Embed Size (px)
Citation preview

Investigation of a cluster of children with Down’ssyndrome born to mothers who had attended aschool in Dundalk, Ireland
G Dean, N C Nevin, M Mikkelsen, G Karadima, M B Petersen, M Kelly, J O’Sullivan
AbstractObjectives—To investigate a reportedcluster of Down’s syndrome in oVspring offormer pupils of a girls’ school in Ireland,to establish the prevalence of Down’s syn-drome among live births in the areaaround the school, and to review theliterature on the possible causes of re-ported clusters of Down’s syndrome.Methods—Questionnaire survey of obstet-ric and personal histories of women whohad attended the girls’ school at Dundalk,County Louth, Republic of Ireland, atsome time during 1956–7, and also ofwomen who had attended another, nearby,girls’ school during the same period.Comparison of observed numbers of casesof Down’s syndrome identified by thesesurveys with maternal age adjusted ex-pected numbers for the reported livebirths. Laboratory tests were conducted toverify and characterise the cases ofDown’s syndrome constituting the cluster.Retrospective collection and collation ofdata on Down’s syndrome occurringamong live births, and the compilation ofmaternal age specific incidences, inCounty Louth and in Newry and MourneDistrict in neighbouring Northern Ire-land, during 1961–80. These rates werecompared with reference rates and ratesfor other areas of Ireland.Results—Six children with Down’s syn-drome were confirmed among 387 reportedlive births to women who had been pupils atthe girls’ school in Dundalk during 1956–7,compared with 0.69 expected (nominalp<10-4). Five of the aVected births were tomothers under 30 years of age, against 0.15expected (nominal p<10-6), although onlyfour of these mothers were attending theschool at any one time. The origin of thenon-disjunction was found to be maternalfirst meiotic in four children, mitotic afterfertilisation in another (with the youngestmother), and in the remaining one couldnot be determined. The marked excess ofDown’s syndrome in births to young moth-ers did not extend to oVspring of formerpupils of the other Dundalk girls’ schoolsurveyed, or to live births in County Louthgenerally or in adjacent Newry and MourneDistrict.Conclusion—A striking, highly localised,excess of Down’s syndrome in births toyoung mothers who had attended a girls’school in Dundalk during 1956–57 hasbeen confirmed. However, not all of the
mothers of the aVected children attendedthe school concurrently and the origin ofnon-disjunction in one child was an erroroccurring after conception. Some expo-sure essentially confined to girls attendingthe school at this time is a possible,although unlikely, explanation, but a re-view of potential risk factors does not sug-gest what this could be. Previoussuggestions that an influenza epidemic orcontamination from the Windscale nu-clear reactor fire might be implicated,both of which occurred in October 1957,can be eVectively dismissed because threeof the women with aVected oVspring hadleft the school by then and had movedaway from Dundalk, and Down’s syn-drome in the child of another motheroriginated in an error after fertilisation.Owing to the retrospective nature of theinvestigation and the characteristics of thecases, chance is the most likely explana-tion for the cluster.(Occup Environ Med 2000;57:793–804)
Keywords: Down’s syndrome; cluster; maternal expo-sure
In 1983, Sheehan and Hillary1 reported thepreliminary findings of an investigation into anunusual space-time cluster of six cases ofDown’s syndrome associated with a small girls’school in the town of Dundalk, County Louth,in the northeast of the Republic of Ireland. Thecluster was characterised by births to youngmothers who had attended the school duringthe 1950s and the authors proposed that someexposure of the mothers while pupils at theschool could be responsible for this unusualaggregation of births with Down’s syndrome.In subsequent correspondence, Sheehan andHillary2 reported that they had learnt of a fur-ther two babies with Down’s syndrome born tothese mothers, bringing the number of casesconstituting the cluster to eight, which com-pares with an estimate of less than oneexpected.3
Sheehan and Hillary1 suggested that an out-break of illness similar to influenza thatoccurred at the school in October 1957 mightbe relevant. However, the testing of serumsamples from the mothers of the original sixaVected children, from former pupils of thisand two other schools and from similarly agedmothers of children with Down’s syndrome inIreland, for antibodies to several strains ofinfluenza and other infectious agents, showednothing unusual.1 The authors further sug-
Occup Environ Med 2000;57:793–804 793
Medico-SocialResearch Board (nowThe Health ResearchBoard), 73 LowerBaggot Street, Dublin2, IrelandG Dean (emeritus)
Department ofMedical Genetics, TheQueen’s University ofBelfast, Belfast CityHospital, LisburnRoad, Belfast,BT9 7AB, NorthernIreland, UKN C Nevin
John F KennedyInstitute, Gl Landevej7, DK-2600, Glostrup,DenmarkM MikkelsenM B Petersen
Department ofGenetics, Institute ofChild Health, Athens,GreeceG KaradimaM B Petersen
Bawnmore, Limerick,Ireland, and St John ofGod’s, Drumcar,County Louth, IrelandM Kelly
Our Lady of Lourdes’Hospital, Drogheda,County Louth, IrelandJ O’Sullivan
Correspondence to:Dr G [email protected]
Accepted 25 July 2000
www.occenvmed.com
on July 28, 2021 by guest. Protected by copyright.
http://oem.bm
j.com/
Occup E
nviron Med: first published as 10.1136/oem
.57.12.793 on 1 Decem
ber 2000. Dow
nloaded from
on July 28, 2021 by guest. Protected by copyright.
http://oem.bm
j.com/
Occup E
nviron Med: first published as 10.1136/oem
.57.12.793 on 1 Decem
ber 2000. Dow
nloaded from
on July 28, 2021 by guest. Protected by copyright.
http://oem.bm
j.com/
Occup E
nviron Med: first published as 10.1136/oem
.57.12.793 on 1 Decem
ber 2000. Dow
nloaded from

gested1 that radioactive contamination fromthe fire (the Windscale fire) in October 1957 atthe Windscale No 1 Pile, a nuclear reactor atSellafield in northwest England, could be apossible factor. In subsequent correspon-dence3 4 it was pointed out that fallout from thisfire did not make a significant contribution tothe radiation exposure of the population ofeither Dundalk in particular or Ireland in gen-eral, and that evidence that exposure toionising radiation increases the risk of Down’ssyndrome in oVspring is weak. However, Sharpand McConnell3 concluded that the cluster wasa suYciently unusual occurrence that alterna-tive explanations should be examined. Theexistence of the cluster has been widelyreported in the media.
Sheehan continued her investigation of thiscluster, but did not publish any further findingsin the scientific literature before her death in1994. One of us (GD) has been given access toSheehan’s papers so that additional data fromher study of the cluster could be collated andanalysed. Also, data on the incidence ofDown’s syndrome in Dundalk and its generalvicinity have been collected to assess whetherthe cluster is part of a broader phenomenon. Inthis paper we report the results of this work. Wealso review the literature on what is known ofthe causes of Down’s syndrome.
MethodsQUESTIONNAIRE SURVEY
A remark in 1974 by the mother of a child withDown’s syndrome about the number of herschoolfriends with similarly aVected childrenled Sheehan to contact women whom she hadidentified as attending St Louis’ SecondarySchool for Girls in Dundalk at some timebetween September 1951 and June 1961.1 2 StLouis’ School was a small convent secondaryschool situated on the outskirts of Dundalk,attended by girls aged 11–18 years, whichopened for day pupils in 1950 and for boardersin 1953. After the publication of the prelimi-nary findings about the cluster, in 1987Sheehan issued a questionnaire, enquiringabout obstetric and personal histories, to 178women whom she had identified from schoolexamination rolls and dates of birth as attend-ing St Louis’ School during the years 1956 and1957. Presumably, this period was chosenbecause the cases of Down’s syndrome hadbeen found from her initial enquiries to beconcentrated among births to mothers whohad attended the school at some time in these2 years. A questionnaire was also sent by DrSheehan to each of the 671 women whom shehad similarly identified as attending a dayschool for girls aged 5–18 years in Dundalk (StVincent’s School, the largest girls’ school in thetown) during 1956–7. The questionnaire phaseof the study was closed at the end of 1988 andno results have been reported in the scientificliterature.
