-
7/29/2019 Investigation of Specificity of Auricular Acupuncture
Points In
1/7
Investigation of specificity of auricular acupuncture points
in
regulation of autonomic function in anesthetized rats
Xin-Yan Gao a,b, Shi-Ping Zhang a,, Bing Zhu b, Hong-Qi Zhang
a
a School of Chinese Medicine, Hong Kong Baptist University, 7
Baptist University Road, Kowloon Tong, Kowloon, Hong Kong, Chinab
Institute of Acupuncture & Moxibustion, China Academy of
Chinese Medical Sciences, Beijing, China, 100700
Received 2 August 2007; received in revised form 29 September
2007; accepted 22 October 2007
Abstract
Auricular acupuncture has been used for various autonomic
disorders in clinical practice. It has been theorized that
different auricular
areas have distinct influence on autonomic functions. The
present study aims to examine the effects of acupuncture
stimulation at different
auricular areas on cardiovascular and gastric responses. In male
SpragueDawley rats anesthetized with pentobarbital sodium, five
auricular
areas, which were located at the apex of the helix (A 1), the
middle of the helix (A2), the tail of the helix (A3), the inferior
concha (A4) and the
middle of the antihelix (A5), had been selected for stimulation
with manual acupuncture (MA) and different parameters of
electroacupuncture
(EA). A mild depressor response (6%12% decrease from baseline)
was evoked from A1, A3 and A4 by MA and from all five areas by
EA
(100 Hz1 mA). The biggest depressor response (18.4 3.1 mmHg,
pb0.001) was evoked from A4. A small bradycardia was evoked by
MA from A4 and by EA at A3, A4 and A5. Increase in intragastric
pressure (814 mmH2O) was evoked by MA from A1, A3 and A4 and by
EA at A2. These results show that similar patterns of
cardiovascular and gastric responses could be evoked by stimulation
of different areas of
the auricle. The present results do not support the theory of a
highly specific functional map in the ear. Rather, there is a
similar pattern of
autonomic changes in response to auricular acupuncture, with
variable intensity depending on the area of stimulation.
2007 Elsevier B.V. All rights reserved.
Keywords: Acupuncture; Blood pressure; Heart rate; Gastric
motility; Vagus nerve; Ear map
1. Introduction
Auricular acupuncture (AA) is the application of needle
stimulation to the external ear, which is a form of
acupuncture
practice that has been described in ancient China as well as
Egypt, Greece and Rome (Oleson, 2003a). In 1950s,
Frenchphysician Nogier reawakened the interest in AA by
proposing
a theory that there is a somatotopic and viscerotopic rep-
resentation on the auricle, such that different body regions
and organs appear on the external ear to form a humunculus
of inverted fetus (Nogier, 1987). The selection of AA point
for treatment, therefore, has been based on this theory.
Hence,
a disorder from a particular part of the body is treated by
the
corresponding point in the ear (Oleson et al., 1980; Nogier,
1987). Since then, AA has been used for pain relief
(Usichenko et al., 2005a,b; Goertz et al., 2006), anxiety
and
sleep disorders (Chen et al., 2007, Pilkington et al., 2007),
as
well as various autonomic disorders including hypertension(Huang
and Liang, 1992), gastrointestinal disorders (Taka-
hashi, 2006), lower urinary tract symptoms (Capodice et al.,
2007) and postoperative vomiting (Kim et al., 2003). How-
ever there was no scientific evidence supporting Nogier's
theory, and the specificity of AA points is still a matter
of
conjecture. This can be problematic when selecting treatment
and control points in clinic trials (e.g., Margolin et al.,
1996).
A better understanding of the specificity of auricular
points
will help to improve clinical practice and facilitate AA
research.
Autonomic Neuroscience: Basic and Clinical 138 (2008) 5056
www.elsevier.com/locate/autneu
Corresponding author. Tel.: +852 34112466; fax: +852
34112461.
