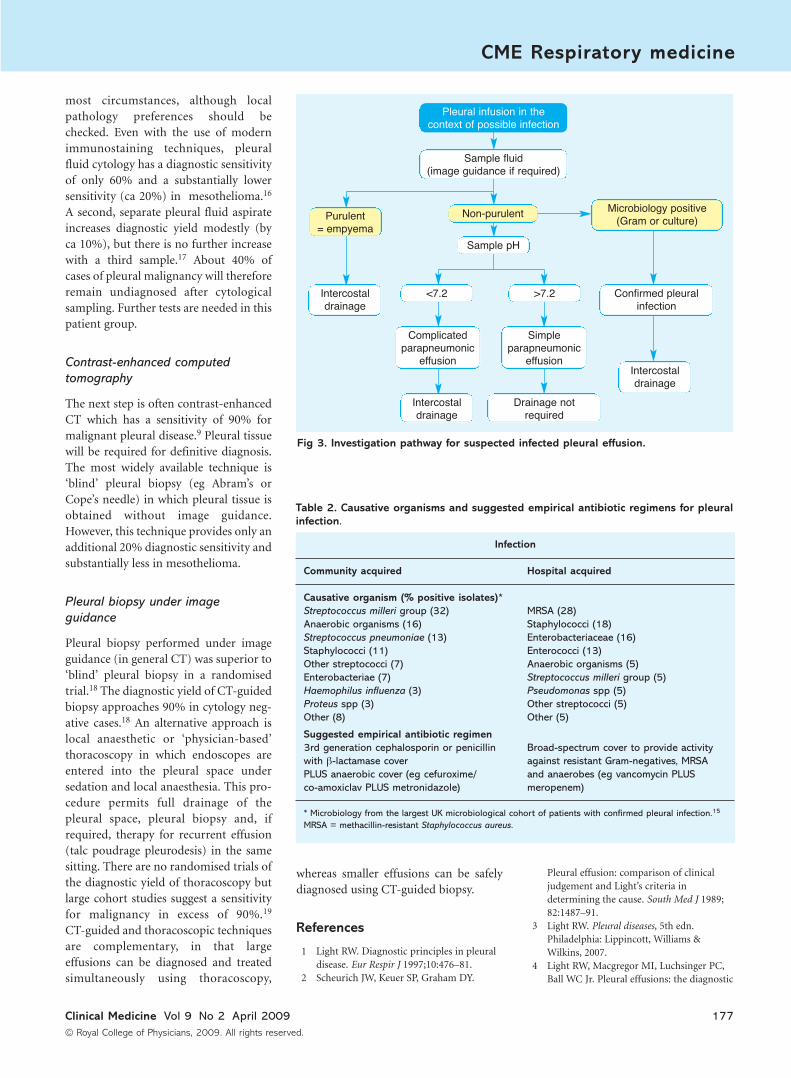
A suggested diagnostic algorithm forsuspected infected pleural infection isshown in Fig 3.10 A combination ofpleural fluid appearance, pH and micro-biological analysis is required to assess theneed for intercostal drainage. Franklypurulent fluid is diagnostic of empyema(pleural fluid pH is not required in thiscircumstance). In cases of non-purulentfluid in the context of an infective illness,accurate pleural fluid pH guides furthermanagement. Meta-analysis has demon-
strated that acidic pH (<7.2) is associatedwith a ‘complicated’ clinical course andhence requires chest drainage.12 In con-trast, non-acidic pH is associated with anuncomplicated course and thereforeappropriate antibiotic treatment for thepneumonia alone is usually sufficient.
Although pH is a sensitive and specificmarker of patients requiring intercostaldrainage, decisions to initiate drainagemust not be based solely on pH. Repeatsampling should be considered in non-acidic effusion if there is clinical deterio-ration. It should also be noted that anumber of conditions (which do notmandate prompt intercostal drainage)may result in a low pleural fluid pH,including tuberculous pleural effusion,rheumatoid arthritis, oesophageal per-foration and some malignant pleuraleffusions.13
Recent data demonstrate that accuratepleural fluid pH measurement requiresanalysis by blood gas analyser (not litmuspaper) within one hour of collection,with care taken to exclude all heparin,local anaesthetic and air from the sam-pling syringe.14 If pleural fluid is Gram-or culture-positive, intercostal drainageis required regardless of pleural fluidappearance and pH.