LABORATORY TESTS
Owing to the potential importance of the clus-ter of eight births with Down’s syndromereported to be associated with St Louis’
School, checks were made on the identificationand diagnosis of these children, and oninformation about maternal attendance at theschool during the 1950s. One of us (GD), withthe cooperation of St Louis’ School, checkedthe details of the mothers contained inSheehan’s documents against school records.Another of us (MM) had collaborated withSheehan in a cytogenetic analysis of peripheralblood lymphocytes sampled from the fiveaVected children who were alive in 1984 toconfirm Down’s syndrome. (One of these fivedied at the age of 19 years in 1985.) Blood hadalso been sampled from the parents, so thatchromosomal fluorescence heteromorphisms(method described by Mikkelsen et al5) couldbe used to find the origin of the supernumerarychromosome 21 and the meiotic stage ofgametogenesis of the non-disjunction that ledto trisomy in the child. The results of this cyto-genetic analysis have not been previouslyreported. More recently, the four survivingchildren and their parents have providedfurther biological samples, in all but oneinstance blood, the exception being a buccalsmear from one of the fathers. Also, an infantwho was subsequently reported2 as aVectedwith Down’s syndrome and who died at the ageof 8 weeks had had a necropsy, and blocks hadbeen kept; we were given access to thismaterial, and the parents provided blood sam-ples. Thus, biological material was availablefrom five aVected people and their parents foranalysis for DNA polymorphisms to find theparental origin of the non-disjunction. Micros-atellite DNA polymorphisms spanning theentire 21q were detected after polymerasechain reaction (PCR) amplification of genomicDNA.6 The 12 polymorphisms studied werethe short sequence repeats at loci D21S369,D21S215, D21S258, D21S16, D21S11,D21S214, D21S210, D21S213, HMG14,D21S212, D21S171, D21S1575. Amplifica-tion of the PCR with end labelling of primers,polyacrylamide gel electrophoresis of the am-plification products, and autoradiography wereperformed as described by Petersen et al.7 Allloci have been localised on the genetic linkagemap of human chromosome 21.8 The parentalorigin of the extra chromosome 21 was foundby dose analysis when two diVerent alleles werepresent in the proband, or by scoring the poly-morphic alleles when three diVerent alleleswere present.9 The meiotic stage of non-disjunction (meiosis i or ii) was assigned on thebasis of reduction to homozygosity at the fourpericentromeric 21q loci.10 A mitotic error afterfertilisation was assumed when pericentro-meric markers were reduced to homozygosityand there was lack of recombination along theentire 21q.11
DOWN’S SYNDROME IN COUNTY LOUTH
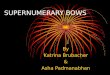
County Louth (population 67 378 at the 1961census) has two main towns, Dundalk (1961population 19 790) in the north of the countyand Drogheda (1961 population 17 085) in thesouth (figure). Louth County Hospital islocated in Dundalk and Our Lady of Lourdes’Hospital in Drogheda. One of us (JO’S) was a
794 Dean, Nevin, Mikkelsen, et al
www.occenvmed.com
on July 28, 2021 by guest. Protected by copyright.
http://oem.bm
j.com/
Occup E
nviron Med: first published as 10.1136/oem
.57.12.793 on 1 Decem
ber 2000. Dow
nloaded from

paediatrician at Our Lady of Lourdes’ Hospitalwhere most babies with Down’s syndromeborn to mothers resident in County Louthwould have been examined, as until recentlythere was no paediatrician at Louth CountyHospital. Down’s syndrome among live birthsbetween 1961 and 1980 to mothers who werenormally resident in County Louth was of spe-cific interest because of the possibility of someexposure of the mothers, as schoolgirls, in1956–7. These cases were identified from sev-eral sources: the register of the handicapped;hospital records in Dundalk and Drogheda, inNewry and Kilkeel in adjacent NorthernIreland, and in Dublin; and, since people withDown’s syndrome could have died in infancy,death registers. Other sources of informationwere a major centre for the care of the mentallyhandicapped, St John of God’s, at Drumcar,County Louth (where one of us (MK) wasbased); the Foundation for the Prevention ofChildhood Handicap; the Down’s SyndromeAssociation of Ireland; and the records of thecytogenetics laboratories at University CollegeDublin and University College Galway. For themothers of aVected children, maiden nameswere obtained from hospital and birth registersand ages at birth from hospital records, andthis information was compared with details ofgirls who had attended St Louis’ School or StVincent’s School. The maternal age profile ofall live births to women resident in CountyLouth during 1961–80 is available for eachyear from the Central Statistics OYce, butbirth data were not routinely collated forsmaller geographical units within CountyLouth. There is no prenatal testing for Down’ssyndrome in the Republic of Ireland, and so
induced abortion does not influence the preva-lence of Down’s syndrome among live births.
DOWN’S SYNDROME IN NEWRY AND MOURNE
DISTRICT
Owing to the closeness of Dundalk to North-ern Ireland, data on incidence of Down’ssyndrome for the district of Northern Irelandadjacent to County Louth, Newry and MourneDistrict (figure), were also collected andcollated for the period 1961–80. Newry andMourne District was created in 1974 from sixlocal authority areas and the population of thedistrict at the 1981 census was 79 205. Themain town, Newry (1981 population 20 554),contains the principal hospital serving the dis-trict (Daisy Hill Hospital) and a small privatehospital, and a small hospital is also located atKilkeel. Another hospital in Newry (NewryGeneral Hospital) closed in 1975 and many ofthe medical records were destroyed. A registerof congenital abnormalities among births towomen resident in Northern Ireland has beenmaintained in Belfast by one of us (NN) since1970.12 Down’s syndrome in births to womennormally resident in Newry and MourneDistrict were identified from this register.Down’s syndrome in births in this districtbefore 1970 were identified from hospitalrecords, registers of deaths, records of thehandicapped, and those of the Down’s Syn-drome Association of Northern Ireland,records of the cytogenetics laboratory inBelfast, a survey of Down’s syndrome inNorthern Ireland carried out by the Institutefor Counselling and Personal Development,and general practitioners. As the congenitalabnormalities register in Belfast may not havebeen complete in the early years of its existencethese sources of information were also used tocross check against the registry data for theperiod from 1970. Prenatal diagnosis and sub-sequent induced abortion is practised inNorthern Ireland and account must be taken ofsuch cases to allow a proper comparison withprevalences of Down’s syndrome among livebirths in the Republic of Ireland. Therefore,records at Belfast were checked by one of us(NN) to identify any such instances amongwomen living in Newry and Mourne District.As for County Louth, maiden names and agesat birth of mothers of children with Down’ssyndrome from Newry and Mourne Districtwere obtained from birth and hospital regis-ters. This information was checked against theschool roll of St Louis’ School.
The maternal age structure of all live birthsto mothers resident in Newry and MourneDistrict is readily available for 1974 onwardsfrom computerised records held by the Regis-trar General’s OYce, but no easily accessiblesource of such information exists for the yearsbefore 1974. As a consequence, records for alllive births in three hospitals in Newry andMourne District during the years 1961, 1966,and 1970 were examined to obtain maternalages. It was assumed that the annual propor-tions of these births by maternal age groupvaried linearly between the years sampled.These annual proportions were then applied to
Map showing County Louth, Republic of Ireland, and Newry and Mourne District,Northern Ireland, and the location of the major towns in these two areas.
Northern Ireland
Newry and Mourne District
County Louth
Newry
Kilkeel
Dundalk
Drogheda
Irish Sea
Republic of Ireland
Cluster of Down’s syndrome 795
www.occenvmed.com
on July 28, 2021 by guest. Protected by copyright.
http://oem.bm
j.com/
Occup E
nviron Med: first published as 10.1136/oem
.57.12.793 on 1 Decem
ber 2000. Dow
nloaded from

the annual total number of live births in theDistrict for each year during 1961–70, theannual numbers of live births being estimatedfrom those for the constituent local authorityareas on advice from the Registrar General’sOYce. The maternal age distribution for 1970and that for 1974 were used to similarly obtain,through linear interpolation of proportions ofbirths by age group, the annual maternal agestructure of all live births during 1971–3.Together with the exact number of births ineach maternal age group for 1974–80, this pro-cedure allowed the maternal age distributionfor all live births during 1961–80 in Newry andMourne District to be estimated.
ANALYSIS
Observed numbers of cases of Down’s syn-drome were compared with maternal ageadjusted expected numbers. These expectednumbers are the sum of maternal age specificexpected numbers, generated from the mater-nal age specific reference rates for the preva-lence of Down’s syndrome among live birthspresented by Cuckle et al.13 The significance ofany excess of observed over expected numberswas found from the Poisson distribution.Significance values relating to the previouslyreported cluster are nominal because compari-sons were not identified initially.
ResultsQUESTIONNAIRE SURVEY
Of the 178 questionnaires issued by Sheehan towomen who had been pupils at St Louis’School, Dundalk, during the years 1956 and1957, 159 (89%) were completed and re-turned. Among the 387 live births identified inthese questionnaires were five with Down’ssyndrome included in the original report ofSheehan and Hillary1; but the mother of thesixth child with Down’s syndrome presented inthis original report1 was found not to haveattended St Louis’ School. She was a pupil at aprimary day school, Scoil Muire gan Smál(School of the Immaculate Conception), whichwas under the aegis of the St Louis’ Order andwas situated about 1 km away from thesecondary school. Questionnaires had not beensent to mothers who had been pupils at thisprimary school unless they had also attendedSt Louis’ School during 1956–7. Conse-quently, this sixth child with Down’s syndromeshould not be included in the cohort of
children identified through the questionnairessent to the specific group of past pupils of StLouis’ School.
Two further cases of Down’s syndrome werereported2 to have occurred among the oVspringof former pupils of St Louis’ School. Both ofthese children were reported2 to have died. Acompleted questionnaire was obtained for themother of one of these children who had beendiagnosed with Down’s syndrome and haddied in infancy. On investigation, the otherchild was found not to have died and not tohave Down’s syndrome. This child may havebeen confused with a relative with Down’s syn-drome born about the same time.
Details of the six cases of Down’s syndrome,identified by the questionnaires as occurringamong children whose mothers attended StLouis’ School during 1956–7, are given in table1. The aVected children were born between1963 and 1972, and the births showed no ten-dency to occur at any particular time or place(table 1). The maternal age at birth was under30 years in all but one instance, the exceptionbeing a mother who was 31 years of age at thetime of the birth. Four of the mothers wereboarders and two were day pupils at St Louis’School, which is not especially unusual sincebetween 35% and 40% of girls attending thisschool during the 1950s were boarders.