E-mail address: [email protected] (S.-P. Zhang).
1566-0702/$ - see front matter 2007 Elsevier B.V. All rights
reserved.
doi:10.1016/j.autneu.2007.10.003
mailto:[email protected]://dx.doi.org/10.1016/j.autneu.2007.10.003http://dx.doi.org/10.1016/j.autneu.2007.10.003mailto:[email protected]
-
7/29/2019 Investigation of Specificity of Auricular Acupuncture
Points In
2/7
It has been documented that the human auricle receives
innervations from cervical and cranial nerves including the
auricular branch of the vagus nerve, the great auricular
nerve
and the auriculotemporal nerve (Peuker and Filler, 2002).
Study of the origin and peripheral distribution of the
primary
afferent fibers in the auricle of cats and rats showed that
innervations of the central region of the auricle mainly
came
from the trigeminal ganglion, the geniculate ganglion, the
superior ganglion of the vagus nerve, and to a lesser
degree,
the spinal ganglia. In contrast, the peripheral region of
the
auricle was mostly innervated by spinal nerves (Satomi and
Takahashi, 1991; Folan-Curran et al., 1994). The central
projections of the auricular branch of the vagus nerve, socalled
the Arnold's nerve, had been examined by the trans-
ganglionic horseradish peroxidase (HRP) tracing method in
cats. HRP-labelled neuronal somata were seen in the superior
ganglion of the vagus nerve and terminal labelling was seen
mainly in the ipsolateral solitary nucleus (Nomura and
Mizuno, 1984). Thus, in the theorized ear map, the areas
representing somatic parts such as the helix and the scapha
are mainly innervated by somatic afferents, and those rep-
resenting visceral organs such as the superior and inferior
concha are primary innervated by cranial nerves especially
the vagus nerve (Fig. 1). In human, it has been suggested
that
the sensory vagus nerve is responsible for the ear-coughreflex
seen clinically (Tekdemir et al., 1998). As well,
stimulation of the inferior concha could induce a
significant
increase in parasympathetic activity as demonstrated by
heart rate variability (Haker et al., 2000).
In the study of point specificity, Young and McCarthy
(1998) reported that stimulation of the sympathetic point at
the lower limb of the antihelix (AH6 in Fig. 1)
significantly
decreased the stimulus-evoked electrodermal response when
compared with stimulation of a controlled point in the mid-
dle of the helix (HX9 in Fig. 1). It had been found that AA
at
specific points such as Lung (CO14 in Fig. 1) and Shenmen
(TF4 in Fig. 1) produced better analgesic effect than at
non-
acupuncture points on the helix (Usichenko et al., 2005a,b).
Taken together, evidence from anatomical studies and
clinical observations suggest that there might be location
specificity for auricular points. In this study, we set out
to
examine the specificity of auricular acupuncture points in
regulation of autonomic function using gastric and cardio-
vascular changes as indicators.
2. Methods and materials
2.1. Animal preparation
The experimental protocol was approved by the animalethics
committee of the Hong Kong Baptist University.
Male SpragueDawley rats (n =18), weighing 300380 g,
were fasted overnight with free access to water. They were
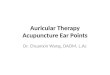
Fig. 1. Drawings showing auricular zones and nerve distribution
of the human auricle. A, auricular zones based on recommendations
of the 1990 WHO auricular
nomenclature committee (Oleson, 2003b). Large dots indicate
areas stimulated in the present study or in previous studies as
mentioned in the text. B, C and D
show nerve distribution (indicated by small dots) of the human
auricle according to Peuker and Filler (2002).
Fig. 2. Photograph of the right ear of the rat showing areas
being stimulated
in the present experiments. A1, A2, A3, A4, and A5 correspond to
HX6, HX9,
HX12, CO15, and AH9 in the human auricular map as described in
Fig. 1,
respectively.
