Embed Size (px)
Citation preview

REVIEW ARTICLE
Investigating the association between health literacy and non-adherence
Remo Ostini • Therese Kairuz
Received: 5 June 2013 / Accepted: 22 November 2013 / Published online: 1 December 2013
� Koninklijke Nederlandse Maatschappij ter bevordering der Pharmacie 2013
Abstract Background Low health literacy is expected to
be associated with medication non-adherence and early
research indicated that this might be the case. Further
research suggested that the relationship may be more
equivocal. Aim of the review The goal of this paper is
initially to clarify whether there is a clear relationship
between health literacy and non-adherence. Additionally,
this review aims to identify factors that may influence that
relationship and ultimately to better understand the mech-
anisms that may be at work in the relationship. Method
English language original research or published reviews of
health literacy and non-adherence to orally administered
medications in adults were identified through a search of
four bibliographic databases (PubMed, EMBASE, CI-
NAHL, and EBSCO Health). Results The search protocol
produced 78 potentially relevant articles, of which 16
articles addressed factors that contribute to non-adherence
and 24 articles reported on the results of research into the
relationship between non-adherence and health literacy.
Factors that contribute to non-adherence can be categorised
into patient related factors, including patient beliefs;
medication related factors; logistical factors; and factors
around the patient-provider relationship. Of the 23 original
research articles that investigated the relationship between
non-adherence and health literacy, only five reported
finding clear evidence of a relationship, four reported
mixed results and 15 articles reported not finding the
expected relationship. Research on possible mechanisms
relating health literacy to non-adherence suggest that dis-
ease and medication knowledge are not sufficient for
addressing non-adherence while self-efficacy is an impor-
tant factor. Other findings suggest a possible U-shaped
relationship between non-adherence and health literacy
where people with low health literacy are more often non-
adherent, largely unintentionally; people with moderate
health literacy are most adherent; and people with high
health literacy are somewhat non-adherent, sometimes due
to intentional non-adherence. Conclusion It is clear that
relevant research generally fails to find a significant rela-
tionship between non-adherence and health literacy. A U-
shaped relationship between these two conditions would
explain why linear statistical tests fail to identify a rela-
tionship across all three levels of health literacy. It can also
account for the conditions under which both positive and
negative relationships may be found.
Keywords Health literacy � Knowledge � Non-
adherence � Non-linear relationship � Patient
adherence � Self-efficacy
Impact on practice
• Improving patient’s health literacy is unlikely to
improve adherence if the focus is purely on improving
knowledge.
• Improving patient’s health literacy is likely to improve
adherence if it enhances patient self-efficacy. Improved
knowledge may have a role in this.
• People with low health literacy will require different
approaches to improving adherence than people with
high health literacy because their non-adherence is
R. Ostini (&)
School of Population Health, The University of Queensland,
Ipswich, QLD 4305, Australia
e-mail: [email protected]
T. Kairuz
School of Pharmacy, St Lucia, QLD 4072, Australia
123
Int J Clin Pharm (2014) 36:36–44
DOI 10.1007/s11096-013-9895-4

likely to be unintentional while high health literacy
patients have a greater likelihood of intentional non-
adherence.
Introduction
The simple premise underlying research into the rela-
tionship between health literacy and medicine-taking, is
that people who understand how to manage their health
will be adherent, taking medication as prescribed. Initial
findings from early research appeared to support the
basic proposition that health literacy interventions could
improve adherence [1, 2] but further research appeared
to indicate that the relationship between non-adherence
and health literacy was more ambiguous [3]. Results
began to show that for self-reported medication non-
adherence, the relationship with health literacy was not
predictable [4].
Health literacy
Health literacy typically refers to the ability of people to
obtain, process and understand health information and
services in order to make appropriate health decisions
[5]. In practice, much of the focus has been on under-
standing information with far less emphasis on the
components related to obtaining information and deci-
sion-making. The most frequently used current measures
of health literacy, such as the Test of Functional Health
Literacy in Adults: TOFHLA [6] and the Rapid Estimate
of Adult Literacy in Medicine: REALM [7, 8], focus on
literacy tasks such as reading and comprehension,
reducing the decision-making component even further.
The link between understanding and using information is
largely taken for granted.
Health literacy goes well beyond the narrow idea of
reading health-related material [9]. We take health liter-
acy to mean people’s capacity to manage their health,
similar to the way financial literacy is taken to mean
people’s capacity to manage their finances. In this sense,
health literacy incorporates the four factors that the
World Health Organisation (WHO) associates with non-
adherence—that is, the health care team and system, the
condition or illness, therapy (i.e., medication), and
patient-related factors [10]. This also corresponds with
the WHO definition of health literacy, which involves
cognitive and social skills together determining the ability
and motivation of individuals to promote and maintain
good health [11]. According to WHO, this process
requires knowledge, personal skills and confidence to
take action.
Non-adherence
Adherence to medication has been associated with
improved patient health outcomes and reduced unnecessary
costs [12]. However, non-adherence to medicines is not
necessarily the converse of adherence; the latter is defined
as the extent to which patients take medications as pre-
scribed by their health care provider [10], while non-
adherence indicates non-initiation, suboptimal dosing reg-
imens, or discontinuation of treatment [13]. The World
Health Organisation (WHO) describes non-adherence as a
‘‘multi-determined problem caused by the interplay of [the]
four factors’’ indicated above [10].
In contrast, adherence refers to the process by which
patients take their medication as prescribed [13] and is
associated with a degree of patient autonomy. The term is
more patient-centred than ‘compliance’ which reflects a
subservient patient role, [14] and ignores much of the pre-
scriber-patient dynamic. ‘Persistence’ generally refers to
patients who use continuous pharmacotherapy [15], from
initiation to the last dose prior to discontinuation, [13] and is
determined by using medication refills as a measure [15].
The terms are often used interchangeably and inconsistently.
Interventions that improve and maintain adherence at
optimal levels remain elusive, and studies have yet to
define a non-adherent patient [16]. In this review, we focus
on non-adherence while accepting that it is often treated as
a lack of adherence rather than the distinct concept that it
may be.
Aim of the review
The goal of this paper is to clarify whether or not there is a
clear, demonstrable, and meaningful relationship between
health literacy and medication non-adherence. Beyond this,
we will endeavour to identify and evaluate factors that may
influence or affect the relationship between health literacy
and medication non-adherence. In this way, we hope to
explain the ambiguous results that have been reported for
this relationship, identifying the conditions that promote or
impede it, and consider possible mechanisms underpinning
these effects.
Method
Search strategy
English language published reviews or original research on
health literacy and non-adherence to orally administered
medications were the focus of the search. Exclusion criteria
included research with children; opinion, editorial or
Int J Clin Pharm (2014) 36:36–44 37
123
commentary articles; and conference abstracts. Both qual-
itative and quantitative research was included.
