Embed Size (px)
Citation preview

Investigating PPP Health Model – Chiranjeevi Yojana District : Sabarkantha, Gujarat
Anuja Kastia, Research Officer CEHAT
Dr Ramila Bisht, Associate Professor, JNU


Area Profile- Sabarkantha District - One of the pilot district where CY was
started.- Total population - 20,82,531
173,325 is scheduled caste (8.32%) 420,242 is the schedule tribe (20.18%).
Bhil, other Generic tribes and Naikda comprises of the three largest tribes in the district
10 blocks - Khedbhrama situated on the northern side of Sabarkantha
district and has a population of 2,50,289 and over 137 villages. (census 2001)
- Khedbhrama is one of the poorest performing blocks in CY (district data source).
- Approximately 70% of the population is Tribal population.

Maternal and Child health indicators of Tribal population .vs. General population.
Table showing the comparative scenario of maternal and child health indicators of Tribal population and General population.
Indicator/Outreach Tribal population General population
Maternal Mortality 16% 10%
Infant Mortality 83% 61.80%
Child Mortality 46.30% 22.20%
Fully immunized children 26.40% 46.80%
Anaemic children 79.80% 72.70%
Anaemic mother 64.90% 47.60%
Antenatal checked mothers 34.70% 56.50%
Institutionalized delivery 17.10% 40.10%
Data source: NFHS II / 2000

Aims & Objectives
Explore the Program Reach in Study Area Study the Mechanism & Operation of Scheme Examine the reasons for Non Adoption of the
Scheme Perception of Private Practioners in the Study
Area Encompass View Point of Stakeholders & State
towards Chiranjeevi Yojana

Research Methodology
Exploratory in Nature Research Tool : Semi structured Interviews,
Observation Sampling : Purposive / snow ball Site : selected villages of Khedbrahma Period of Research : April ‘08 – May ‘08 Sample Size : 32 women

Nature of the Data set and Analysis
Type Qualitative Quantative
Analysis Manually coded SPSS
and Thematically
analyzed

Profile of the women
All the 32 women were BPL women. Heterogeneous Minimum age – 20 where as maximum was 45
years 30 – Hindu, 2 – Muslim women. 68.7% ST, 12.5% SC, and 9.3 % General and
OBC category All with different obstetric history. Peculiar cultural practices in the area –
engagement of the men of the family in delivery process.

FINDINGSReach of the scheme
Mechanism and Operation of the Scheme in the study area.

Program Reach - SabarkanthaDistrict Nature of Delivery (2006 – 2008 )
Normal Lower Segment Cesarian Section (LSCS)
Complicated Total % LSCS
Banaskantha 14571 833 1095 16499 5
Dahod 15882 669 4614 21165 3.2
Kutch 6947 456 2417 9820 4.6
Panchmahal 24651 922 424 25997 3.5
Sabarkantha 16606 1754 529 18889 9.3
Rest of Gujarat
65225 5644 2039 72908 7.7
TOTAL 143882 10278 11118 165278 6.2
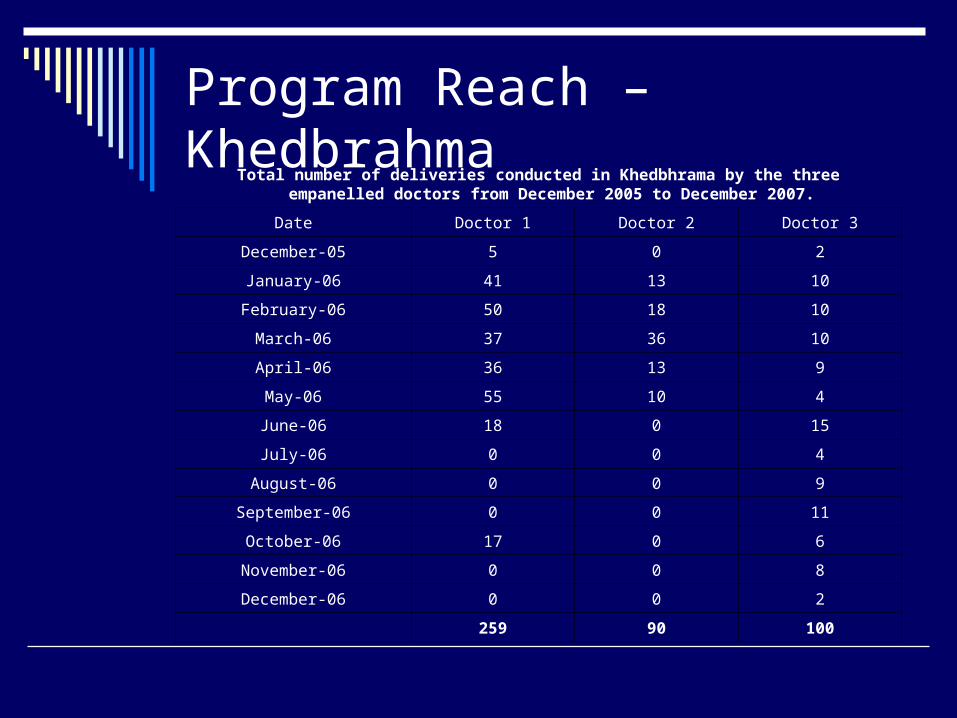
Program Reach –KhedbrahmaTotal number of deliveries conducted in Khedbhrama by the three empanelled doctors from
December 2005 to December 2007.
Date Doctor 1 Doctor 2 Doctor 3
December-05 5 0 2
January-06 41 13 10
February-06 50 18 10
March-06 37 36 10
April-06 36 13 9
May-06 55 10 4
June-06 18 0 15
July-06 0 0 4
August-06 0 0 9
September-06 0 0 11
October-06 17 0 6
November-06 0 0 8
December-06 0 0 2
259 90 100