LABORATORY TESTS
Five of the aVected children and their parentshad previously been karyotyped by one of us(MM), and the results are presented in table 2.Primary trisomy 21 was found in all five cases.Samples from four of these five families wereavailable for DNA analysis together with a fur-ther family not previously studied, where thechild had died shortly after birth and necropsymaterial was obtained. The conclusions on theorigin of the non-disjunction derived from thelaboratory analyses are presented in table 2.(Full details of the DNA polymorphismresults, obtained as described in the methodssection, can be obtained from one of us(MBP).) Four of the six cases were the result ofan error in the first maternal meiotic division.In a further case, chromosome analysis of cyto-genetic heteromorphisms had originally as-signed the error to the second maternal meioticdivision, but DNA analysis showed a mitoticevent after fertilisation involving the maternallyderived chromosome. The study of cytogenetic
Table 1 Details of Down’s syndrome births to mothers who had attended St Louis’ Secondary School, Dundalk, during 1956–7, as obtained fromcompleted questionnaires
Caseidentifier† Sex
Date of birth(month/y) Place of birth Parity
Maternalage (y)
Paternalage (y)
Period at StLouis’ SecondarySchool (month/y) Comment
1 F 6/63 Newtownards, NorthernIreland
1 21 27 9/54–6/59 Boarder
2 M 10/64 New York 1 26 33 9/54–6/56 Boarder3* M 5/65 Drogheda 1 26 35 9/52–6/57 Day girl
Child died aged 8 weeks (necropsy carried out).4 F 3/66 Dublin 1 26 27 9/52–6/57 Day girl
Child died aged 19 years (no necropsy).5 M 5/70 Dublin 1 26 25 9/56–6/62 Boarder6 M 12/72 Drogheda 3 31 34 9/55–6/59 Boarder
*Not in original report,1 but identified subsequently.2
†Not included in this table are one child with Down syndrome who was included in the original report1 but whose mother was found not to have attended St Louis’Secondary School, and one child subsequently reported2 as aVected with Down syndrome who was found not to be so aVected (see text).
796 Dean, Nevin, Mikkelsen, et al
www.occenvmed.com
on July 28, 2021 by guest. Protected by copyright.
http://oem.bm
j.com/
Occup E
nviron Med: first published as 10.1136/oem
.57.12.793 on 1 Decem
ber 2000. Dow
nloaded from

polymorphisms cannot distinguish betweenthese two mechanisms. It was not possible tofind the origin of the non-disjunction in theremaining subject, because of failure of theDNA analysis of the necropsy material, despiteseveral attempts by us and the Forensic ScienceService in Birmingham. (The necropsy reportfor this infant gave mongolism as the underly-ing cause of death.) Cytogenetic analysis ofblood samples taken from the parents of thischild, undertaken to exclude the possibility offamilial translocation, showed a variant chro-mosome 4 in the father (table 2). The variantchromosome number 4, identified with QFQ-banding, is generally considered to be clinicallyunimportant.
ANALYSIS
The maternal age distribution of the 374 livebirths with the maternal age identified in thereturned questionnaires completed by pastpupils of St Louis’ School is given in table 3.Also given in table 3 are, for each maternal agegroup, the observed number of births withDown’s syndrome and the expected number ofsuch births obtained from maternal age specificreference rates.13 The six observed births withDown’s syndrome compare with a maternalage adjusted expected number of 0.69 (nomi-nal Poisson p(O>6)<10-4). The five aVectedbirths to mothers under 30 years of agecompare with 0.15 expected (nominal p<10-6).
Of the 671 questionnaires issued by Sheehanto women who had been pupils at the larger dayschool, St Vincent’s School, Dundalk, during1956–7, only 319 (48%) were completed andreturned. Among the 920 live births reportedin these completed questionnaires were fourchildren with Down’s syndrome, which is inexcess of the maternal age adjusted expectednumber of 1.8, but not significantly so. Onlyone of the aVected births was to a motherunder 30 years of age (she was 29 years of age)which compares with 0.4 expected. Again, thisdiVerence is not significant. The results ofthese comparisons must be viewed withcaution given the low response rate.
COUNTY LOUTH AND NEWRY AND MOURNE
DISTRICT
During 1961–70, in 17 012 live births tomothers normally resident in County Louththere were 48 babies with Down’s syndrome,and during 1971–80 there were 37 withDown’s syndrome among 19 489 live births.The numbers of these births by maternal agegroup are given in table 4, as are the maternalage specific incidences for Down’s syndrome inCounty Louth. Observed numbers did not dif-fer significantly from maternal age adjustedexpected numbers for all maternal ages ormaternal ages less than 30 years during 1961–70, 1971–80, or 1961–80.
During 1961–70, there were an estimated17 141 live births to mothers resident in Newryand Mourne District, Northern Ireland.Among these births were 37 babies withDown’s syndrome. During 1971–80, therewere 33 births with Down’s syndrome amongan estimated number of 16 382 live births. Noterminations of pregnancy after positive prena-tal testing occurred among women resident inNewry and Mourne District during these twoperiods. From hospital records, maternal agesfor live births during 1961, 1966, and 1970were available for, respectively, 54%, 63%, and86% of all live births in the District. Details bymaternal age group are presented in table 4,where estimated maternal age specific rates are
Table 2 Details of karyotypes and origin of non-disjunction in families of Down’s syndrome births to mothers who hadattended St Louis’ Secondary School, Dundalk, during 1956–7
Caseidentifier
FamilyMember Karyotype
Origin of non-disjunction
Chromosome polymorphisms DNA polymorphisms
1 Father 46, XYChild 47, XX, +21 Maternal second meiotic Mitotic after fertilisationMother 46, XX
2 Father 46, XYChild 47, XY, + 21 Maternal first meiotic Maternal first meioticMother 46, XX
3* Father 46, XY, var(4)(p11,QFQ35)Child — Not studied (child died) FailedMother 46, XX
4 Father 46, XYChild 47, XX, +21 Maternal first meiotic Not studied (child died)Mother 46, XX
5 Father 46, XYChild 47, XX, +21 Maternal first meiotic Maternal first meioticMother 46, XX
6 Father 46, XYChild 47, XY, +21 Maternal first meiotic Maternal first meioticMother 46, XX
*Necropsy carried out at Our Lady of Lourdes’ Hospital, Drogheda. Necropsy report gives the underlying cause of death as “mon-golism”. Necropsy material unsuitable for DNA analysis.
Table 3 Number of live births, and the number of cases of Down’s syndrome observed andexpected among these births, by maternal age group, for women who attended St Louis’Secondary School, Dundalk, during 1956–7, as determined by completed questionnaires(reference rates are those obtained by Cuckle et al13)
Maternal agegroup (y)
Live births(n)
Observed cases ofDown’s syndrome(n)
Reference incidence ofDown’s syndrome(per 104 live births)
Expected cases ofDown’s syndrome(n)
<20 0 0 6.2 020–24 23 1 6.7 0.01525–29 158 4 8.8 0.13930–34 127 1 13.8 0.17535–39 56 0 39.3 0.22340–44 10 0 138.2 0.138>45 0 0 404.2 0N/A* 13 0 — —
*Maternal age at the birth not available.
Cluster of Down’s syndrome 797
www.occenvmed.com
on July 28, 2021 by guest. Protected by copyright.
http://oem.bm
j.com/
Occup E
nviron Med: first published as 10.1136/oem
.57.12.793 on 1 Decem
ber 2000. Dow
nloaded from

also given. No significant diVerences betweenobserved and expected numbers occurred foreither all maternal ages or maternal ages under30 years during 1961–70, 1971–80, or 1961–80.
Inspection of maiden names and ages ofmothers of children with Down’s syndrome(details which were almost invariably availablefrom records), who could have attended schoolduring 1956–7, did not show any furtherformer pupils of St Louis’ School or StVincent’s School. Owing to the initial identifi-cation of an aVected child of a mother who hadattended the primary school in the vicinity of StLouis’ School during 1956–7, the mothers ofchildren with Down’s syndrome born inCounty Louth or Newry and Mourne Districtwere checked against the roll for this school.This showed a further two children withDown’s syndrome born to mothers who werepupils at this primary school in 1956–7,although one of these mothers left the school inJune 1956. Primary trisomy 21 was confirmedin all three children. Only one of the motherswas under 30 years of age at the birth of theaVected child, and she was 28 years old. Fromthe primary school roll, at least 250 girls wouldhave attended the school in 1956–7. Assumingthat the average number of live births per pupil,and the maternal age distribution of thesebirths, are the same for the primary school girlsas for girls attending the socioeconomicallysimilar St Vincent’s School in 1956–7, then theexpected number of live births to these 250former pupils is 720, among which would be,on average, 1.4 babies aVected with Down’ssyndrome. Among the estimated 370 live births
to mothers under 30 years of age, 0.3 cases ofDown’s syndrome would be expected. Neitherof these expected numbers diVers significantlyfrom the numbers observed.