Four bibliographic databases were searched. PubMed
(1951-April 19, 2013) was searched using a comprehensive
health literacy search based on a protocol developed by the
National Library of Medicine [17], combined with a search
using Adherence (text word) OR Persistence (text word)
OR Concordance (text word) OR Compliance (mesh major
topic) and a search using Non adherence (text word) OR
Non compliance (text word) as search terms. The same
specific terms were used in searches of the EMBASE
(1974–April 2013), CINAHL (1981-April 2013) and EB-
SCO Health (1969-April 2013) databases, using database
specific term mapping where available, or keyword sear-
ches where this was not available.
Article evaluation and data extraction
One author (RO) reviewed the titles of all articles identified
to assess potential relevance, and then reviewed the
abstracts of remaining articles to identify studies that met
inclusion and exclusion criteria.
Both authors extracted data from the remaining articles.
The primary goal of data extraction was to identify the
results of investigations into the relationship between
health literacy and non-adherence and the possible causes
of any relationship. In addition, descriptive features of
study samples and analysis methods that could assist in
evaluating strength of evidence were identified. Search
results were also used to extract information on factors
other than health literacy that had been investigated for
their association with non-adherence.
A narrative synthesis process incorporated the extracted
information into three main areas: examples of factors
associated with medication adherence, which may be rel-
evant to any health literacy–non-adherence relationship;
research investigating the relationship between non-
adherence and health literacy itself; and research reporting
potential mechanisms by which non-adherence and health
literacy might be associated.
Results
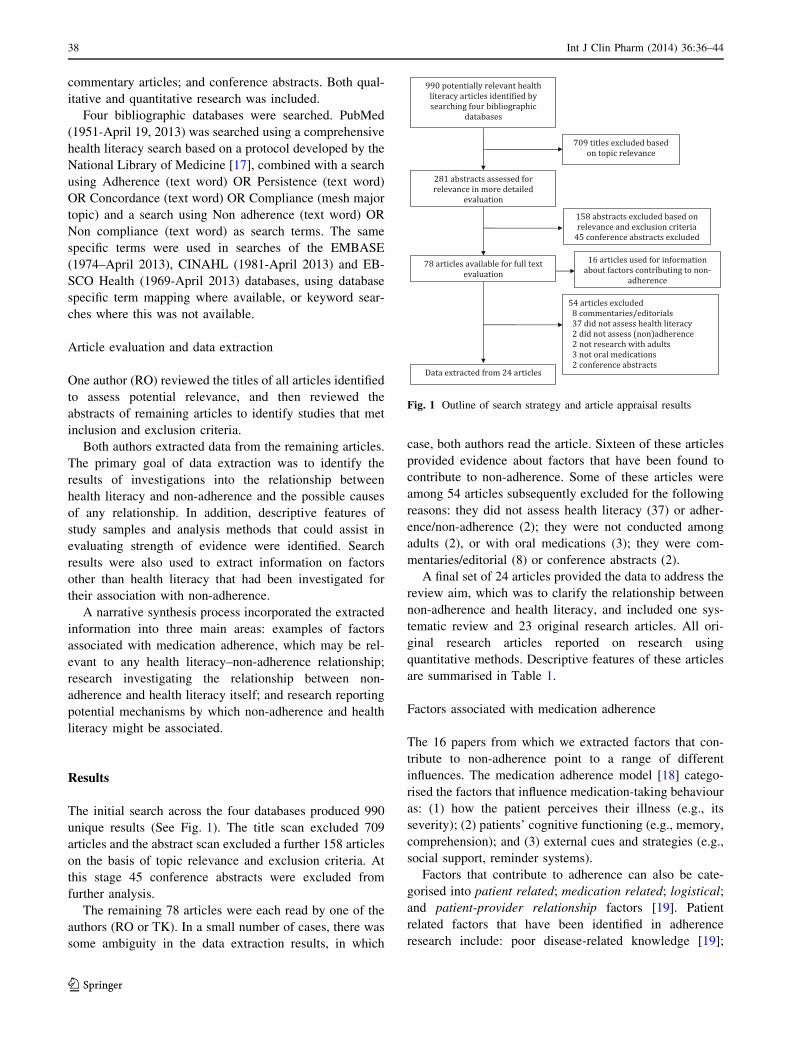
The initial search across the four databases produced 990
unique results (See Fig. 1). The title scan excluded 709
articles and the abstract scan excluded a further 158 articles
on the basis of topic relevance and exclusion criteria. At
this stage 45 conference abstracts were excluded from
further analysis.
The remaining 78 articles were each read by one of the
authors (RO or TK). In a small number of cases, there was
some ambiguity in the data extraction results, in which
case, both authors read the article. Sixteen of these articles
provided evidence about factors that have been found to
contribute to non-adherence. Some of these articles were
among 54 articles subsequently excluded for the following
reasons: they did not assess health literacy (37) or adher-
ence/non-adherence (2); they were not conducted among
adults (2), or with oral medications (3); they were com-
mentaries/editorial (8) or conference abstracts (2).
A final set of 24 articles provided the data to address the
review aim, which was to clarify the relationship between
non-adherence and health literacy, and included one sys-
tematic review and 23 original research articles. All ori-
ginal research articles reported on research using
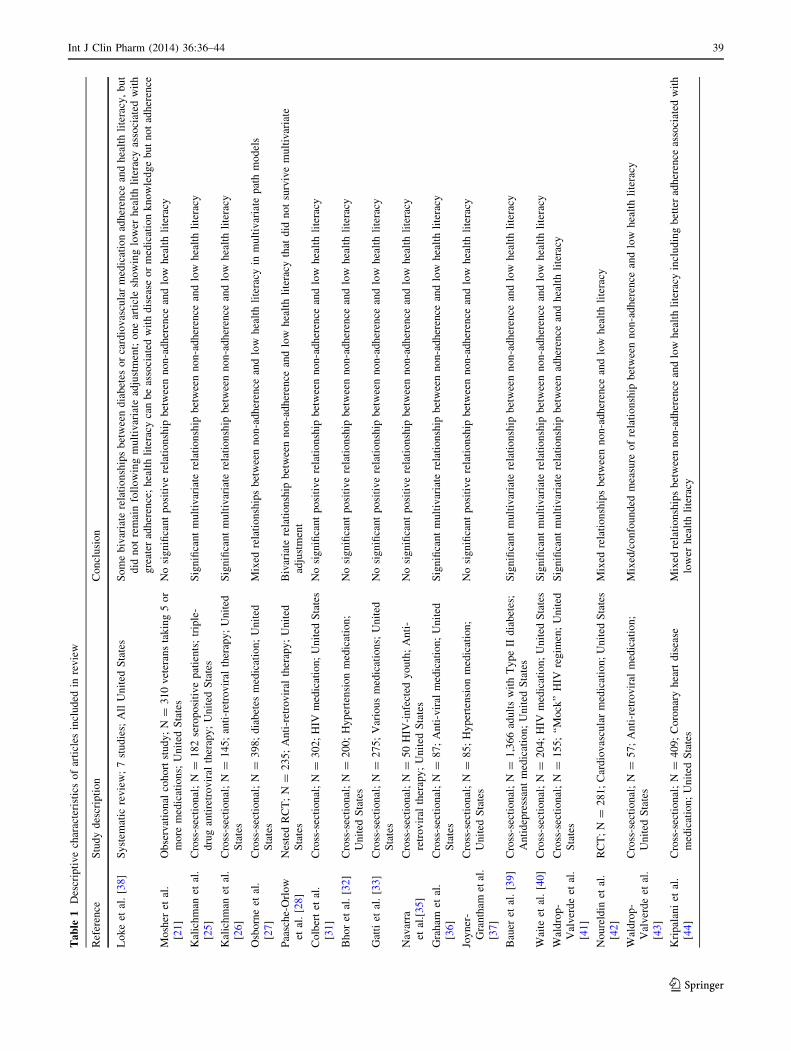
quantitative methods. Descriptive features of these articles
are summarised in Table 1.