Program Reach - KhedbrahmaTotal number of deliveries conducted in Khedbhrama by the three empanelled doctors
from December 2005 to December 2007.
Date Doctor 1 Doctor 2 Doctor 3
February-07 0 0 0
March-07 0 0 0
April-07 17 0 4
May-07 47 0 0
June-07 46 0 7
July-07 53 0 2
August-07 61 0 3
September-07 81 0 0
October-07 28 0 4
November-07 12 0 1
December-07 42 0 6
387 0 34
total deliveries under CY in 2007-2008 is 421
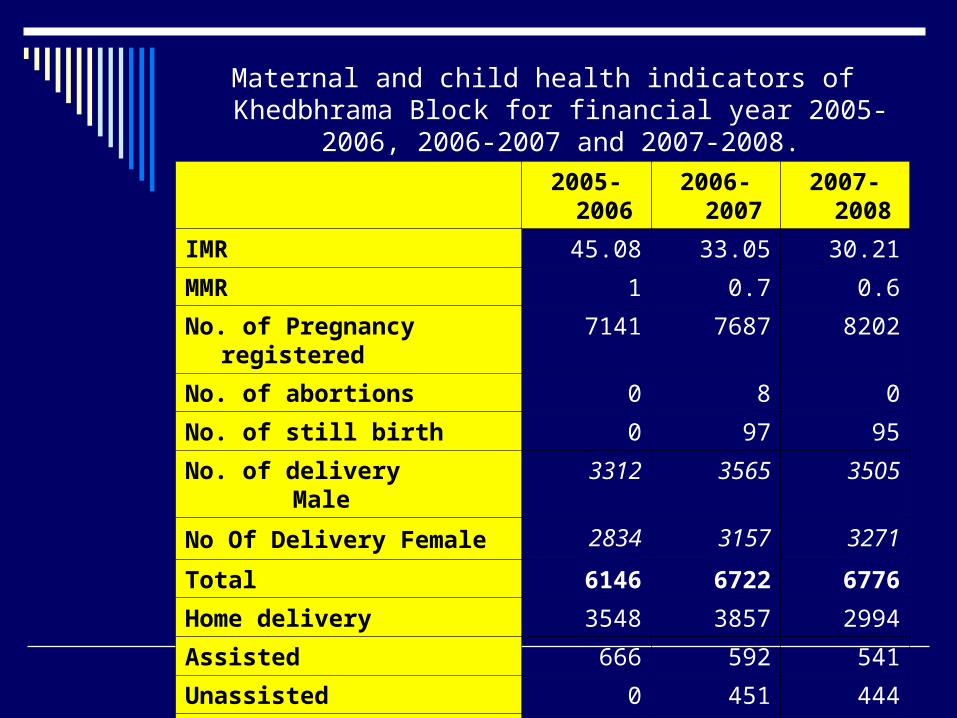
Maternal and child health indicators of Khedbhrama Block for financial year 2005-2006, 2006-2007 and 2007-2008.
2005-2006 2006-2007 2007-2008
IMR 45.08 33.05 30.21
MMR 1 0.7 0.6
No. of Pregnancy registered 7141 7687 8202
No. of abortions 0 8 0
No. of still birth 0 97 95
No. of delivery Male 3312 3565 3505
No Of Delivery Female 2834 3157 3271
Total 6146 6722 6776
Home delivery 3548 3857 2994
Assisted 666 592 541
Unassisted 0 451 444
No. of trained dias 2667 2750 1974
No. of untrained Dais 215 64 35
Source: District Project Unit, Sabarkantha. May 2008