51X.-Y. Gao et al. / Autonomic Neuroscience: Basic and Clinical
138 (2008) 5056
-
7/29/2019 Investigation of Specificity of Auricular Acupuncture
Points In
3/7
anesthetized with an initial dose of pentobarbital sodium
(i.p., 50 mg/kg, Alfasan), with i.v. supplement (1520 mg/
kg/h) via the jugular vein using a syringe pump to maintain
the level of anesthesia at a depth in which the withdrawal
reflex to a noxious toe pinch was absent. After tracheal
cannulation, animals breathed spontaneously and the core
temperature was maintained at 37.00.5 C by a feedback-
controlled electric blanket. Animals were sacrificed huma-
nely with an overdose of pentobarbital sodium at the end of
the experiments.
For recording of mean arterial pressure (MAP), the left
common carotid artery was cannulated with a polyethylene
tubing filled with normal saline containing heparin (500 IU/
ml, Sigma), and connected to a blood pressure transducer.
Needle electrodes were placed at the forelimbs and the left
hind limb for ECG recording (Bio Amp, ADInstruments),
from which heart rate (HR) was derived. For recording of
intragastric pressure (IGP), a midline laparotomy was made
with a small latitudinal incision in the duodenum wall about
23 cm from the pylorus. A balloon (1 cm in diameter) made
of flexible condom rubber was inserted into the pyloric
antrum and kept in position by tying the connecting poly-
ethylene tubing (ID 0.58 mm, OD 0.96 mm, PORTEX) to the
duodenum (Kametani et al., 1979). The balloon was filled
Fig. 3. Computer chart records of a typical experiment. Changes
in blood pressure (BP), heart rate (HR) and intragastric pressure
(IGP) during manual acupuncture
(MA) at five areas of the rat auricle are shown in the boxes.
Schematic drawing of the right ear of the rat shows the location of
the auricular areas being stimulated.
52 X.-Y. Gao et al. / Autonomic Neuroscience: Basic and Clinical
138 (2008) 5056
-
7/29/2019 Investigation of Specificity of Auricular Acupuncture
Points In
4/7
with 0.30.8 ml water pre-warmed to 37.00.5 C and kept
at a baseline pressure of 40250 mmH2O. IGP was measured
from the intragastric balloon with a transducer connecting
to
an amplifier (ADInstruments). Background gastric motility
was recorded for at least 30 min before AA stimulation.
2.2. Auricular acupuncture stimulation
When the depth of anesthesia was stable, showing that the
fluctuation of MAP and HR were less than 5% within a minuteand
the gastric peristaltic wavewas stable, responses to manual
(MA) or electroacupuncture (EA) were examined. Five
auricular areas, which were located at the apex of the helix
(A1), the middle of the helix (A2), the tail of the helix (A3),
the
inferior concha (A4) and the middle of the antihelix (A5),
corresponding to HX6, HX9, HX12, CO15, and AH9 in
human auricle respectively, were selected for MA and EA
(Figs. 1 and 2). Acupuncture needle (0.2 mm13 mm Hwato,
China) was inserted to a depth of 12 mm from the skin
surface before each stimulation. For MA, the needle was
twisted right and left once every second for 30 s and then
removed. For EA, a pair of needles was inserted into the
same
auricular area separated by approximately 1.5 mm with the
aid
of a piece of cotton wool. The EA stimulation consisted of
biphasic rectangular pulses (0.45 ms) at four different in-
tensities and frequencies: low frequencylow intensity (LL:
4 Hz0.4 mA), low frequencyhigh intensity (LH: 4 Hz
1.0 mA),high frequencylow intensity (HL: 100 Hz0.4 mA),
high frequencyhigh intensity (HH: 100 Hz1.0 mA). Eachepisode of
EA stimulation lasted for 30 s. All four parameters
of EA induced twitch of the ear, indicating effective
stimulation of auricular muscles. When tested on human
subjects, LL and HL of EA were just above the detection
threshold and were reported non-painful, whereas LH and HH
of EA were sometimes reported to be painful but tolerable
(personal observation). In a given experiment, MA and EA
were examined for different auricular areas and the stimula-
tions were arranged randomly and repeated 34 times.