Factors associated with medication adherence
The 16 papers from which we extracted factors that con-
tribute to non-adherence point to a range of different
influences. The medication adherence model [18] catego-
rised the factors that influence medication-taking behaviour
as: (1) how the patient perceives their illness (e.g., its
severity); (2) patients’ cognitive functioning (e.g., memory,
comprehension); and (3) external cues and strategies (e.g.,
social support, reminder systems).
Factors that contribute to adherence can also be cate-
gorised into patient related; medication related; logistical;
and patient-provider relationship factors [19]. Patient
related factors that have been identified in adherence
research include: poor disease-related knowledge [19];
Fig. 1 Outline of search strategy and article appraisal results
38 Int J Clin Pharm (2014) 36:36–44
123
Ta
ble
1D
escr
ipti
ve
char
acte
rist
ics
of
arti
cles
incl
ud
edin
rev
iew
Ref
eren
ceS
tud
yd
escr
ipti
on
Co
ncl
usi
on
Lo
ke
etal
.[3
8]
Sy
stem
atic
rev
iew
;7
stu
die
s;A
llU
nit
edS
tate
sS
om
eb
ivar
iate
rela
tio
nsh
ips
bet
wee
nd
iab
etes
or
card
iov
ascu
lar
med
icat
ion
adh
eren
cean
dh
ealt
hli
tera
cy,
bu
t
did
no
tre
mai
nfo
llo
win
gm
ult
ivar
iate
adju
stm
ent;
on
ear
ticl
esh
ow
ing
low
erh
ealt
hli
tera
cyas
soci
ated
wit
h
gre
ater
adh
eren
ce;
hea
lth
lite
racy
can
be
asso
ciat
edw
ith
dis
ease
or
med
icat
ion
kn
ow
led
ge
bu
tn
ot
adh
eren
ce
Mo
sher
etal
.
[21
]
Ob
serv
atio
nal
coh
ort
stu
dy
;N
=3
10
vet
eran
sta
kin
g5
or
mo
rem
edic
atio
ns;
Un
ited
Sta
tes
No
sig
nifi
can
tp
osi
tiv
ere
lati
on
ship
bet
wee
nn
on
-ad
her
ence
and
low
hea
lth
lite
racy
Kal
ich
man
etal
.
[25
]
Cro
ss-s
ecti
on
al;
N=
18
2se
rop
osi
tiv
ep
atie
nts
;tr
iple
-
dru
gan
tire
tro
vir
alth
erap
y;
Un
ited
Sta
tes
Sig
nifi
can
tm
ult
ivar
iate
rela
tio
nsh
ipb
etw
een
no
n-a
dh
eren
cean
dlo
wh
ealt
hli
tera
cy
Kal
ich
man
etal
.
[26
]
Cro
ss-s
ecti
on
al;
N=
14
5;
anti
-ret
rov
iral
ther
apy
;U
nit
ed
Sta
tes
Sig
nifi
can
tm
ult
ivar
iate
rela
tio
nsh
ipb
etw
een
no
n-a
dh
eren
cean
dlo
wh
ealt
hli
tera
cy
Osb
orn
eet
al.
[27
]
Cro
ss-s
ecti
on
al;
N=
39
8;
dia
bet
esm
edic
atio
n;
Un
ited
Sta
tes
Mix
edre
lati
on
ship
sb
etw
een
no
n-a
dh
eren
cean
dlo
wh
ealt
hli
tera
cyin
mu
ltiv
aria
tep
ath
mo
del
s
Paa
sch
e-O
rlo
w
etal
.[2
8]
Nes
ted
RC
T;
N=
23
5;
An
ti-r
etro
vir
alth
erap
y;
Un
ited
Sta
tes
Biv
aria
tere
lati
on
ship
bet
wee
nn
on
-ad
her
ence
and
low
hea
lth
lite
racy
that
did
no
tsu
rviv
em
ult
ivar
iate
adju
stm
ent
Co
lber
tet
al.
[31
]
Cro
ss-s
ecti
on
al;
N=
30
2;
HIV
med
icat
ion
;U
nit
edS
tate
sN
osi
gn
ifica
nt
po
siti
ve
rela
tio
nsh
ipb
etw
een
no
n-a
dh
eren
cean
dlo
wh
ealt
hli
tera
cy
Bh
or
etal
.[3
2]
Cro
ss-s
ecti
on
al;
N=
20
0;
Hy
per
ten
sio
nm
edic
atio
n;
Un
ited
Sta
tes
No
sig
nifi
can
tp
osi
tiv
ere
lati
on
ship
bet
wee
nn
on
-ad
her
ence
and
low
hea
lth
lite
racy
Gat
tiet
al.
[33]
Cro
ss-s
ecti
on
al;
N=
27
5;
Var
iou
sm
edic
atio
ns;
Un
ited
Sta
tes
No
sig
nifi
can
tp
osi
tiv
ere
lati
on
ship
bet
wee
nn
on
-ad
her
ence
and
low
hea
lth
lite
racy
Nav
arra
etal
.[3
5]
Cro
ss-s
ecti
on
al;
N=
50
HIV
-in
fect
edy
ou
th;
An
ti-
retr
ov
iral
ther
apy
;U
nit
edS
tate
s
No
sig
nifi
can
tp
osi
tiv
ere
lati
on
ship
bet
wee
nn
on
-ad
her
ence
and
low
hea
lth
lite
racy
Gra
ham
etal
.
[36
]
Cro
ss-s
ecti
on
al;
N=
87
;A
nti
-vir
alm
edic
atio
n;
Un
ited
Sta
tes
Sig
nifi
can
tm
ult
ivar
iate
rela
tio
nsh
ipb
etw
een
no
n-a
dh
eren
cean
dlo
wh
ealt
hli
tera
cy
Joy
ner
-
Gra
nth
amet
al.