TURNER’S SYNDROME
Further examination of the 159 questionnairesreturned by former pupils of St Louis’ Schoolshowed two live born oVspring aVected bychromosomal abnormalities other than Down’ssyndrome. In both, the anomaly was Turner’ssyndrome, characterised by monosomy X.Details are given in table 5. Turner’s syndromehas a birth prevalence in females of 1 in 2000 to1 in 5000,14 which shows no apparent variationwith parental age.15 Therefore, in the 203 liveborn girls of mothers who completed the ques-tionnaire, at most 0.1 cases of Turner’ssyndrome would be expected. The two ob-served are a significant excess (nominalp<0.005). Cytogenetic analysis of peripheralblood lymphocytes previously sampled fromone of the aVected children (case A), carriedout at the cytogenetics laboratory in Belfast,had shown a mosaic karyotype, 45,X/46,X,i(X)(q10). Samples of peripheral bloodwere obtained from both aVected people andtheir parents for DNA analysis. Karyotyping ofthe other girl (case B) was also carried out, andshowed non-mosaic 45,X. Analysis for sixDNA polymorphic loci on the X chromosomeindicated that the child with non-mosaicmonosomy X was the result of maternalmeiotic non-disjunction. The error resulting inthe mosaic arose after fertilisation and involvedthe paternally derived X chromosome.
Table 4 The numbers of live births, numbers of live births with Down’s syndrome and prevalences of Down’s syndrome per104 live births, during 1961–80 and 1971–80 by maternal age group for County Louth and Newry and Mourne District(reference incidences of Down’s syndrome from Cuckle et al13)
Maternal agegroup (y)
Referenceincidence oflive birthswith Down’ssyndrome(×10−4)
1961–70 1971–80
Live births(n)
Live birthswith Down’ssyndrome (n)
Prevalence oflive births withDown’ssyndrome(×10−4) (n)
Live births(n)
Live birthswith Down’ssyndrome (n)
Prevalence oflive births withDown’ssyndrome(×10−4) (n)
County Louth:<20 6.2 502 0 0 994 2 20.120–24 6.7 3567 2 5.6 5090 3 5.925–29 8.8 4792 5 10.4 6327 4 6.330–34 13.8 3935 6 15.2 4165 6 14.435–39 39.3 2861 15 52.4 2163 12 55.540–44 138.2 1229 13 105.8 667 9 134.9>45 404.2 102 7 686.3 53 1 188.7N/A* — 24 0 — 30 0 —
Newry and Mourne District:†<20 6.2 737 0 0 985 0 020–24 6.7 4052 0 0 4533 1 2.225–29 8.8 4926 4 8.1 5117 5 9.830–34 13.8 3905 6 15.4 3438 7 20.435–39 39.3 2454 11 44.8 1697 8 47.140–44 138.2 954 12 125.8 556 11 197.8>45 404.2 96 4 416.7 48 1 208.3
*Maternal age at the birth not available.† For 1961–73, the annual numbers of live births were estimated as described in the text.
Table 5 Details of live births with Turner’s syndrome to mothers who had attended St Louis’ Secondary School, Dundalk,during 1956–7, as obtained from completed questionnaires
Caseidentifier
Date of birth(month/y)
Place ofbirth Parity
Maternalage (y)
Paternalage (y)
Period at St Louis’Secondary School(month/y) Comment
A 5/68 Belfast 1 24 29 9/57–6/62 Day girlB 1/70 Liverpool 2 26 28 9/56–6/61 Boarder
798 Dean, Nevin, Mikkelsen, et al
www.occenvmed.com
on July 28, 2021 by guest. Protected by copyright.
http://oem.bm
j.com/
Occup E
nviron Med: first published as 10.1136/oem
.57.12.793 on 1 Decem
ber 2000. Dow
nloaded from

DiscussionTHE SCHOOLS
The high level of response (89%) to thequestionnaires issued to former pupils of StLouis’ School, the publicity given to the originalreport1 of this cluster, and the absence of anyfurther linkages of children with Down’ssyndrome to oVspring of former pupils of theschool, gives confidence in the completeness ofthe known number of births with Down’ssyndrome to women who had attended theschool during 1956–7. If it is assumed that theadditional 13 live births with an unknownmaternal age (table 3) have the same maternalage distribution as those 374 live births with aknown maternal age, and if it is further assumedthat the same average number of live births withthe same maternal age profile apply to thosewomen who did not respond to the question-naire as were found for those who did, then thematernal age adjusted expected number ofcases of Down’s syndrome among all live birthsto women who had attended St Louis’ Schoolduring 1956–7 would increase to 0.80. If noDown’s syndrome occurred among the liveborn children of the non-responders, then anobserved number of six compares with anexpected number of 0.80 (nominal p<5x10-4).If attention is concentrated on the 181 livebirths to mothers known to have been under 30years of age when they gave birth, then, on thesame assumptions about missing information,the expected number would be 0.18 (nominalp<5x10-6). Therefore, given the high responserate and the relatively few live births for whichinformation is lacking, the nominal significanceof the excess is robust. Evidently, the clusterconstitutes a highly unusual aggregation ofDown’s syndrome.
By contrast, the low response rate (48%)among past pupils of St Vincent’s School doesnot allow confidence in a comparison ofobserved and expected numbers. If it isassumed, however, that no further casesoccurred among live births to non-respondersand that these births have the same maternalage structure as those to responders, then thefour births with Down’s syndrome at all mater-nal ages, one of which was to a mother under30 years old, would be very similar to theexpected numbers for all past pupils of 3.7 and0.8, respectively. Given the absence of any fur-ther linkages between mothers of aVected chil-dren and pupils of St Vincent’s School during1956–7, it is reasonably clear that the markedexcess of Down’s syndrome among children ofyoung mothers who were former pupils of StLouis’ School does not extend to the oVspringof past pupils of the larger St Vincent’s School.
As well as the child with Down’s syndromeborn to a mother who had attended theprimary school near St Louis’ School in1956–7, and who was originally1 (and mistak-enly) thought to have attended St Louis’School, two aVected oVspring of past pupils ofthis primary school were identified. Question-naires had not been issued systematically topast pupils of the primary school and soapproximate expected numbers of cases ofDown’s syndrome in the oVspring had to be
derived. No significant diVerences betweenobserved and expected numbers were found,although the comparisons could only be crude.However, the single aVected birth to a motherunder 30 years of age suggests that a notableexcess of Down’s syndrome is not present inthe oVspring of young mothers who hadattended this primary school in 1956–7.
COUNTY LOUTH AND NEWRY AND MOURNE
DISTRICT
The maternal age specific incidences ofDown’s syndrome for County Louth during1961–70 and 1971–80 (shown in table 4),periods which include the dates of birth of thechildren with Down’s syndrome born to moth-ers who had attended St Louis’ School in1956–7, do not indicate that the underlyingrisk of Down’s syndrome, whether for allmothers or for young mothers specifically, israised in comparison with that expected fromreference rates. Our Lady of Lourdes’ Hospitalin Drogheda is the major maternity hospital inthe north east of the Republic of Ireland.Between 1962 and 1973, 78 babies withDown’s syndrome were born at this hospitalout of a total of 27 227 live births, giving acrude incidence of 28.6/104 live births. Thisrate is comparable with the crude rate of 28.2/104 live births found for County Louth duringthe similar period 1961–70. More than half ofthe mothers giving birth at Our Lady of Lour-des’ Hospital during this period were not resi-dent in County Louth, suggesting that the inci-dence of Down’s syndrome in County Louth istypical of the north east of the Republic of Ire-land as a whole.
Although routinely collated birth data do notexist for smaller geographical areas withinCounty Louth, so that it is not possible todetermine the prevalence of Down’s syndromeamong live births to mothers resident in Dun-dalk itself, a rough comparison of observedwith expected numbers can be carried out fromthe numbers of women living in Dundalk andthe rest of County Louth, which are availablefrom census data. During 1961–70 and 1971–80, just under one third of women of childbearing age resident in County Louth were liv-ing in the town of Dundalk. During these twoperiods, out of totals of 48 and 37 live birthswith Down’s syndrome in the whole of CountyLouth, 13 and 14 aVected births, respectively,were to mothers resident in Dundalk. Conse-quently, from this breakdown, there is noevidence of any unusual distribution of the riskof Down’s syndrome between the town ofDundalk and the remainder of County Louth.
The observed prevalences for Down’s syn-drome among live births in the Newry andMourne District of Northern Ireland during1961–70 and 1971–80 are comparable withreference rates (table 4), and do not suggest anunusual level of risk. Certain assumptions hadto be made to derive the maternal age distribu-tions of live births in Newry and MourneDistrict, but these are unlikely to seriouslyunderestimate the observed rates.