Reasons For Non Adoption
No Awareness of the Scheme amongst Target Population
Awareness of the Scheme but did’nt opt due to
-Distance- High Expenditure- Fear, Beliefs, Trust- Family Pressure- Bad Past Experience

It is not only knowledge about the scheme which determines the decision of these women
“I’ll still prefer to got to poshina (to the local doctor)” “Our people would prefer here only” “tempo is so costly………even if we want it is not
possible.” “No, not at all, it is very far and it is not that we are given
sarkari gaadi.” “ it is not that one person goes for the delivery, so many
relatives goes and their tea snacks also costs money” “The doctor should be in poshina. If it is near, then it is
easy to go. “My pain started in the night, so we cannot reach there in
time in such times.”

Cross tab showing Institutionalized and non-institutionalized deliver and the knowledge of Chiranjeevi Yojana
Don’t Know
Know Some knowledge
Total
Institutional
11(34.4%) 5(15.6%) 2(6.3%) 18(56.3%)
delivery
Home
13(40.6%) 0(.0%) 1(3.1%) 14(43.8%)
Delivery
Total
24(75.0%) 5(15.6%) 3(9.4%) 32(100%)75% of the women did not know anything about the scheme

Views of associated doctors with the Scheme
“In emergency situations of blood requirement, even if the patient is under the scheme, I will have to refer it to Idar”
“Unless and until Government takes some action against those doctors (referring to unqualified doctors) there is nothing which is going to happen. I have come across patients wherein they have come to me in worst of condition, one came where the hand of the newborn was tried to be taken out from the anal canal instead of the normal opening”
“Once I got a woman with haemoglobin - 6, I don’t know what kind of ANC is carried out in the field. I didn’t take up that case, I had to refer”
Perception of un-qualified doctors operating in the field
“We are practicing from more than 15 to 20 years at this place. Weekly I carry out so many deliveries, if Government ties up with people like me, it would be so beneficial to them, we would do each delivery in 500 to 700 Rs.”
ARGUMENT :
Institutionalized, Attended yet not medically legalized

Voices on the Ground….ANM s
“I have to walk so much to each of these houses, one house is on this top and one is on that top, and that too with the vaccination bag in this much of heat… it is very difficult” – ANM
“It is very risky to work after 5’ o clock. It is very common to find drunken men on the streets. I have heard comments so many times, but then over a period of time I learned how to manage”- ANC
“During rainy season, the whole path gets blocked, I choose a home, and open my vaccination box here, and the male health worker calls the mothers”, some of them come, some don’t, but what to do.” – ANC
“we go to their place and tell them everything, we give them tablets, (which they sometimes eat and sometimes don’t eat

Views from State Officials
“There are so few doctors in the area”, what to do?”
“In proper Khedbhrama CHC too, there is no General Surgeon or Gynecologist more than last 10 years, forget about Poshina CHC……no one wants to come and work in these areas”
Common feeling was scheme should remain on-going
Also showed helplessness with the number of doctors in the area and how sustaining the partnership making becomes difficult in such circumstances.

Few limitations and experiences during the study
- Non presence of a NGO working in health - Not being able to capture the level of education
variable- Environment during interviewing (Sitting
arrangement, Presence of male member)- Apprehension / reluctance – ‘here you come
again……- Dialect- Exposure to tribal practices/beliefs

CONCLUDING REMARKS
Besides intensifying CY, the area cries a crucial need to review the aims of reducing MMR, IMR among the population in back drop of a high level of unassisted home deliveries and the peculiar socio-cultural environment.
Requires reviewing of partnership and related issues and move beyond CY in terms of having a micro plan to reduce IMR and MMR.
Policy Level Recommendations Detailed research study which would elucidate the
reach within the tribal pockets is essential for greater understanding of the barriers in the scheme.
The efforts to fill the vacant post in public health department of the block need consideration.
The awareness building activities of the CY requires scaling up for better reach in the interior pockets.
The vigilant monitoring is required by the block and district health functionaries in order to see that no monetary gains are achieved by the associated doctors. This would further help in restricting any unpleasant experience to the women and help in promotion of the scheme
In terms of monitoring the progress of the scheme, the analysis of reach needs to be calculated against the total deliveries among vulnerable population.
Tribal Development Budget and District allocation to the block needs to converge.





