[37
]
Cro
ss-s
ecti
on
al;
N=
85
;H
yp
erte
nsi
on
med
icat
ion
;
Un
ited
Sta
tes
No
sig
nifi
can
tp
osi
tiv
ere
lati
on
ship
bet
wee
nn
on
-ad
her
ence
and
low
hea
lth
lite
racy
Bau
eret
al.
[39
]C
ross
-sec
tio
nal
;N
=1
,36
6ad
ult
sw
ith
Ty
pe
IId
iab
etes
;
An
tid
epre
ssan
tm
edic
atio
n;
Un
ited
Sta
tes
Sig
nifi
can
tm
ult
ivar
iate
rela
tio
nsh
ipb
etw
een
no
n-a
dh
eren
cean
dlo
wh
ealt
hli
tera
cy
Wai
teet
al.
[40]
Cro
ss-s
ecti
on
al;
N=
20
4;
HIV
med
icat
ion
;U
nit
edS
tate
sS
ign
ifica
nt
mu
ltiv
aria
tere
lati
on
ship
bet
wee
nn
on
-ad
her
ence
and
low
hea
lth
lite
racy
Wal
dro
p-
Val
ver
de
etal
.
[41
]
Cro
ss-s
ecti
on
al;
N=
15
5;
‘‘M
ock
’’H
IVre
gim
en;
Un
ited
Sta
tes
Sig
nifi
can
tm
ult
ivar
iate
rela
tio
nsh
ipb
etw
een
adh
eren
cean
dh
ealt
hli
tera
cy
No
ure
ldin
etal
.
[42
]
RC
T;
N=
28
1;
Car
dio
vas
cula
rm
edic
atio
n;
Un
ited
Sta
tes
Mix
edre
lati
on
ship
sb
etw
een
no
n-a
dh
eren
cean
dlo
wh
ealt
hli
tera
cy
Wal
dro
p-
Val
ver
de
etal
.
[43
]
Cro
ss-s
ecti
on
al;
N=
57
;A
nti
-ret
rov
iral
med
icat
ion
;
Un
ited
Sta
tes
Mix
ed/c
on
fou
nd
edm
easu
reo
fre
lati
on
ship
bet
wee
nn
on
-ad
her
ence
and
low
hea
lth
lite
racy
Kri
pal
ani
etal
.
[44
]
Cro
ss-s
ecti
on
al;
N=
40
9;
Co
ron
ary
hea
rtd
isea
se
med
icat
ion
;U
nit
edS
tate
s
Mix
edre
lati
on
ship
sb
etw
een
no
n-a
dh
eren
cean
dlo
wh
ealt
hli
tera
cyin
clu
din
gb
ette
rad
her
ence
asso
ciat
edw
ith
low
erh
ealt
hli
tera
cy
Int J Clin Pharm (2014) 36:36–44 39
123
poor treatment knowledge [20]; poor medication knowl-
edge [20, 21]; impaired cognitive functioning [19]; having
a history of non-adherence [20]; hectic schedules/work
[22]; lack of social support [23–26]; education [23, 25];
socioeconomic status [23]; emotional distress [25, 26]; and
illness duration [27].
A history of alcohol problems, drinking to intoxication
and injecting drug use were also associated with poorer
adherence in a sample of 235 people living with HIV/AIDS
[28]. In another study among people living with HIV/AIDS
who had demonstrated low health literacy (n = 188), a
multivariate analysis showed that food insufficiency and
hunger predicted non-adherence over and above the effects
of depression, internalised stigma, substance abuse and
HIV-related social stressors [29]. In this research, adher-
ence was not related to gross cognitive functioning. Simi-
larly, general reading ability and understanding were not
associated with non-compliance in an older sample of 126
ambulatory care respondents from mixed socio-economic
backgrounds [30].
Patient beliefs are a distinct and important set of patient
factors. They include: beliefs about their disease [23];
unrealistic or uninformed expectations of risk, including
risk of adverse effects [23]; lack of self-efficacy [23, 31];
and disbelief about medication efficacy [23, 32, 33].
Medication related factors include: adverse effects [19,
34]; polypharmacy/multiple medications [19–21]; complex
medication regimens [20, 28]; safety concerns [20];
incomplete or confusing information on prescription labels
[22]; administrative processes (i.e., logistical factors) for
obtaining medications [20], intent to adhere and positive
outcome expectancy [35]; and higher adherence norms
[36].
Patient-provider relationship factors include: generally
having a poor relationship [23]; providers not fully
explaining how to take a medication [22]; and different
cultural models exacerbating distrust of the health system
[22].
A complex factor that does not fit easily into any of the
four categories above is cost. This is a clear barrier to
adherence for some people [23, 34] but can be considered a
combination of patient-related, medication-related and
logistical factors. Rust and Davis [34] reported the results
of an online survey of almost 10,000 adults with chronic
medical conditions which showed that not filling pre-
scriptions (primary non-adherence) or taking medication
incorrectly resulted from forgetfulness (24 %); side-effects
(20 %); cost (17 %); denial that medication was needed
(14 %); and inconvenience (10 %). A survey of 85 emer-
gency room patients found that they attributed their non-
adherence to inability to pay (36 %); feeling better (35 %);
feeling worse (25 %); and difficulty remembering to take
medication (32 %) [37]. Participant frustration withTa
ble
1co
nti
nu
ed
Ref
eren
ceS
tud
yd
escr
ipti
on
Co
ncl
usi
on
Kri
pal
ani
etal
.
[45
]
RC
T;
N=
42
0;
Car
dio
vas
cula
rm
edic
atio
ns;
Un
ited
Sta
tes
No
sig
nifi
can
tp
osi
tiv
ere
lati
on
ship
bet
wee
nn
on
-ad
her
ence
and
low
hea
lth
lite
racy
Ho
lzem
er(e
tal
.
[46
]
RC
T;
N=
11
8;
HIV
med
icat
ion
;U
nit
edS
tate
sN
osi
gn
ifica
nt
po
siti
ve
rela
tio
nsh
ipb
etw
een
no
n-a
dh
eren
cean
dlo
wh
ealt
hli
tera
cy
Mu
rph
yet
al.
[47
]
Cro
ss-s
ecti
on
al;
N=
18
6H
IV-i
nfe
cted
yo
uth
;H
IV
med
icat
ion
s;U
nit
edS
tate
s
No
sig
nifi
can
tp
osi
tiv
ere
lati
on
ship
bet
wee
nn
on
-ad
her
ence
and
low
hea
lth
lite
racy
Bai
ns
and
Eg
ede
[48
]
Cro
ss-s
ecti
on
al;
N=
12
5;
Dia
bet
esm
edic
atio
n;
Un
ited
Sta
tes
No
sig
nifi
can
tp
osi
tiv
ere
lati
on
ship
bet
wee
nn
on
-ad
her
ence
and
low
hea
lth
lite
racy
Fan
get
al.