Cluster of Down’s syndrome 799
www.occenvmed.com
on July 28, 2021 by guest. Protected by copyright.
http://oem.bm
j.com/
Occup E
nviron Med: first published as 10.1136/oem
.57.12.793 on 1 Decem
ber 2000. Dow
nloaded from

COMPARISON WITH OTHER AREAS IN IRELAND
The live birth prevalences of Down’s syndromein County Louth and Newry and Mourne Dis-trict may be compared with those that havebeen published for other areas of Ireland.O’Brien and Crowley16 examined the incidenceof Down’s syndrome among 111 208 livebirths during 1966–81 at the NationalMaternity Hospital, Dublin. There were 225babies with Down’s syndrome live born in thishospital during this 16 year period. The mater-nal age specific incidences of Down’s syndromeobtained by O’Brien and Crowley are shown intable 6. Johnson et al17 studied the prevalence ofDown’s syndrome among live births in1981–90 in four Irish counties (Dublin,Kildare, Wicklow, and Galway) which werecovered by registries participating in the Euro-pean registration of congenital anomalies(EUROCAT) project.18 The maternal age spe-cific rates are given in table 6. The Lowry com-mittee (on which NN sat) investigated the inci-dence of Down’s syndrome in districts ofNorthern Ireland during 1974–84.11 The datapresented were for live births and did notinclude cases of positive prenatal testing andsubsequent induced abortion which is prac-tised in Northern Ireland, unlike the Republicof Ireland. As induced abortions will influencethe prevalence of Down’s syndrome among livebirths, it is important to include data oninduced abortions where these contribute aconsiderable fraction of the overall number ofcases of Down’s syndrome, to enable a propercomparison with areas where termination ofpregnancy is not performed. One of us (NN)has collated relevant terminations in NorthernIreland during 1974–84. Also available fromthe EUROCAT registry for Northern Ireland(maintained by NN) are the numbers of livebirths and induced abortions with Down’s syn-drome between 1985 and 1997. The numberof terminations was multiplied by 0.74 beforebeing added to the number of live births withDown’s syndrome to account for the likelihoodthat the pregnancy would have resulted in astillbirth.19 The resulting maternal age specificincidences for Northern Ireland for the period1974–97 are given in table 6.
The rapidly rising risk of Down’s syndromewith increasing maternal age is well estab-lished. Therefore, it is necessary to correct forthe maternal age distribution of births whencomparing areas where, or periods when, the
proportion of births to older mothers diVers, asis the case in Ireland. Under these circum-stances, the comparison of crude incidences islikely to be misleading. It is clear, however, thatwhen a comparison is made of maternal agespecific rates of Down’s syndrome for thoseareas of Ireland for which data are reasonablycomplete and reliable, then incidence ofDown’s syndrome does not show marked vari-ations. The maternal age specific incidences forCounty Louth and Newry and MourneDistrict are compatible with those obtainedfrom other areas of Ireland (table 6).
INTERPRETATION OF CLUSTERS
It seems clear that the excess occurrence ofDown’s syndrome among babies born to youngmothers who were pupils of St Louis’ School,Dundalk, in 1956–7 is highly unusual but thatit does not extend generally to Dundalk or tothe rest of County Louth, or to the adjacentNewry and Mourne District. Indeed, thematernal age specific incidences of Down’ssyndrome for County Louth and Newry andMourne District are at the levels expected fromreference rates and from other areas of Ireland.It must be considered, therefore, whether thislocalised cluster of cases associated withmaternal attendance at St Louis’ School during1956 and 1957 represents a genuinely raisedunderlying risk of Down’s syndrome, orwhether the cluster is a rare eVect of chancewhich does not reflect an increased risk.Although it would seem at face value that theplay of chance would have to be extreme toaccount for this cluster, it must be appreciatedthat striking clusters will occur naturally as sta-tistical fluctuations above a uniform underlyingrisk, and that the retrospective nature of mostcluster investigations tends to enhance thenominal significance of clusters which arereported by alert clinicians.
Given the diYculty of distinguishing a causalsignal from statistical noise, Rothman20 hasargued that:
“with very few exceptions, there is little scientific orpublic health purpose to investigate individualdisease clusters at all”
and this has been illustrated by Caldwell21 whonoted that of 108 cancer clusters investigatedby the United States Centers for Disease Con-trol from 1961, no clear cause was found forany cluster. Olsen et al22 have highlighted the
Table 6 Maternal age specific incidences of Down’s syndrome (per 104 live births) for various areas of Ireland (numbersof live births with Down’s syndrome are given in parentheses)
Maternalage group(y) Reference13
County Louth(1961–80)
Newry andMourneDistrict(1961–80)
National MaternityHospital, Dublin16
(1966–81)*
Counties Dublin,Kildare, Wicklow,and Galway17
(1981–90)Northern Ireland(1974–97)†
<20 6.2 13.4 (2) 0 (0) 4 5.4 (7) 4.7 (22)20–24 6.7 5.8 (5) 1.2 (1) 4 6.4 (32) 6.6 (108.7)25–29 8.8 8.1 (9) 9.0 (9) 9 9.7 (79) 9.3 (195.7)30–34 13.8 14.8 (12) 17.7 (13) 15 15.2 (101) 15.4 (217.4)35–39 39.3 53.7 (27) 45.8 (19) 56 43.2 (132) 43.9 (254.0)40–44 138.2 116.0 (22) 152.3 (23) H166
137.8 (93) 153.2 (191.6)>45 404.2 516.1 (8) 347.2 (5) 390.2 (16) 322.0 (21.2)
*The number of Down’s syndrome live births in each maternal age group is not given by O’Brien and Crowley,16 but overall therewere 225 Down’s syndrome babies among 111 208 live births.†Includes 956 live births and (with appropriate adjustment, see text) 74 cases of positive prenatal testing and subsequent inducedabortion.
800 Dean, Nevin, Mikkelsen, et al
www.occenvmed.com
on July 28, 2021 by guest. Protected by copyright.
http://oem.bm
j.com/
Occup E
nviron Med: first published as 10.1136/oem
.57.12.793 on 1 Decem
ber 2000. Dow
nloaded from

tendency in retrospective investigations of dis-ease clusters for “boundary tightening” aroundthe population in which the cluster is seen:
“the more narrowly the underlying population isdefined, the less will be the number of expectedcases, the greater will be the estimates of the excessrate, and often the more pronounced will be thestatistical significance”.
They have likened this process to the “Texassharpshooter” who first fires his gun and thendraws the target around the bullet hole, ananalogy first used by GruVerman and Delzell23
when discussing clusters of Hodgkin’slymphoma. Glass et al24 illustrated this pointwith childhood leukaemia data for Los AngelesCounty. They noted that by severely tighteningthe boundaries around a few cases, they wereable to create clusters comparable with thosepreviously described in the scientific literature.They warned:
“in the study of a relatively rare disease such as leu-kaemia, it is important to keep in mind thepossibility that seemingly high concentrations ofcases may be generated by over-zealous statisticalmanipulation”.
Boundary constriction is not just a problem ofgeographical area, but applies equally to thechoice of time interval, age group, disease type,etc selected retrospectively. Recently, the prob-lem of interpreting clusters has been empha-sised by Hook and Carothers25 who analysed areported excess of Down’s syndrome in birthsto young mothers in Norway during 1985–6,and concluded that it was likely to have arisenby chance.
There is no doubt that the cluster of cases ofDown’s syndrome associated with St Louis’School is a retrospective observation which hashad boundary tightening: the adverse healtheVect (Down’s syndrome) and the location(maternal attendance at St Louis’ School) weredictated by the initial report, and the clusterwas further defined in retrospect by period(1956–7) and age group (maternal age <30years). This makes the true significance of thiscluster diYcult, if not impossible, to properlyassess. Interpretation is further complicated bytwo of the five young mothers (cases 2 and 5)not attending the school at the same time, andby the error which led to Down’s syndrome inthe child of a further young mother (case 1)occurring after fertilisation. (That Down’s syn-drome in four of the six aVected children origi-nated at the first maternal meiotic division isnot surprising as, in general, 80%–90% of casesare maternally derived, and of these, about75% are due to first meiotic failure.26–27) ThisdiYculty of interpretation is enhanced by thenominally significant excess of another chro-mosomal anomaly, Turner’s syndrome, in thesame group of children: one of the two was amosaic, with the error after fertilisation involv-ing the paternally derived X chromosome, andcould not be due to any exposure of the motheras a child, but the second was the result ofmaternal meiotic non-disjunction and this isthought to occur in only 20%–30% of cases ofTurner’s syndrome.15
CAUSES OF DOWN’S SYNDROME
If the cluster of Down’s syndrome is not ahighly unusual chance fluctuation, but reflectsa genuinely increased underlying risk, thenwhat factor (or factors) might have caused thisraised risk? It is apparent that the two possiblecauses originally suggested by Sheehan andHillary,1 the influenza epidemic during theautumn of 1957 and radioactive contaminationfrom the Windscale fire of October 1957, areimplausible candidates. Of the five girls at StLouis’ School during the years 1956–7 wholater gave birth to a child with Down’ssyndrome while under 30 years of age, three(cases 2, 3, and 4) had left St Louis’ Schoolbefore the 1957 summer vacation, and thesethree in themselves constitute a significantexcess over expectation (nominal p<0.001), sothat events occurring at the school in theautumn of 1957 cannot account for the excess.These three girls were not in Dundalk in theautumn of 1957 but were by then resident ineither London or Dublin, so that factors localto Dundalk at this time could not have aVectedthem. Furthermore, the influenza epidemicinvolved the whole of Ireland and it would alsobe expected that any radioactive contaminationfrom the Windscale fire would influence awider area than just St Louis’ School, makingthese two occurrences improbable explana-tions for the highly localised nature of the clus-ter of Down’s syndrome. Moreover, the testingof serum samples from six mothers of aVectedchildren for antibodies to several strains ofinfluenza showed nothing unusual,1 and theradioactive plume from the Windscale firetravelled predominantly in a southeasterlydirection over England to the mainland ofEurope, rather than in a westerly direction overIreland.28 It must also be noted that Down’ssyndrome in one of the aVected children (case1) whose mother was at the school in October1957 has now been shown to be the result of anerror in mitosis after fertilisation and it is diY-cult to envisage how this could have beeninfluenced by childhood events.