2.3. Statistical analysis
Baseline values of MAP and HR were measured by taking
the average of 1 second record after needle insertion and
just
before acupuncture stimulation, when the signals were
stable.
Baseline IGP was determined by the last peak value of the
peristaltic wave just before the stimulation. Changes in MAP
and HR were measured by taking the average of a 1 second
record with the biggest change during acupuncture
stimulation,
and change of IGP was measured by selecting the highest peak
of peristaltic wave during the acupuncture stimulation
period.
Comparison between means was made by Student's-ttest and
one-way ANOVAwith LSD post-hoc test. Datawere presented
as mean S.E.M., and pb0.05 was considered significant.
3. Results
3.1. Cardiovascular and gastric responses evoked by
manual acupuncture (MA)
Data had been obtained from 12 successful experiments.
Before the start of any stimulation, the MAP was 116.4
8.9 mmHg, and the HR was 386.0 8.4 beats per minute (bpm).
As seen in Fig. 3, MA at auricular areas of A1, A3, and
A4produced significant depressor responses (8.01.6 mmHg,
7.5 2.6 mmHg and 18.4 3.1 mmHg respectively,
Fig. 4. Histograms showing mean values ( S.E.M.) of mean
arterial pressure
(MAP), heart rate (HR) andintragastric pressure (IGP) beforeand
after manual
acupuncture (MA) in five different areas of the auricle (A1-5).
*" s inside the
bars indicates statistical significant difference between pre-MA
and post-MA
(: pb0.01; : pb0.01;: pb0.001; paired t-test). #s indicates
statistical
significant differencecompared with A4 (one wayANOVAwith
LSDpost-hoc
test; #: pb0.05; ##: pb0.01; ###: pb0.001).
Fig. 5. Histograms showing the effect of needle insertion on
mean arterial
pressure (MAP). indicates statistical significant difference
between
pre- and post-insertion in MAP (pb0.001, paired t-test).
53X.-Y. Gao et al. / Autonomic Neuroscience: Basic and Clinical
138 (2008) 5056
-
7/29/2019 Investigation of Specificity of Auricular Acupuncture
Points In
5/7
pb0.05, Fig. 4), which outlasted the duration of the
stimulation.No significant change in MAP was observed during
stimulation
of A2 and A5. Changes in HR were rather variable and
statistical
difference could only be found during stimulation of A4 (4.5
1.6 bpm,pb0.05). MA also led to an increase in IGP at A1,
A3,
A4 (14.7 4.3 mmH2O, 11.9 5.5 mmH2O and 12.8
3.8 mmH2O, pb0.05, respectively). Thus, MA at A1, A3 and
A4 evoked simultaneous changes in MAP and IGP, but
simultaneous changes in MAP, and IGP as well as HR were
evoked only at A4. A4 showed the biggest depressor response
compared to other areas (pb0.01).
Interestingly, it was observed that insertion of the needle
evoked significant depressor responses at all auricular
areas
(pb0.001, Fig. 5). Compared to MA, the duration of thedepressor
responses evoked by insertion of the needle was
less than that evoked by MA, lasting for a few seconds only,
but the magnitude of the response was similar to that of
manual acupuncture. However, no significant change in HR
or IGP was observed during needle insertion.