[49
]C
ross
-sec
tio
nal
;N
=1
79
;W
arfa
rin
;U
nit
edS
tate
sN
osi
gn
ifica
nt
po
siti
ve
rela
tio
nsh
ipb
etw
een
no
n-a
dh
eren
cean
dlo
wh
ealt
hli
tera
cy
Gaz
mar
aria
n
etal
.[5
0]
Pro
spec
tiv
e;N
=1
,54
9;
Var
iou
sm
edic
atio
ns;
Un
ited
Sta
tes
Biv
aria
tere
lati
on
ship
bet
wee
nn
on
-ad
her
ence
and
low
hea
lth
lite
racy
that
did
no
tsu
rviv
em
ult
ivar
iate
adju
stm
ent
40 Int J Clin Pharm (2014) 36:36–44
123

inconsistent health information from doctors and pharma-
cists was reported from focus groups among underserved
African American women (n = 24) who had completed
breast cancer treatment at least one year previously [34].
Many of these women reported receiving information
through churches, community centres, and word of
mouth—with the attendant possibility of misinformation.
Participants also showed differing levels of satisfaction in
seeking information, particularly from ‘busy’ pharmacists.
Relationship between non-adherence and health literacy
A systematic review of research on the relationship
between non-adherence with diabetes or cardiovascular
medication and health literacy, found no consistent links in
the seven relevant studies reviewed [38]. Bivariate rela-
tionships were identified in some cases but did not hold up
to adjustment in multivariate analysis, primarily with
demographic variables. Contrary to expectations, one study
found lower health literacy associated with higher self-
reported medication adherence. In a secondary finding, a
number of studies showed a relationship between health
literacy and disease or medication knowledge, while
showing no association with greater medication adherence
[38].
A relationship was found between non-adherence and
health literacy in five of the 23 articles reporting original
research into the relationship [25, 26, 39–41]. Most of these
were well-designed studies, unlike the Kalichman et al.
[25] study, which had a small sample and where the rela-
tionship was only positive for respondents with a greater
number of years of education. Waldrop-Valverde et al. [41]
reported a very carefully designed study that was however,
unusual in using a simulated measure of adherence. While
this standardised the measurement procedure it leaves
some question about the ecological validity of the results.
Bauer et al. [39] used a screening measure of health liter-
acy that is rarely used, reporting associations between
health literacy and medication non-persistence before the
first refill and at 180 days but not for primary non-adher-
ence (in any analysis) or non-persistence at 365 days in
multivariate analysis [39].
Four studies reported mixed results [27, 42–44]. A lar-
ger cumulative medication gap was associated with low
health literacy in the Kripalani et al. [44] study but self-
reported adherence was not. Noureldin et al. [42] con-
ducted a well-designed RCT but only found an association
between non-adherence and health literacy for two of seven
adherence measures in the usual care arm of the study.
Osborn et al. [27] reported the results of a path analysis
which only showed a relationship between non-adherence
and health literacy when numeracy was included in the
path model. Finally, the study reported by Waldrop-
Valverde et al. [43] confounded health literacy and cog-
nitive functioning, showing adherence to be associated
with a group low in cognition health literacy. This study
also had a very small sample (n = 57).
A clear majority of articles in this review (15 of 23),
reported not finding significant positive relationships
between non-adherence and low health literacy [21, 28,
31–33, 35, 37, 42, 44–50]. Some of these studies had small
sample sizes and consequently likely had low power to
detect a relationship. However, most were well-designed
cross-sectional studies with reasonable samples; two stud-
ies used a randomized controlled trial design [28, 45]; and
Gazmararian et al. [50] had the advantage of using a pro-
spective design in a large, ethnically and geographically
diverse population, using a preferred measure of adherence
[51].
Two of the 15 studies found a bivariate relationship
between health literacy and non-adherence that did not
survive adjustment for the effects of other relevant vari-
ables in multivariate analysis [28, 50]. Counter-intuitively,
better adherence was associated with lower health literacy
for a self-report measure of adherence in the study reported
by Kripalani et al. [44].
Potential mechanisms for an association between health
literacy and non-adherence
Factors found to be associated with non-adherence, which
may have a role in the relationship between health literacy
and non-adherence, include education, cognitive function-
ing, relevant knowledge, information sources, social sup-
port and self-efficacy. The Loke et al. [38] review found
that health literacy was associated with disease and medi-
cation knowledge. Although research has also shown these
factors to be associated with non-adherence, they have not
been found to result in a relationship between health lit-
eracy and non-adherence.
Research that directly addresses potential mechanisms
in any relationship between non-adherence and health lit-
eracy is rare. In one of two such examples identified in this
review, a finding that many patients in a hospital emer-
gency room sample felt that nothing they did would help
their blood pressure, was used to explain the fact that they
did not take medications despite good health knowledge/
literacy about blood pressure [37]. This suggests that these
patients had low self-efficacy, and implicitly, low medi-
cation efficacy beliefs as well.
In another study, reasons for medication discrepancies
48 h after hospital discharge among 254 community-
dwelling seniors (70 years or older) differed across health
literacy levels [52]. Discrepancies for those with inade-
quate or marginal health literacy were significantly asso-
ciated with lack of understanding about how to take the
Int J Clin Pharm (2014) 36:36–44 41
123
medication (unintentional non-adherence). In contrast,
people with adequate health literacy were significantly
more likely to have medication discrepancies as a result of
choosing not to follow instructions—despite understanding
those instructions [52].