The only well established risk factor forDown’s syndrome is increasing maternal age,and there is still very little knowledge of themechanisms that cause non-disjunction. Re-cently, it has been suggested that chromosomesegregation is influenced by the extent andnature of the genetic recombination whichoccurs during the first meiotic division and thatthis influence can extend to the second meioticdivision.29 However, the search for factors inthe environment, or related to the health of themother, which could aVect segregation andhence result in increased meiotic non-disjunction has so far failed to identify anythingconclusive.30 In the 1960s it was found thatthyroid disease was more common in womenwho had given birth to a child with Down’ssyndrome and this led to suggestions thatincreased concentrations of maternal thyroidantibodies could be associated with an in-creased risk.31 32 Although several subsequentstudies seemed to show increased concentra-tions of thyroid antibodies in mothers ofchildren with Down’s syndrome, these have
Cluster of Down’s syndrome 801
www.occenvmed.com
on July 28, 2021 by guest. Protected by copyright.
http://oem.bm
j.com/
Occup E
nviron Med: first published as 10.1136/oem
.57.12.793 on 1 Decem
ber 2000. Dow
nloaded from

been criticised for being conducted many yearsafter the birth of the child and for the quality ofthe control data, and two recent studies havefailed to confirm that the presence of thyroidantibodies in maternal serum samples is a sig-nificant risk factor.33 34
The finding that births of children withDown’s syndrome seem to be aggregated ledPleydell35 to suggest the involvement of aninfectious agent. Stoller and Collmann36 founda significant association between the occur-rence of infectious hepatitis and the birth ofchildren with Down’s syndrome 9 monthslater, but other studies have found no evidencefor such a correlation.37–39 A study39 of Down’ssyndrome in births in British Columbia, as wellas finding no correlation with infectious hepa-titis, found no variation in yearly or seasonalincidence nor any association with severalother notifiable diseases (streptococcal infec-tions, chicken pox, influenza, measles, mumps,poliomyelitis, and rubella). Nevertheless, sea-sonal variations have been reported (referencescited by Puri and Singh40) with most of thesestudies finding a lower frequency of aVectedbirths in the winter and a peak in the summer.However, a recent review by Stolwijk et al41
concluded that the prevalence of Down’ssyndrome is not aVected by seasonality and thishas been supported by analysis of data from theUnited Kingdom national Down’s syndromecytogenetic register.42 Kallen43 has reviewed theconflicting data on maternal smoking andDown’s syndrome, and after a study of Swedishhealth registries, has concluded that there is nodirect risk from smoking on Down’s syndrome.Suggestions that parity may influence the riskof Down’s syndrome have not been supportedby recent studies which have recognised thatthe confounding eVects of diVerent attitudes totermination of pregnancy may influence suchfindings.44 45 An increase in chromosomalanomalies has been found in children of moth-ers taking various drugs around the period offertilisation.46 In a recent comprehensive study,Stoll et al47 examined a range of maternallyrelated factors such as smoking, alcoholconsumption, medication, diabetes, parity, andcontraceptives, and also investigated paternalage, seasonality, and consanguinity. There wassome suggestion that consanguinity and mater-nal diabetes might be associated with Down’ssyndrome, but no other factors were identified.
Perhaps the most extensively studied envi-ronmental factor in relation to Down’s syn-drome is ionising radiation. After a review ofmaternal preconception irradiation the UnitedNations Scientific Committee on the EVects ofAtomic Radiation concluded that the data donot allow the dismissal of the possibility thatradiation can cause an increase in maternalnon-disjunction, but noted that this suggestionis not supported by data from the children ofthe Japanese atomic bomb survivors.48 TheUnited States Committee on the BiologicalEVects of Ionizing Radiations, while recognis-ing that non-disjunction is an importantcontributor to the spontaneous genetic burdenin humans, concluded that low level irradiationmay not be a serious concern.49 Data that sug-
gest a higher incidence of Down’s syndrome inareas of high background radiation have beenseverely criticised,48–50 and the earlier report ofan increased incidence in the high backgroundradiation area of Kerala51 has not beensupported by studies that used more reliabledatabases.52 Other studies have also failed toprovide convincing evidence for Down’s syn-drome being produced by exposure toradiation,53–59 the one puzzling result being anapparently significant eVect found for exposureto radiation in older fathers.60 Bound et al61
reported an association between the prevalenceof Down’s syndrome in births in northwestEngland during 1957–91 and the annual levelof fallout from atmospheric nuclear weaponstesting. However, in a preliminary study afterthe accident at Chernobyl in 1986, de Wals etal62 examined data submitted to EUROCATregistries and found no evidence for anincrease in Down’s syndrome associated withexposure around the time of conception, afinding recently confirmed by Dolk et al.63 In areview of national studies on the impact of theChernobyl accident, Little64 noted that theincrease in Down’s syndrome in West Berlin inJanuary 1987, first reported in English bySperling et al,65 is not confirmed in larger andmore representative European series. Burkartet al66 have noted that the cluster in West Berlinwas preceded by an equally significant clusterin northern Bavaria and a previously higherthan average rate in southern Bavaria, both ofwhich have their origins before the Chernobylaccident. An excess of cases in the LothianRegion of Scotland, reported as being associ-ated with Chernobyl fallout, has not been con-firmed in a recent more extensive analysis,68
and Stoll et al47 note that no space-time clusterswere found in their study of the Strasbourgarea, although the Chernobyl accident oc-curred during the course of the study. In arecent review, Verger69 concludes that thecurrent evidence from epidemiological studiesfor an association between Down’s syndromeand radiation is “contradictory and not con-vincing”.
Any exposure that was to be responsible forthe cluster of Down’s syndrome associatedwith maternal attendance at St Louis’ Schoolwould have to be highly localised in its eVect tohave such a pronounced influence solely uponthe girls of this particular school, and seem-ingly would have to have occurred sometimebetween September 1955 and June 1957 whenall of the women were pupils at the school for atleast 1 academic year. It is possible that pupilsexperienced a very localised viral infectionduring this period, but there is no evidence tosuggest this, and the presence of a considerableproportion of day girls makes this possibilityless likely than when the school was thought tobe a closed community.2 Discussions withteachers at St Louis’ School did not show evi-dence of any other unusual exposures experi-enced predominantly by the girls of St Louis’School rather than by all girls resident in thegeneral vicinity of Dundalk.
802 Dean, Nevin, Mikkelsen, et al
www.occenvmed.com
on July 28, 2021 by guest. Protected by copyright.
http://oem.bm
j.com/
Occup E
nviron Med: first published as 10.1136/oem
.57.12.793 on 1 Decem
ber 2000. Dow
nloaded from

ConclusionIn conclusion, we have been able to confirm astriking cluster of cases of Down’s syndromeamong births to young mothers who hadattended St Louis’ School in Dundalk at sometime during 1956 and 1957. No excess risk ofDown’s syndrome was found for children ofmothers who would have been resident else-where in Dundalk, or in the rest of CountyLouth, or in the adjacent area in the south ofNorthern Ireland, during this period. We havebeen unable to find a plausible common causeof the cases constituting this cluster, and detailsof the individual cases suggest that there maynot be one. Previously proposed possibleexplanations, an influenza epidemic or theWindscale fire, both of which occurred in theautumn of 1957, can be eVectively eliminatedbecause they cannot account for the cluster,and their action would not be so localised.Owing to the retrospective nature of this inves-tigation, and therefore, of the definition of thecluster by the cases observed, we are unable torule out chance as being wholly or principallyresponsible, and this may well be the most rea-sonable explanation.
We acknowledge the pioneering work on this cluster carried outby Dr Patricia Sheehan, without which this study would nothave been possible. We thank the many people who assisted uswith this study, especially Mrs Aine Buckley and the families ofchildren with Down’s syndrome. We thank Sr Colmcille and SrMaeve, St Louis’ School; Sr Joan, St Vincent’s School; MsAnaleen Quigley, Scoil Eoin Bàiske, Dundalk; Professor IreneHillary, Mrs Carmel Byrne, Dr Andrew McDonald, Mr DomMurtagh, Dr Rory O’Hanlon, Mr Kevin Marron, Ms JackieRooney, Ms Yvonne Gregory; Dr Zachary Johnson, EURO-CAT; Dr Victoria CoVey, Ms Bridie McCabe, the Foundationfor the Prevention of Childhood Handicap; the Down’sSyndrome Association of Ireland; Professor Nollaig Parfrey, DrTerry Brien, Cytogenetic Records, Dublin; Ms Audrey Arthur,St John of God’s, Drumcar; Ms Evelyn Higgins, Health Centre,Drogheda; Ms Rachel O’Donoghue, Births and DeathsRegister, Dublin; Mr Jerry Ruddy, Medically HandicappedRegister, Co Louth; Dr Carmel Mothersill, Dublin; DrRosaleen Corcoran, Director of Public Health, North-EasternHealth Board, and her staV. In Northern Ireland we thank DrNuala Keenan, Dr David Mayne, Mrs Dorothy Warnock, TowerHill, Armagh; Miss Elizabeth Anderson and Ms BronaghMcCartan, Daisy Hill Hospital, Newry; Mrs Anne Cooney, StJohn of God’s Hospital, Newry; Ms Christine Morgan, MourneHospital, Kilkeel; Ms Hilda McLaughlin for statistical analysis;Mr Stanley Campbell, the Registrar General’s OYce, Belfast;Dr Chris ConliVe, Institute for Counselling and PersonalDevelopment, Belfast; the Down’s Syndrome Association ofNorthern Ireland; Dr Mina Hollinger, community paediatri-cian, and Mr Tom Smith, principal social worker, Newry; thedoctors in medical practice in Newry and Mourne District; DrGilly Carson, Craigavon Hospital, Portadown. In Denmark wethank Mrs Hanne Poulsen and Mrs Hanne Sand for experttechnical assistance. We acknowledge the assistance of Dr PeterGill and his staV at the Forensic Science Service, Birmingham,in the laboratory analysis of necropsy material from one of thecases with Down’s syndrome. We are most grateful to ProfessorsSir Richard Doll, H John Evans, and Ernest B Hook forcommenting on an early draft of this paper. This study waspartly funded by the North-Eastern Health Board of theRepublic of Ireland.