Even with frankly purulent fluid,microbiological analysis will be positivein only about 60% of cases.15 Therefore,a substantial number of patients willrequire empirical antibiotic regimens forthe duration of treatment (Table 2).10
Malignant pleural effusion
Accurate diagnosis of tissue type is essen-tial in further management of malignantpleural effusion. Although its presence (innon-mesothelioma) implies metastaticdisease most commonly from lung, breast,bowel and lymphoma,16 the advent ofmore focused oncological therapies meansthat accurate diagnosis often altersmanagement or provides prognosticinformation.
Cytological analysis
Pleural fluid should be sent for cyto-logical analysis on diagnostic aspiration.A small amount (10 ml) is sufficient in
CME Respiratory medicine
176 Clinical Medicine Vol 9 No 2 April 2009
© Royal College of Physicians, 2009. All rights reserved.
Fig 2. Thoracic ultrasound demonstrating consolidated lung and a very smallparapneumonic effusion (arrow) about 1.5 cm deep. The chest radiograph showedbasal consolidation only.
most circumstances, although localpathology preferences should bechecked. Even with the use of modernimmunostaining techniques, pleuralfluid cytology has a diagnostic sensitivityof only 60% and a substantially lowersensitivity (ca 20%) in mesothelioma.16
A second, separate pleural fluid aspirateincreases diagnostic yield modestly (byca 10%), but there is no further increasewith a third sample.17 About 40% ofcases of pleural malignancy will thereforeremain undiagnosed after cytologicalsampling. Further tests are needed in thispatient group.
Contrast-enhanced computed
tomography
The next step is often contrast-enhancedCT which has a sensitivity of 90% formalignant pleural disease.9 Pleural tissuewill be required for definitive diagnosis.The most widely available technique is‘blind’ pleural biopsy (eg Abram’s orCope’s needle) in which pleural tissue isobtained without image guidance.However, this technique provides only anadditional 20% diagnostic sensitivity andsubstantially less in mesothelioma.
Pleural biopsy under image
guidance
Pleural biopsy performed under imageguidance (in general CT) was superior to‘blind’ pleural biopsy in a randomisedtrial.18 The diagnostic yield of CT-guidedbiopsy approaches 90% in cytology neg-ative cases.18 An alternative approach islocal anaesthetic or ‘physician-based’thoracoscopy in which endoscopes areentered into the pleural space undersedation and local anaesthesia. This pro-cedure permits full drainage of thepleural space, pleural biopsy and, ifrequired, therapy for recurrent effusion(talc poudrage pleurodesis) in the samesitting. There are no randomised trials ofthe diagnostic yield of thoracoscopy butlarge cohort studies suggest a sensitivityfor malignancy in excess of 90%.19
CT-guided and thoracoscopic techniquesare complementary, in that largeeffusions can be diagnosed and treatedsimultaneously using thoracoscopy,
whereas smaller effusions can be safelydiagnosed using CT-guided biopsy.
References
1 Light RW. Diagnostic principles in pleuraldisease. Eur Respir J 1997;10:476–81.
2 Scheurich JW, Keuer SP, Graham DY.
Pleural effusion: comparison of clinicaljudgement and Light’s criteria indetermining the cause. South Med J 1989;82:1487–91.
3 Light RW. Pleural diseases, 5th edn.Philadelphia: Lippincott, Williams &Wilkins, 2007.
4 Light RW, Macgregor MI, Luchsinger PC,Ball WC Jr. Pleural effusions: the diagnostic
CME Respiratory medicine
Clinical Medicine Vol 9 No 2 April 2009 177
© Royal College of Physicians, 2009. All rights reserved.
Infection
Community acquired Hospital acquired
Causative organism (% positive isolates)*
Streptococcus milleri group (32) MRSA (28)
Anaerobic organisms (16) Staphylococci (18)
Streptococcus pneumoniae (13) Enterobacteriaceae (16)
Staphylococci (11) Enterococci (13)
Other streptococci (7) Anaerobic organisms (5)
Enterobacteriae (7) Streptococcus milleri group (5)
Haemophilus influenza (3) Pseudomonas spp (5)
Proteus spp (3) Other streptococci (5)
Other (8) Other (5)
Suggested empirical antibiotic regimen
3rd generation cephalosporin or penicillin Broad-spectrum cover to provide activity
with β-lactamase cover against resistant Gram-negatives, MRSA
PLUS anaerobic cover (eg cefuroxime/ and anaerobes (eg vancomycin PLUS
co-amoxiclav PLUS metronidazole) meropenem)
* Microbiology from the largest UK microbiological cohort of patients with confirmed pleural infection.15
MRSA = methacillin-resistant Staphylococcus aureus.