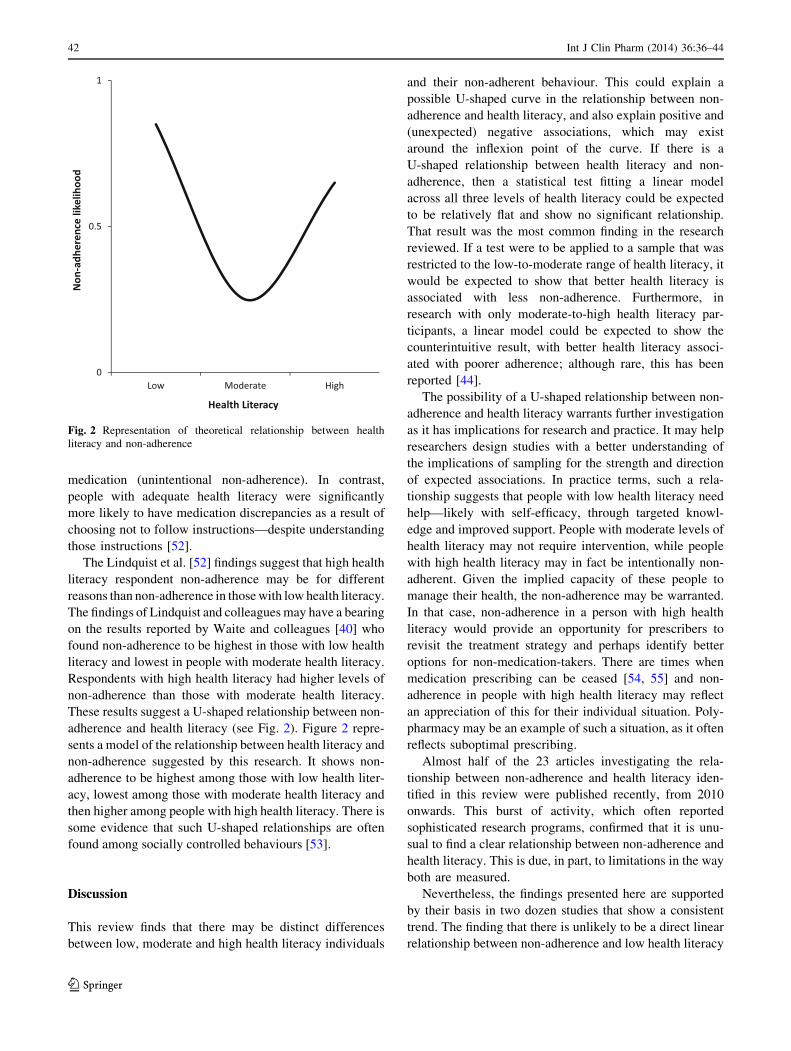
The Lindquist et al. [52] findings suggest that high health
literacy respondent non-adherence may be for different
reasons than non-adherence in those with low health literacy.
The findings of Lindquist and colleagues may have a bearing
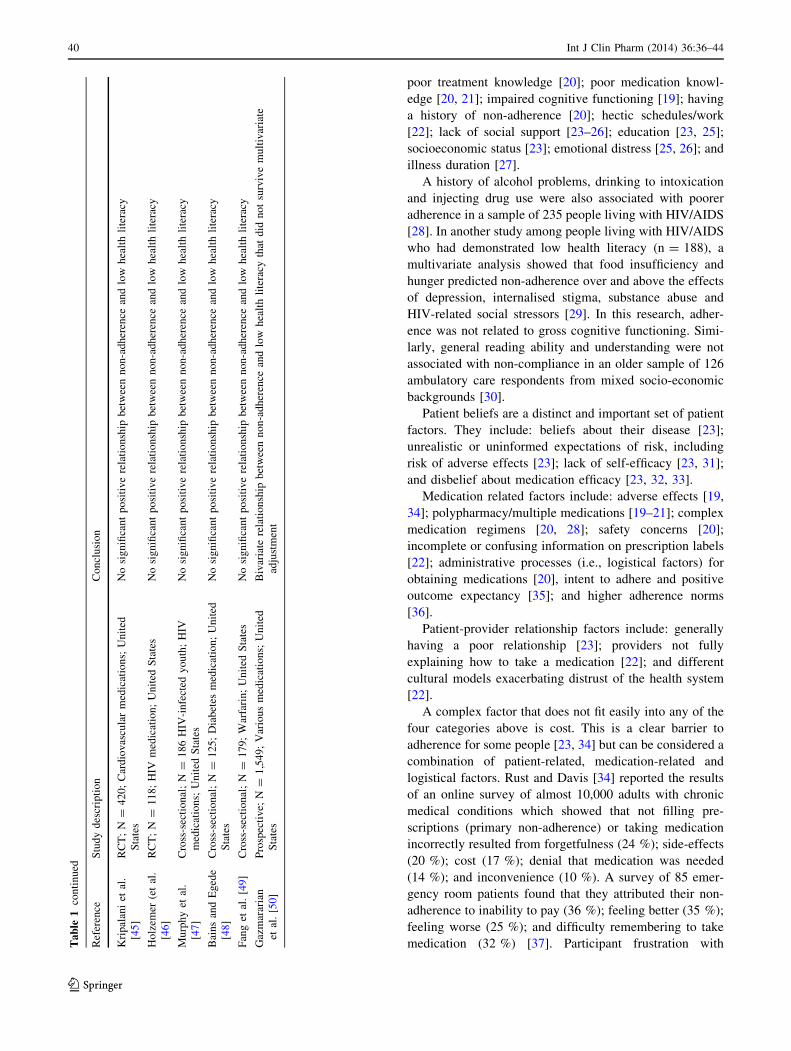
on the results reported by Waite and colleagues [40] who
found non-adherence to be highest in those with low health
literacy and lowest in people with moderate health literacy.
Respondents with high health literacy had higher levels of
non-adherence than those with moderate health literacy.
These results suggest a U-shaped relationship between non-
adherence and health literacy (see Fig. 2). Figure 2 repre-
sents a model of the relationship between health literacy and
non-adherence suggested by this research. It shows non-
adherence to be highest among those with low health liter-
acy, lowest among those with moderate health literacy and
then higher among people with high health literacy. There is
some evidence that such U-shaped relationships are often
found among socially controlled behaviours [53].
Discussion
This review finds that there may be distinct differences
between low, moderate and high health literacy individuals
and their non-adherent behaviour. This could explain a
possible U-shaped curve in the relationship between non-
adherence and health literacy, and also explain positive and
(unexpected) negative associations, which may exist
around the inflexion point of the curve. If there is a
U-shaped relationship between health literacy and non-
adherence, then a statistical test fitting a linear model
across all three levels of health literacy could be expected
to be relatively flat and show no significant relationship.
That result was the most common finding in the research
reviewed. If a test were to be applied to a sample that was
restricted to the low-to-moderate range of health literacy, it
would be expected to show that better health literacy is
associated with less non-adherence. Furthermore, in
research with only moderate-to-high health literacy par-
ticipants, a linear model could be expected to show the
counterintuitive result, with better health literacy associ-
ated with poorer adherence; although rare, this has been
reported [44].
The possibility of a U-shaped relationship between non-
adherence and health literacy warrants further investigation
as it has implications for research and practice. It may help
researchers design studies with a better understanding of
the implications of sampling for the strength and direction
of expected associations. In practice terms, such a rela-
tionship suggests that people with low health literacy need
help—likely with self-efficacy, through targeted knowl-
edge and improved support. People with moderate levels of
health literacy may not require intervention, while people
with high health literacy may in fact be intentionally non-
adherent. Given the implied capacity of these people to
manage their health, the non-adherence may be warranted.
In that case, non-adherence in a person with high health
literacy would provide an opportunity for prescribers to
revisit the treatment strategy and perhaps identify better
options for non-medication-takers. There are times when
medication prescribing can be ceased [54, 55] and non-
adherence in people with high health literacy may reflect
an appreciation of this for their individual situation. Poly-
pharmacy may be an example of such a situation, as it often
reflects suboptimal prescribing.