3.2. Autonomic changes evoked by electroacupuncture (EA)
As seen in Fig. 6, of the four types of EA applied to the
five AA areas, HH evoked significant decrease in MAP
at all areas (8.8 3.7 mmHg at A1, pb0.05; 8.6
2.6 mmHg at A2, pb0.01; 9.63.5 mmHg at A3, pb0.05;
Fig. 6. Histograms showing changes in mean arterial pressure
(MAP), heart rate (HR) and intragastric pressure (IGP) for five
auricular areas (A 15) under
different parameters of electroacupuncture. LL, low frequency (4
Hz), low intensity (0.4 mA) stimulation; LH, low frequency (4 Hz),
high intensity (1 mA)
stimulation; HL, high frequency (100 Hz), low intensity (0.4 mA)
stimulation; and HH, high frequency (100 Hz), high intensity (1 mA)
stimulation. s inside
the bars indicate statistical significant change compared with
baseline (pb0.05; : pb0.01; paired t-test); #s outside the bars
indicate statistical significance
compared with HH (one way ANOVA with LSD post-hoc test; #:
pb0.05; ##: pb0.01; ###: pb0.001).
54 X.-Y. Gao et al. / Autonomic Neuroscience: Basic and Clinical
138 (2008) 5056
-
7/29/2019 Investigation of Specificity of Auricular Acupuncture
Points In
6/7
7.61.9 mmHg at A4, pb0.01 and 12.92.5 mmHg at
A5,pb0.01). HH at A3, A4 and A5 induced small bradycardia
(7.01.4 bpm, 5.7 1.7 bpm and 8.31.8 bpm respec-
tively, pb0.05), and at A2 produced significant increase in
IGP (7.6 2.4 mmH2O, pb0.05).
EA of HL evoked significant depressor effect at A3 (5.1
1.7 mmHg, pb0.05). Low frequency EA at either low (LL) orhigh
intensity (LH) did not evoke any significant change in
MAP, HR or IGP (Fig. 6).
Comparing the responses evoked by MA and EA of HH
for a given area, the overall patterns of response appeared
to
be similar, except the depressor effect produced by MA was
significantly bigger than that evoked by EA of HH at A4(pb0.01),
and the bradycardia evoked by EA of HH was
bigger than that evoked by MA at A3 (pb0.05).
4. Discussion
This is the first study that examines systematically thelocation
specificity and response characteristics of auto-
nomic changes using different methods of stimulation in
auricular acupuncture. The major finding from this study is
that stimulation of the auricle with either MA or strong EA
(100 Hz1 mA) can evoke a characteristic pattern of res-
ponse including decrease in blood pressure, bradycardia and
gastric contraction, whereas mild EA is ineffective.
Decrease
in blood pressure is the most consistent response evoked by
MA and EA. On the other hand, changes in HR and gastric
contraction are more variable, depending on the area and
method of stimulation.
Cardiac dysrhythmias and bradycardia have been re-
ported during insertion of an ear speculum and initial
ma-nipulation of the ear (Moorthy et al., 1985). Activation of
the
parasympathetic system by auricular acupuncture in man, as
measured by heart rate variability, has also been reported
before, although the same study fails to elicit any change
in
blood pressure and heart rate (Haker et al., 2000). The
observation in the current study that needle insertion,
manual
needle manipulation and strong EA are effective in evoking
autonomic responses, whereas weaker forms of EA are not,
suggest that strong or even painful stimulation may be
required to produce these responses.
In a separate series of experiments aimed to explore the
mechanism of the auricular-autonomic responses (Gao et
al.,unpublished data), we had observed that the responses
evoked
from A4 were abolished by blockade of vagal transmission
with intravenous injection of the muscarinic receptor
blocker
atropine sulphate (0.5 mg/kg). That is, before atropine
block-
ade the changes in MA, HR and IGP were16.54%,2.3
0.5% and 49.513.2%, respectively (n = 5, pb0.05, paired
t-test, compared with pre-acupuncture baseline), and after
the blockade the changes in MA, HR and IGP were 2.7
1.7%, 0.70.6% and 4.52.9%, respectively (n = 5, pN0.05,
paired t-test, compared with post-atropine, pre-acupuncture
baseline). These results suggest that the depressor
response,
bradycardia and gastric contraction induced by AA may be
due to an increase in vagal output, mediated by auricular-
vagal reflexes. In contrast, a different efferent pathway
has
been demonstrated in depressor response evoked by body
acupuncture. For example, Ohsawa et al. (1995) showed in
the rat that acupuncture-like stimulation at the hind limb
reduced renal sympathetic nerve activity coupled with the
depressor response. It is interesting to note that MA at onlyA4
of the inferior concha area evoked consistent bradycardia,
whereas MA at other areas evoked increase or decrease in
heart rate. Sato et al. (1976) reported that cutaneous
noxious
stimulation in anesthetized rats produced an increase in
heart
rate in about 70% of their tests, while in the other 30%
induced either biphasic responses or no change. Activation
of
hind limb muscle afferents in the dog was also associated
with
either increase or decrease in heart rate (Tallarida et al.,
1985).