Table 2. Causative organisms and suggested empirical antibiotic regimens for pleuralinfection.
Fig 3. Investigation pathway for suspected infected pleural effusion.
Pleural infusion in thecontext of possible infection
Sample fluid(image guidance if required)
Sample pH
<7.2Intercostaldrainage
Intercostaldrainage
Confirmed pleuralinfection
Microbiology positive(Gram or culture)
Non-purulentPurulent= empyema
Intercostaldrainage
Drainage notrequired
>7.2
Simpleparapneumonic
effusion
Complicatedparapneumonic
effusion

separation of transudates and exudates.Ann Intern Med 1972;77:507–13.
5 Maskell NA, Butland RJ; Pleural DiseasesGroup, Standards of Care Committee,British Thoracic Society. BTS guidelines forthe investigation of a unilateral pleuraleffusion in adults. Thorax 2003;58(Suppl 2):ii8–17.
6 Blackmore CC, Black WC, Dallas RV,Crow HC. Pleural fluid volume estimation:a chest radiograph prediction rule. AcadRadiol 1996;3:103–9.
7 Diacon AH, Brutsche MH, Solér M.Accuracy of pleural puncture sites: aprospective comparison of clinicalexamination with ultrasound. Chest 2003;123:436–41.
8 Risk of chest drain insertion. NationalPatient Safety Agency, UK 2009. Available atwww.npsa.nhs.uk/nrls/alerts-and-directives/rapidrr/risks-of-chest-drain-insertion/
9 Leung AN, Müller NL, Miller RR. CT indifferential diagnosis of diffuse pleuraldisease. AJR Am J Roentgenol 1990;154:487–92.
10 Davies CW, Gleeson FV, Davies RJ; PleuralDiseases Group, Standards of Care
Committee, British Thoracic Society. BTSguidelines for the management of pleuralinfection. Thorax 2003;58(Suppl 2):ii18–28.
11 Davies CW, Kearney SE, Gleeson FV,Davies RJ. Predictors of outcome and long-term survival in patients with pleuralinfection. Am J Respir Crit Care Med 1999;160(5 Pt 1):1682–7.
12 Heffner JE, Brown LK, Barbieri C, DeLeoJM. Pleural fluid chemical analysis inparapneumonic effusions. A meta-analysis.Am J Respir Crit Care Med 1995;151:1700–8.
13 Heffner JE, Heffner JN, Brown LK.Multilevel and continuous pleural fluid pHlikelihood ratios for evaluating malignantpleural effusions. Chest 2003;123:1887–94.
14 Rahman NM, Mishra EK, Davies HE,Davies RJ, Lee YC. Clinically importantfactors influencing the diagnosticmeasurement of pleural fluid pH andglucose. Am J Respir Crit Care Med 2008;178:483–90.
15 Maskell NA, Batt S, Hedley EL et al. Thebacteriology of pleural infection by geneticand standard methods and its mortalitysignificance. Am J Respir Crit Care Med2006;174:817–23.
16 Antunes G, Neville E, Duffy J, Ali N;Pleural Diseases Group, Standards of CareCommittee, British Thoracic Society. BTSguidelines for the management ofmalignant pleural effusions. Thorax 2003;58(Suppl 2):ii29–38.
17 Garcia LW, Ducatman BS, Wang HH. Thevalue of multiple fluid specimens in thecytological diagnosis of malignancy. ModPathol 1994;7:665–8.
18 Maskell NA, Gleeson FV, Davies RJ.Standard pleural biopsy versus CT-guidedcutting-needle biopsy for diagnosis ofmalignant disease in pleural effusions: arandomised controlled trial. Lancet 2003;361:1326–30.
19 Harris RJ, Kavuru MS, Rice TW, Kirby TJ.The diagnostic and therapeutic utility ofthoracoscopy. A review. Chest 1995;108:828–41.
CME Respiratory medicine
178 Clinical Medicine Vol 9 No 2 April 2009
© Royal College of Physicians, 2009. All rights reserved.