1 Sheehan PME, Hillary IB. An unusual cluster of babies withDown’s syndrome born to former pupils of an Irish board-ing school. BMJ 1983;287:1428–9.
2 Sheehan PME, Hillary IB. An unusual cluster of babies withDown’s syndrome. BMJ 1984;288:147.
3 Sharp PM, McConnell DJ. An unusual cluster of babieswith Down’s syndrome: was it caused by the Windscalefire? BMJ 1984;289:378.
4 Brown A. Role of radiation in aetiology of Down’ssyndrome. BMJ 1984;288:147–8.
5 Mikkelsen M, Poulsen H, Grinsted J, et al. Non-disjunctionin trisomy 21: study of chromosomal heteromorphisms in110 families. Ann Hum Genet 1980;44:17–28.
6 Saiki RK, Gelfand DH, StoVel S, et al. Primer-directedenzymatic amplification of DNA with a thermostable DNApolymerase. Science 1988;239:487–91.
7 Petersen MB, Economou EP, Slaugenhaupt SA, et al. Link-age analysis of the human HMG14 gene on chromosome21 using a GT dinucleotide repeat as polymorphic marker.Genomics 1990;7:136–8.
8 Anon. Report and abstracts of the 5th InternationalWorkshop on Human Chromosome 21 Mapping 1994.Tsukuba, Japan, November 9–11, 1994. Cytogenet CellGenet 1995;70:147–82.
9 Petersen MB, Schinzel AA, Binkert F, et al. Use of shortsequence repeat DNA polymorphisms after PCR amplifi-cation to detect the parental origin of the additional chro-mosome 21 in Down syndrome. Am J Hum Genet 1991;48:65–71.
10 Chakravarti A, Slaugenhaupt SA. Methods for studyingrecombination on chromosomes that undergo non-disjunction. Genomics 1987;1:35–42.
11 Antonarakis SE, Avramopoulos D, Blouin JL, et al. Mitoticerrors in somatic cells cause trisomy 21 in about 4.5% ofcases and are not associated with advanced maternal age.Nat Genet 1993;3:146–50.
12 Independent Committee (Chairman, Lowry S). Investigationinto patterns of disease with possible association with radiationin Northern Ireland. Final report. Belfast: The StationeryOYce, 1989.
13 Cuckle HS, Wald NJ, Thompson SG. Estimating a woman’srisk of having a pregnancy associated with Down’ssyndrome using her age and serum á-fetoprotein level. Br JObstet Gynaecol 1987;94:387–402.
14 Zinn AR. Growing interest in Turner syndrome. Nat Genet1997;16:3–4.
15 Jacobs P, Dalton P, James R, et al. Turner syndrome: a cyto-genetic and molecular study. Ann Hum Genet 1997;61:471–83.
16 O’Brien N, Crowley P. Down’s syndrome and maternal age.Ir Med J 1984;77:10–11.
17 Johnson Z, Lillis D, Delany V, et al. The epidemiology ofDown syndrome in four counties in Ireland 1981–90. JPublic Health Med 1996;18:78–86.
18 Lechat MF, Dolk H. Registries of congenital anomalies:EUROCAT. Environ Health Perspect 1993;101(suppl 2):153–7.
19 Hook EB, Topol BB, Cross PK. The natural history ofcytogenetically abnormal fetuses detected at midtrimesteramneosentesis which are not terminated electively: newdata and estimates of the excess and relative risk of late fetaldeath associated with 47, +21 and some other abnormalkaryotypes. Am J Hum Genet 1989;45:855–61.
20 Rothman KJ. A sobering start for the cluster busters’conference. Am J Epidemiol 1990;132:S6–13.
21 Caldwell, GG. Twenty two years of cancer cluster investiga-tions at the Centers for Disease Control. Am J Epidemiol1990;132:S43–7.
22 Olsen SF, Martuzzi M, Eliott P. Cluster analysis and diseasemapping: why, when, and how? A step-by-step guide. BMJ1996;313:863–6.
23 GruVerman S, Delzell E. Epidemiology of Hodkgin’sdisease. Epidemiol Rev 1984;6:76–106.
24 Glass AG, Hill JA, Miller RW. Significance of leukemia clus-ters. J Pediatr 1968;73:101–7.
25 Hook EB, Carothers AD. Use of computer simulation toevaluate a putative cluster of genetic or teratologicoutcomes: adjustment for “multiple hypotheses” and appli-cation to a reported excess of Down’s syndrome. Genet Epi-demiol 1997;14:133–45.
26 Yoon PW, Freeman SB, Sherman SL, et al. Advancedmaternal age and the risk of Down syndrome characterizedby the meiotic stage of the chromosomal error: apopulation-based study. Am J Hum Genet 1996;58:628–33.
27 Ballesta F, Queralt R, Gomez D, et al. Parental origin andmeiotic stage of non-disjunction in 139 cases of trisomy 21.Ann Genet 1999;42:11–15.
28 Crick MJ, Linsley GS. An assessment of the radiologicalimpact of the Windscale reactor fire, October 1957. Int JRadiat Biol 1984;46:479–506.
29 Lamb NE, Freeman SB, Savage-Austin A, et al. Susceptiblechiasmate configurations of chromosome 21 predispose tonon-disjunction in both maternal meiosis I and meiosis II.Nat Genet 1996;14:400–5.
30 International Commission for Protection against Environ-mental Mutagens and Carcinogens. ICPEMC MeetingReport No 3. Is the incidence of Down syndrome increas-ing? Mutat Res 1986;175:263–66.
31 Fialkow PJ, Hecht F, Uchida IA, et al. Increased frequencyof thyroid autoantibodies in mothers of patients withDown’s syndrome. Lancet 1965;ii:868–70.
32 Engel E. Autoantibodies and chromosomal aberrations.Lancet 1967;i:1271–2.
33 Torfs CP, van den Berg BJ, Oechsli FW, et al. Thyroid anti-bodies as a risk factor for Down syndrome and other triso-mies. Am J Hum Genet 1990;47:727–34.
34 Gustafsson J, Anneren G, Ericsson UB, et al. Thyroid anti-bodies are not a risk factor for pregnancies with Down syn-drome. Prenat Diagn 1995;15:451–4.
35 Pleydell MJ. Mongolism and other congenital abnormali-ties. An epidemiological study in Northamptonshire.Lancet 1957;i:1314–19.
36 Stoller A, Collmann RD. Area relationship betweenincidences of infectious hepatitis and of the births ofchildren with Down’s syndrome nine months later. J MentDefic Res 1966;10:84–8.
37 Stark CR, Fraumeni JF. Viral hepatitis and Down’ssyndrome. Lancet 1966;i:1036–7.
38 Ceccarelli G, Torbidoni L. Viral hepatitis and Down’ssyndrome. Lancet 1967;i:438.
39 Miller JR, Baird PA. Some epidemiological aspects ofDown’s syndrome in British Columbia. Br J Prev Soc Med1968;22:81–5.
Cluster of Down’s syndrome 803
www.occenvmed.com
on July 28, 2021 by guest. Protected by copyright.
http://oem.bm
j.com/
Occup E
nviron Med: first published as 10.1136/oem
.57.12.793 on 1 Decem
ber 2000. Dow
nloaded from

40 Puri BK, Singh I. Season of birth in Down’s syndrome. Br JClin Pract 1995;49:129–30.
41 Stolwijk AM, Jongbloet PH, Zielhuis GA, et al. Seasonalvariation in the prevalence of Down syndrome at birth: areview. J Epidemiol Community Health 1997;51:350–3.
42 Morris JK, Alberman E, Mutton D. Is there evidence ofclustering in Down syndrome? Int J Epidemiol 1998;27:495–8.
43 Kallen K. Down’s syndrome and maternal smoking in earlypregnancy. Genet Epidemiol 1997;14:77–84.
44 Kallen K. Parity and Down syndrome. Am J Med Genet1997;70:196–201.
45 Chan A, McCaul KA, Keane RJ, et al. EVect of parity, gra-vidity, previous miscarriage, and age on risk of Down’ssyndrome: population based study. BMJ 1998;317:923–4.
46 Watanabe G. Environmental determinants of birth defectsprevalence. Contr Epidem Biostatist 1979;1:91–100.
47 Stoll C, Alembik Y, Dott B, et al. Study of Down syndromein 238 942 consecutive births. Ann Genet 1998;41:44–51.
48 United Nations Scientific Committee on the EVects ofAtomic Radiation. Sources and eVects of ionizing radiation.UNSCEAR 1993 report to the General Assembly,with scientificannexes. New York: United Nations, 1993.