Taken together, the inferior concha represents a distinct
region
in which decrease in heart rate could be evoked
consistently.
It has been observed that for a given area, the patterns of
response evoked by MA and EA can be different. This maybe due to
the fact that EA stimulates local receptors as well as
nerve fibers that innervate other area passing through the
area of stimulation, and that the effective stimulation area
of
EA may well exceed the area between the two inserted
needles as a result of spreading of the electrical current.
In
contrast, manual manipulation stimulates receptors primary
at the site of needle insertion. The differences in the
response
evoked by different methods of AA should be taken into
consideration in clinical practice and research.
As for the analysis of functionalanatomical relationships on
the auricle, the results obtained from MA stimulation may be
more precise, for reasons discussed above. The inferior
concha
produced the biggest depressor effect during MA in the
presentexperiments, andit was the only site where bradycardia could
be
elicited. This coincides with previous findings that the
conchae
receives major innervations from the auricular branch of the
vagus nerve (Fig. 1). However, apart from the inferior
concha,
the areas in which depressor response and gastric
contraction
have been elicited by MA in the current experiments include
the
apex of the helix and tail of the helix, which are
innervated
predominately by the auriculotemporal nerve and the great
auricular nerve, respectively. This indicates that the
hypotensive
and gastric responses are not elicited solely from areas in-
nervated by the vagus nerve. This is in agreement with
previous
findings that denervation of the auricular branch of the
vagusnerve did not abolish gastric response evoked by auricular
acupuncture in the rabbit, but complete denervation of all
the
nerves tothe ear did (Liu et al., 1990). Taken together, it
appears
that the AA-evoked autonomic responses are mediated by the
auricular branch of the vagus nerve, as well as other
sensory
nerves innervating the ear.
Direct vagal nerve stimulation has been used in clinical
practice for treatment of refractory epilepsy and major
depres-
sion (Shafique and Dalsing, 2006). Recently, Kraus et al
(2007)
showed that non-invasive electrical stimulation of the outer
auditory canal, aiming to activate vagal afferences,
produced
enhancement of well-being score coupled with deactivation of
55X.-Y. Gao et al. / Autonomic Neuroscience: Basic and Clinical
138 (2008) 5056
-
7/29/2019 Investigation of Specificity of Auricular Acupuncture
Points In
7/7
limbic and temporal brain structures, whereas stimulation of
the
ear lobe did not. It is interesting to note that AA point
Heart
(CO15 in Fig. 1 or A4 in Fig. 2) in the inferior concha has
also
been used for mood disorders in clinical practice
(Pilkington
et al., 2007; Wang et al., 2001). Taken together, convergent
evidence supports that the concept that vagal afferents on
the
auricle provide a unique situation whereby autonomic and
othernervous disorders may be corrected with the use of
appropriate
stimulation, such as acupuncture.
5. Conclusions
Previous schemas of auricular acupuncture suggest that
auricular points have high specificity. On the other hand,
anatomical studies of auricular innervations have described
an overlapping network of distribution of somatic and
cranial
nerves, although some areas do receive preferential innerva-
tions from one or two nerves. Our experiments show that the
same pattern of reflex responses can be elicited from dif-ferent
areas with supposedly distinct nerve innervations.