Almost half of the 23 articles investigating the rela-
tionship between non-adherence and health literacy iden-
tified in this review were published recently, from 2010
onwards. This burst of activity, which often reported
sophisticated research programs, confirmed that it is unu-
sual to find a clear relationship between non-adherence and
health literacy. This is due, in part, to limitations in the way
both are measured.
Nevertheless, the findings presented here are supported
by their basis in two dozen studies that show a consistent
trend. The finding that there is unlikely to be a direct linear
relationship between non-adherence and low health literacy
Fig. 2 Representation of theoretical relationship between health
literacy and non-adherence
42 Int J Clin Pharm (2014) 36:36–44
123

undermined the goal of this review to identify mechanisms
linking heath literacy and adherence. However, the results
of this review also point toward two potentially fruitful
avenues of investigation. One promising activity is to
untangle the ways in which health literacy, self-efficacy
and medication use are interrelated. The second area that
promises greater clarity involves directly investigating the
strength of the proposition that low health literacy and non-
adherence are non-linearly related.
Investigating non-adherence within a health literacy
framework can place the focus of medication taking on the
potential medication-taker in a non-judgemental way, by
highlighting the many interconnected components that con-
tribute to a person’s ability to manage their health in the
context of medication taking. A prescriber’s recommendation
to take a medicine is one factor in the broad health literacy
context; it may not, in practice, be the most influential factor.
In many situations, this can lead to poor health outcomes. In
some situations, non-adherence to the prescriber’s recom-
mendation may be the most appropriate outcome for a patient.
Understanding this framework will help researchers and cli-
nicians realise that the goal of eliminating all instances of non-
adherence is mistaken, and will contribute to the development
of more effective means of reducing non-adherence when that
non-adherence is not in the patient’s best interests.
Conclusion
The evidence is clear that medication knowledge alone is
insufficient for addressing non-adherence, and that addressing
non-adherence within the framework of health literacy is not
as straightforward as was initially assumed. Medication fac-
tors and self-efficacy influence medication-taking and must be
considered as part of the health literacy equation.
Funding None.
Conflicts of interest None.
References
1. Bush RA, Boyle F, Ostini R, Ozolins I, Brabant M, Soto EJ, et al.
Advancing health literacy through primary health care systems.
Canberra: Australian Primary Health Care Research Institute;
2009.
2. Dewalt DA, Berkman ND, Sheridan S, Lohr KN, Pignone MP.
Literacy and health outcomes: a systematic review of the litera-
ture. J Gen Intern Med. 2004;19(12):1228–39.
3. Keller DL, Wright J, Pace HA. Impact of health literacy on health
outcomes in ambulatory care patients: a systematic review. Ann
of Pharmacother. 2008;42(9):1272–81.
4. Pignone MP, DeWalt DA. Literacy and health outcomes: is
adherence the missing link? J Gen Intern Med. 2006;21(8):896–7.
5. Ratzan SC, Parker RM. Introduction. In: Selden CR, Zorn M,
Ratzan SC, Parker RM, editors. National library of medicine
current bibliographies in medicine: health literacy. NLM Pub.
No. CBM 2000-1. Bethesda, MD: National Institutes of Health,
U.S. Department of Health and Human Services; 2000.
6. Parker RM, Baker DW, Williams MV, Nurss JR. The test of
functional health literacy in adults: a new instrument for measuring
patients’ literacy skills. J Gen Intern Med. 1995;10(10):537–41.
7. Davis TC, Crouch MA, Long SW, Jackson RH, Bates P, George
RB, et al. Rapid assessment of literacy levels of adult primary
care patients. Fam Med. 1991;23(6):433–5.
8. Davis TC, Long SW, Jackson RH, Mayeaux EJ, George RB,
Murphy PW, et al. Rapid estimate of adult literacy in medicine: a
shortened screening instrument. Fam Med. 1993;25(6):391–5.
9. Nutbeam D. The evolving concept of health literacy. Soc Sci
Med. 2008;67(12):2072–8.
10. World Health Organization. Adherence to long-term therapies: evi-
dence for action; 2003. Cited 2013 August 17. Available from: http://
www.who.int/chp/knowledge/publications/adherence_report/en/.
11. Nutbeam D. Health promotion glossary. Health Promot Int.
1998;13(4):349–64.
12. Balkrishnan R. Predictors of medication adherence in the elderly.
Clin Thera. 1998;20(4):764–71.
13. Vrijens B, Geest SD, Hughes DA, Przemyslaw K, Demonceau J,
Ruppar T, et al. A new taxonomy for describing and defining
adherence to medications. B J Clin Pharmacol. 2012;73(5):691–705.
14. Gerth WC. Compliance and Persistence with Newer Antihyper-
tensive Agents. Curr Hypertens Rep. 2002;4:424–33.
15. Wride N, Finch T, Rapley T, Moreira T, May C, Fraser S. What’s
in a name? Medication terms: what they mean and when to use
them. B J Opthalmol. 2007;91:1422–4.
16. Blackwell B. Compliance. Psychother Psychosom. 1992;58:161–9.
17. U.S. National Library of Medicine. MEDLINE/PubMed search
and health literacy information. Bethesda, MD2011 [cited 2013
April 26]; Available from: http://www.nlm.nih.gov/services/
queries/health_literacy.html.
18. Ngoh LN. Health literacy: a barrier to pharmacist-patient com-
munication and medication adherence. J Am Pharm Assoc.
2009;49(5):e132–46.
19. Gellad WF, Grenard JL, Marcum ZA. A systematic review of
barriers to medication adherence in the elderly: looking beyond
cost and regimen complexity. Am J Geriatr Pharmacother.
2011;9(1):11–23.
20. Campbell NL, Boustani MA, Skopelja EN, Gao S, Unverzagt
FW, Murray MD. Medication adherence in older adults with
cognitive impairment: a systematic evidence-based review. Am J
Geriatr Pharmacother. 2012;10(3):165–77.
21. Mosher HJ, Lund BC, Kripalani S, Kaboli PJ. Association of
health literacy with medication knowledge, adherence, and
adverse drug events among elderly veterans. J Health Commun.
2012;17(Suppl 3):241–51.
22. Mohan AV, Riley MB, Boyington DR, Kripalani S. Illustrated
medication instructions as a strategy to improve medication
management among Latinos: a qualitative analysis. J Health
Psychol. 2013;18(2):187–97.
23. Elliott RA, Marriott JL. Standardised assessment of patients’
capacity to manage medications: a systematic review of pub-
lished instruments. BMC Geriatr. 2009;9:27.
24. Johnson VR, Jacobson KL, Gazmararian JA, Blake SC. Does
social support help limited-literacy patients with medication
adherence? A mixed methods study of patients in the pharmacy
intervention for limited literacy (PILL) study. Patient Educ
Couns. 2010;79(1):14–24.
25. Kalichman SC, Ramachandran B, Catz S. Adherence to combi-
nation antiretroviral therapies in HIV patients of low health lit-
eracy. J Gen Intern Med. 1999;14(5):267–73.