49 National Research Council. Health eVects of exposure to lowlevels of ionizing radiation. BEIR V. Washington DC:National Academy Press, 1990.
50 United Nations Scientific Committee on the EVects ofAtomic Radiation. Sources and eVects of ionizing radiation.1977 report to the General Assembly, with annexes. New York:United Nations, 1977.
51 Kochupillai N, Veruma IC, Gerval MS, et al. Down’ssyndrome and related abnormalities in an area of highbackground radiation in coastal Kerala. Nature 1976;262:60–1.
52 Jaikrishan G, Andrews VJ, Thampi MV, et al. Genetic moni-toring of the human population from high-level naturalradiation areas of Kerala on the southwest coast of India. I.Prevalence of congenital malformations in newborns.Radiat Res 1999;152:S149–53.
53 Sever LE, Gilbert ES, Hessol NA, et al. A case-control studyof congenital malformations and occupational exposure tolow-level ionizing radiation. Am J Epidemiol 1988;127:226–42.
54 Sever LE, Hessol NA, Gilbert ES, et al. The prevalence atbirth of congenital malformations in communities near theHanford site. Am J Epidemol 1988;127:243–54.
55 Knox EG, Lancashire RJ. Epidemiology of congenital malfor-mations. London: The Stationery OYce, 1991.
56 Francis, J, Snee, M. A case control study of trisomy 21 andmaternal pre-conceptual radiography. Clin Radiol 1991;43:343–6.
57 Shields LM, Weise WH, Skipper BJ, et al. Navajo birth out-comes in the Shiprock uranium mining area. Health Phys1992;63:542–51.
58 Roman E, Doyle P, Ansell P, et al. Health of children born tomedical radiographers. Occup Environ Med 1996;53:73–9.
59 Kallen B, Karlsson P, Lundell M, et al. Outcome ofreproduction in women irradiated for skin hemangioma ininfancy. Radiat Res 1998;149:202–8.
60 Strigini P, Pierluigi M, Forni GL, et al. EVect of X-rays onchromosome 21 nondisjunction. Am J Med Genet Suppl1990;7:155–9.
61 Bound JP, Francis BJ, Harvey PW. Down’s syndrome:prevalence and ionising radiation in an area of north westEngland 1957–91. J Epidemiol Community Health 1995;49:164–70.
62 de Wals P, Bertrand F, de la Mata I, et al. Chromosomeanomalies and Chernobyl. Int J Epidemiol 1988;17:230–1.
63 Dolk H, Nichols R, et al. Evaluation of the impact of Cher-nobyl on the prevalence of congenital anomalies in 16regions of Europe. Int J Epidemiol 1999;28:941–8.
64 Little J. The Chernobyl accident, congenital anomalies andother reproductive outcomes. Paediatr Perinat Epidemiol1993;7:121–51.
65 Sperling K, Plez J, Wegner RD, et al. Frequency of trisomy21 in Germany before and after the Chernobyl accident.Biomed Pharmacother 1991;45:255–62.
66 Burkart W, Grosche B, Schoetzau A. Down syndrome clus-ters in Germany after the Chernobyl accident. Radiat Res1997;147:321–8.
67 Ramsay CN. Ellis PM, Zealley H. Down’s syndrome in theLothian region of Scotland: 1978–89. Biomed Pharmacother1991;45:267–72.
68 Huether CA, Haroldson K, Ellis PM, et al. Impact of prena-tal diagnosis on revised live birth prevalence estimates ofDown syndrome in the Lothian region of Scotland, 1978–92. Genet Epidemiol 1996;13:367–75.
69 Verger P. Down syndrome and ionizing radiation. HealthPhys 1997;73:882–93.
Correspondence and editorialsOccupational and Environmental Medicinewelcomes correspondence relating to any ofthe material appearing in the journal. Resultsfrom preliminary or small scale studies mayalso be published in the correspondencecolumn if this seems appropriate. Lettersshould be not more than 500 words in lengthand contain a minimum of references. Tablesand figures should be kept to an absolute
minimum. Letters are accepted on the under-standing that they be subject to editorial revi-sion and shortening.
The journal also publishes editorials whichare normally specially commissioned. TheEditor welcomes suggestions regarding suit-able topics; those wishing to submit aneditorial, however, should do so only after dis-cussion with the Editor.
804 Dean, Nevin, Mikkelsen, et al
www.occenvmed.com
on July 28, 2021 by guest. Protected by copyright.
http://oem.bm
j.com/
Occup E
nviron Med: first published as 10.1136/oem
.57.12.793 on 1 Decem
ber 2000. Dow
nloaded from

CORRECTION
Investigation of a cluster of children withDown Syndrome born to mothers whohad attended a school in Dundalk,Ireland. G DEAN, N C NEVIN, M MIKKELSEN,G KARADIMA, M B PETERSEN, M KELLY,J O’SULLIVAN. 2000;57:793-804.
Three small typographical errors occurred intable 1 of this paper which gave details of thecases constituting the cluster.
For case number 3 the parity should be 2and not 1, and the maternal age should be 25years and not 26 years.
For case number 5 the sex should befemale (F), not male (M). These changes donot aVect the remainder of the paper in any-way or the conclusions of the study.
NOTICES
International Short Course: VentilationDesign. 3–7 September 2001. Utrecht,The Netherlands
The course is organised by the Environmen-tal and Occupational Health Group. SinceMay 2000 this group together with theResearch Institute for Toxicology (RITOX)constitutes the Institute for Risk AssessmentSciences (IRAS). The actual move of theEOH group from Wageningen to Utrecht willtake place during the summer of 2001.
The course focuses on occupational hygi-enists, safety engineers, and all others whorequire more knowledge on the measuresavailable for reducing worker exposure to airpollutants.
Course contents:x General principles of airflowx General ventilationx Extraction ventilationx Ductings and fittingsx Fansx Ventilation measurement
x Practical ventilation measurementx Air filtration and discharges to atmos-
pherex Costs of ventilation.For further information contact: Dr Mieke
Lumens, Environmental and OccupationalHealth Group, Institute for Risk AssessmentSciences, Utrecht University, PO Box 80176,3508 TD Utrecht, The Netherlands. Tel +31317482080; fax +31 317485278; [email protected] or visit our websitehttp://www.slm.wau.nl/eoh/
International Short Course: Biologicalagents in the work and homeenvironment: exposure assessment andhealth risk evaluation. 10 –12 September2001. Utrecht, The Netherlands.
The course is organised by the Division ofEnvironmental and Occupational Health ofthe Institute for Risk Assessment Sciences,University of Utrecht (formerly the EOHgroup from Wageningen University).
The course focuses on occupational andenvironmental hygienists, physicians, andepidemiologists, and other researchers orpractitioners in the field of exposure andhealth risk assessment.
Contents:x Overview of most important biological
agents: exposure to micro-organisms,their endotoxins and secreted toxins,specific bioallergens in various occupa-tional environments and the home envi-ronment
x Sources and determinants of exposure tobiological agents
x Recognition of exposure to biologicalagents
x Bioaerosol related health eVects: infec-tious diseases, airway inflammatory dis-eases, organic dust toxic syndrome,allergy, cancer
x Epidemiology of health eVects related tobioaerosols
x Microbiological and microscopic meth-ods to evaluate exposure to microorgan-isms
x Immunoassays and biochemical assaysto evaluate exposure to microorganisms(markers of exposure), and allergens
x Risk assessment and evaluation forbiological agents
x Options to control exposure to micro-organisms.
For further information contact: Dr MiekeLumens, Environmental and OccupationalHealth Group, Institute for Risk AssessmentSciences, Utrecht University, PO Box 80176,3508 TD Utrecht, The Netherlands. Tel +31317482080; fax +31 317485278; [email protected] or visit our websitehttp://www.slm.wau.nl/eoh/
Work in the global village: aninternational high level conference onwork life in the 21st century. 15–17October 2001. Helsinki, Finland
The Conference is planned to be the firststage of a longer process, which will encour-age discussion on work and globalisation at aworldwide level, and which will eventuallylead to a high level follow up meeting. Theobjectives of the Conference are:
+ To discuss the global values and ethics inoccupational safety and health as adimension of decent work
+ To analyse the present status andperspectives of work life, and occupa-tional safety and health in the process ofglobalisation
+ To discuss the prerequisites for achiev-ing occupational health and safety di-mensions ensuring decent work for allworking people
+ To support the dissemination and im-plementation of the ILO safework pro-gramme and WHO global strategy onoccupational health for all by preparing adraft declaration on occupational safetyand health, and by producing a draft fora global strategy on the minimum levelof occupational safety and health for all,and by drafting a strategy to improveintersectoral collaboration and crosscultural understanding
+ To establish ad hoc workgroups toprepare discussion topics according tothe themes of the safework programme fora follow up meeting.
Deadline for abstracts 15 April 2001;letters of approval 15 June 2001; deadline forearly registration 15 August 2001.
Further information from: Work in theGlobal Village, Finnish Institute of Occupa-tional Health, Taina Pääkkönen, Topeliuk-senkatu 41 a A, FIN–00250 Helsinki,Finland. Tel 00358 9 4747 2910; Fax 003589 2413 804; email [email protected] www.occuphealth.fi/e/project/globalwork/
Occup Environ Med 2001;58:353 353
www.occenvmed.com