Taken together, evidence from anatomical and physiological
studies does not support the concept of a highly specific
functional map in the ear. Rather, there is a general
pattern
of autonomic changes in response to auricular acupuncture,
with variable intensity depending on the area of
stimulation.
Our study suggests that the inferior concha is the most
powerful site for regulation of autonomic functions. How-
ever, in clinical study, it should be cautious in using
auricular
points outside the conchae as control points, as they also
have the potential to influence autonomic functions.
Acknowledgements
Dr. Xin-Yan Gao is supported by the Wofoo Postdoctoral
Fellowship Scheme of Chinese Medicine from the Hong
Kong Baptist University. The technical assistance of Miss
Nickie Chan is appreciated.
References
Capodice, J.L., Jin, Z., Bemis, D.L., Samadi, D., Stone, B.A.,
Kapan, S., Katz,
A.E., 2007. A pilot study on acupuncture for lower urinary tract
symptoms
related to chronic prostatitis/chronic pelvic pain. Chin. Med.
2, 1.
Chen, H.Y., Shi, Y., Ng, C.S., Chan, S.M., Yung, K.K., Zhang,
Q.L., 2007.
Auricular acupuncture treatment for insomnia: a systematic
review.
J. Altern. Complement. Med. 13, 669676.Folan-Curran, J., Hickey,
K., Monkhouse, W.S., 1994. Innervation of the rat
external auditory meatus: a retrograde tracing study.
Somatosens. Motor
Res. 11, 6568.
Goertz, C.M., Niemtzow, R., Burns, S.M., Fritts, M.J., Crawford,
C.C.,
Jonas, W.B., 2006. Auricular acupuncture in the treatment of
acute pain
syndromes: A pilot study. Mil. Med. 171, 10101014.
Haker, E., Egekvist, H., Bjerring, P., 2000. Effect of sensory
stimulation
(acupuncture) on sympathetic and parasympathetic activities in
healthy
subjects. J. Auton. Nerv. Syst. 79, 5259.
Huang, H., Liang, S., 1992. Acupuncture at otoacupoint heart for
treatment
of vascular hypertension. J. Tradit. Chin. Med. 12, 133136.
Kametani, H., Sato, A., Sato, Y., Simpson, A., 1979. Neural
mechanisms of
reflex facilitation and inhibition of gastric motility to
stimulation of
various skin areas in rats. J. Physiol. 294, 407418.
Kim, Y., Kim, C.W., Kim, K.S., 2003. Clinical observations on
post-
operative vomiting treated by auricular acupuncture. Am. J.
Chin. Med.
31, 475480.
Kraus, T., Hsl, K., Kiess, O., Schanze, A., Kornhuber, J.,
Forster, C., 2007.
BOLD fMRI deactivation of limbic and temporal brain structures
and
mood enhancing effect by transcutaneous vagus nerve
stimulation.
J. Neural Transm. 114 (11), 14851493.
Liu, W.Z., Xu, G.S., Jiang, W.F., 1990. An approach to mechanism
offunction of auricular point. Zhenci Yanjiu 15, 187190.
Margolin, A., Avants, S.K., Birch, S., Falk, C.X., Kleber, H.D.,
1996.
Methodological investigations for a multisite trial of
auricular
acupuncture for cocaine addiction: a study of active and
control
auricular zones. J. Subst. Abuse Treat. 13, 471481.
Moorthy, S.S., Krishna, G., Elliott, C.L., 1985. Is there an
auriculovagal
reflex producing cardiac dysrhythmias? Arch. Otolaryngol. 111,
631.
Nogier, P., 1987. Points Reflexes Auriculares. Moulins-les-Metz,
Maison-
neuve, France.
Nomura, S., Mizuno, N., 1984. Central distribution of primary
afferent fibers
in the Arnold's nerve (the auricular branch of the vagus
nerve):
a transganglionic HRP study in the cat. Brain Res. 292,
199205.