Int J Clin Pharm (2014) 36:36–44 43
123
26. Kalichman SC, Pope H, White D, Cherry C, Amaral CM, Swe-
tzes C, et al. Association between health literacy and HIV
treatment adherence: further evidence from objectively measured
medication adherence. J Int Assoc Physicians AIDS Care (Chic).
2008;7(6):317–23.
27. Osborn CY, Cavanaugh K, Wallston KA, Kripalani S, Elasy TA,
Rothman RL, et al. Health literacy explains racial disparities in
diabetes medication adherence. J Health Commun. 2011;16(Suppl
3):268–78.
28. Paasche-Orlow MK, Cheng DM, Palepu A, Meli S, Faber V,
Samet JH. Health literacy, antiretroviral adherence, and HIV-
RNA suppression: a longitudinal perspective. J Gen Intern Med.
2006;21(8):835–40.
29. Kalichman SC, Grebler T. Stress and poverty predictors of
treatment adherence among people with low-literacy living with
HIV/AIDS. Psychosom Med. 2010;72(8):810–6.
30. Moisan J, Gaudet M, Gregoire JP, Bouchard R. Non-compliance
with drug treatment and reading difficulties with regard to pre-
scription labelling among seniors. Gerontology. 2002;48(1):44–51.
31. Colbert AM, Sereika SM, Erlen JA. Functional health literacy,
medication-taking self-efficacy and adherence to antiretroviral
therapy. J Adv Nurs. 2013;69(2):295–304.
32. Bhor M, Plake KS, Chen JT. Relationship between health liter-
acy, outcome expectations, efficacy expectations and medication
adherence. Value in Health. 2009;12(3):A155.
33. Gatti ME, Jacobson KL, Gazmararian JA, Schmotzer B, Kripa-
lani S. Relationships between beliefs about medications and
adherence. Am J Health Syst Pharm. 2009;66(7):657–64.
34. Rust C, Davis C. Health literacy and medication adherence in
underserved African-american breast cancer survivors: a quali-
tative study. Soc Work Health Care. 2011;50(9):739–61.
35. Navarra AM, Neu N, Toussi S, Nelson J, Larson EL. Health
literacy and adherence to antiretroviral therapy among hiv-
infected youth. J Assoc Nurses AIDS Care. 2013; 1–11.
36. Graham J, Bennett IM, Holmes WC, Gross R. Medication beliefs as
mediators of the health literacy-antiretroviral adherence relationship
in HIV-infected individuals. AIDS Behav. 2007;11(3):385–92.
37. Joyner-Grantham J, Mount DL, McCorkle OD, Simmons DR,
Ferrario CM, Cline DM. Self-reported influences of hopelessness,
health literacy, lifestyle action, and patient inertia on blood
pressure control in a hypertensive emergency department popu-
lation. Am J Med Sci. 2009;338(5):368–72.
38. Loke YK, Hinz I, Wang X, Salter C. Systematic review of con-
sistency between adherence to cardiovascular or diabetes medi-
cation and health literacy in older adults. Ann Pharmacother.
2012;46(6):863–72.
39. Bauer AM, Schillinger D, Parker MM, Katon W, Adler N, Adams
AS, et al. Health literacy and antidepressant medication adher-
ence among adults with diabetes: the diabetes study of Northern
California (DISTANCE). J Gen Intern Med. 2013; 1181–7.
40. Waite KR, Paasche-Orlow M, Rintamaki LS, Davis TC, Wolf
MS. Literacy, social stigma, and HIV medication adherence.
J Gen Intern Med. 2008;23(9):1367–72.
41. Waldrop-Valverde D, Jones DL, Jayaweera D, Gonzalez P, Ro-
mero J, Ownby RL. Gender differences in medication manage-
ment capacity in HIV infection: the role of health literacy and
numeracy. AIDS Behav. 2009;13(1):46–52.
42. Noureldin M, Plake KS, Morrow DG, Tu W, Wu J, Murray MD.
Effect of health literacy on drug adherence in patients with heart
failure. Pharmacother. 2012;32(9):819–26.
43. Waldrop-Valverde D, Jones DL, Weiss S, Kumar M, Metsch L.
The effects of low literacy and cognitive impairment on medi-
cation adherence in HIV-positive injecting drug users. AIDS
Care. 2008;20(10):1202–10.
44. Kripalani S, Gatti ME, Jacobson TA. Association of age, health
literacy, and medication management strategies with cardiovascular
medication adherence. Patient Educ Couns. 2010;81(2):177–81.
45. Kripalani S, Schmotzer B, Jacobson T. Improving medication
adherence through graphically enhanced interventions in coro-
nary heart disease (IMAGE-CHD): a randomized controlled trial.
JGIM. 2012;27(12):1609–17.
46. Holzemer WL, Bakken S, Portillo CJ, Grimes R, Welch J,
Wantland D, et al. Testing a nurse-tailored HIV medication
adherence intervention. Nurs Res. 2006;55(3):189–97.
47. Murphy DA, Lam P, Naar-King S, Robert Harris D, Parsons JT,
Muenz LR. Health literacy and antiretroviral adherence among
HIV-infected adolescents. Patient Educ Couns. 2010;79(1):25–9.
48. Bains SS, Egede LE. Associations between health literacy, dia-
betes knowledge, self-care behaviours, and glycemic control in a
low income population with type 2 diabetes. Diabetes Technol
Ther. 2011;13(3):335–41.
49. Fang MC, Machtinger EL, Wang F, Schillinger D. Health literacy
and anticoagulation-related outcomes among patients taking
warfarin. J Gen Intern Med. 2006;21(8):841–6.
50. Gazmararian JA, Kripalani S, Miller MJ, Echt KV, Ren J, Rask
K. Factors associated with medication refill adherence in car-
diovascular-related diseases: a focus on health literacy. J Gen
Intern Med. 2006;21(12):1215–21.
51. Powers BJ, Bosworth HB. Revisiting literacy and adherence:
future clinical and research directions. J Gen Intern Med.
2006;21(12):1341–2.
52. Lindquist LA, Go L, Fleisher J, Jain N, Friesema E, Baker DW.
Relationship of health literacy to intentional and unintentional
non-adherence of hospital discharge medications. J Gen Intern
Med. 2012;27(2):173–8.
53. Orford J. Excessive appetites: a psychological view of addictions.
2nd ed. Chichester: John Wiley and Sons; 2001.
54. Ostini R, Jackson C, Hegney D, Tett SE. How is medication pre-
scribing ceased? A systematic review. Med Care. 2011;49(1):24–36.
55. Ostini R, Hegney D, Jackson C, Tett SE. Knowing how to stop:
ceasing prescribing when the medicine is no longer required.
J Manag Care Pharm. 2012;8(1):68–72.
44 Int J Clin Pharm (2014) 36:36–44
123