Ohsawa, H., Okada, K., Nishijo, K., Sato, Y., 1995. Neural
mechanism of
depressor responses of arterial pressure elicited by
acupuncture-like
stimulationto a hindlimb in anesthetized rats. J. Auton.Nerv.
Syst. 51,2735.Oleson, T., 2003a. Overview and history of
auriculotherapy, In: Oleson, T. (Ed.),
Auriculotherapy Manual: Chinese and Western Systemsof Ear
Acupuncture,
3rd ed. Churchill Livingstone, London, p. 2.
Oleson, T., 2003b. Auricular zones, In: Oleson, T. (Ed.),
Auriculotherapy
Manual: Chinese and Western Systems of Ear Acupuncture, 3rd
ed.
Churchill Livingstone, London, p. 104.
Oleson, T.D., Kroening, R.J., Bresler, D.E., 1980. An
experimental
evaluation of auricular diagnosis: the somatotopic mapping
or
musculoskeletal pain at ear acupuncture points. Pain 8,
217229.
Peuker, E.T., Filler, T.J., 2002. The nerve supply of the human
auricle. Clin.
Anat. 15, 3537.
Pilkington, K., Kirkwood, G., Rampes, H., Cummings, M.,
Richardson, J.,
2007. Acupuncture for anxiety and anxiety disordersa
systematic
literature review. Acupunct. Med. 25, 110.
Sato, A., Sato, Y., Shimada, F., Torigata, Y., 1976. Varying
changes in heartrate produced by nociceptive stimulation of the
skin in rats at different
temperatures. Brain Res. 110, 301311.
Satomi, H., Takahashi, K., 1991. Distribution of the cells of
primary afferent
fibers to the cat auricle in relation to the innervated region.
Anat. Anz.
173, 107112.
Shafique, S., Dalsing, M.C., 2006. Vagus nerve stimulation
therapy for
treatment of drug-resistant epilepsy and depression. Perspect.
Vasc.
Surg. Endovasc. Ther. 18, 323327.
Takahashi, T., 2006. Acupuncture for functional gastrointestinal
disorders.
J. Gastroenterol. 41, 408417.
Tallarida, G., Baldoni, F., Peruzzi, G., Raimondi, G., Di Nardo,
P.,
Massaro, M., Visigalli, G., Franconi, G., Sangiorgi, M., 1985.
Car-
diorespiratory reflexes from muscles during dynamic and
static
exercise in the dog. J. Appl. Physiol. 58, 844852.
Tekdemir, I., Aslan, A., Elhan, A., 1998. A clinico-anatomic
study of theauricular branch of the vagus nerve and Arnold's
ear-cough reflex. Surg.
Radiol. Anat. 20, 253257.
Usichenko, T.I., Dinse, M., Hermsen, M., Witstruck, T.,
Pavlovic, D.,
Lehmann, C., 2005a. Auricular acupuncture for pain relief after
total hip
arthroplastya randomized controlled study. Pain 114, 320327.
Usichenko, T.I., Hermsen, M., Witstruck, T., Hofer, A.,
Pavlovic, D.,
Lehmann, C., Feyerherd, F., 2005b. Auricular acupuncture for
pain relief
after ambulatory knee arthroscopy: a pilot study. Evid.
Based
Complement Alternat. Med. 2, 185189.
Wang, S.M., Peloquin, C., Kain, Z.N., 2001. The use of auricular
acupuncture
to reduce preoperative anxiety. Anesth. Analg. 93, 11781180.
Young, M.F., McCarthy, P.W., 1998. Effect of acupuncture
stimulation of the
auricular sympathetic point on evoked sudomotor response. J.
Altern.
Complement. Med. 4, 2938.
56 X.-Y. Gao et al. / Autonomic Neuroscience: Basic and Clinical
138 (2008) 5056