Holy Angel University Angeles City, Pampanga College of Nursing
In Partial Fulfillment of the Requirements in Nursing Care
Management - Related Learning Experience 103 Jose B. Lingad
Memorial Regional Hospital OB Ward
Case study on:
Inverted UterusSubmitted by: N-301 Dizon, Crisfer Gonzales,
April Jamaica Liew, Louie Andrew Pradilla, Angelica Quedit, Jennine
Rosario, Annie Grace Sagcal, Ramil Samson, Evangeline Soriano, Mary
Grace Tayag, Patrisha
Submitted to: Eliezer R. Dizon RN, Ph.D. Date of Submission:
August 8, 2011
TABLE OF CONTENTS I. Introduction 1 2 2 2 2 3 3 3 4-6 7-8 9-11 9
9 9 10-11 12 12-15 13-14 15 15 20-21 22-23 24
II. Personal Data A. Demographic Data B. Activities of Daily
Living C. Socioeconomic, Religion, Cultural Beliefs and Practices
III. History of Past and Present Illness A. Obstetric History B.
History of Present Illness IV. Diagnostic Procedures V. Anatomy and
Physiology VI. Pathophysiology A.Definition B.Predisposing and
Precipitating Factors C.Signs and Symptoms D.Schematic Diagram VII.
Treatment and Management A. Surgical Intervention B. Drug Study C.
Diet D. Activity VIII. Nursing Care Plan
IX. Problems and Difficulties Encountered X. Bibliography
I. IntroductionUterine inversion during the acute postpartum
period is a relatively rare complication. Severe post-partum
hemorrhage and shock result from the uterine fundus collapsing. If
unrecognized, this obstetric emergency could cause serious
morbidity or death. Most commonly, the frequency is reported to be
approximately 1 in 2000 deliveries. Maternal mortality has been
reported to be as high as 15%. Treatment options for this obstetric
complication are also quite varied. Several pharmacologic methods,
as well as manual and surgical options, have been described for
correcting an inversion. The most important aspect of treatment
remains immediate recognition and prompt attention to its
management. Following is a case report of complete uterine
inversion with a discussion of classification, etiology, diagnosis,
and methods of treatment for this lifethreatening obstetric event.
Objectives: After the 2 days of Nurse Patient Interaction the
student nurse will be able to:
Gather demographic, socioeconomic and cultural data of the
patient as well as her maternal history. Enumerate the diagnostic
and laboratory procedures done with the patient. Identify the
anatomy and physiology of female reproductive system. Identify and
make out a pathophysiology of the condition of patient (inverted
Uterus), its synthesis, definition, precipitating, and predisposing
factor. Itemize the surgical/ medical management done in the
patient including the IVF and formulate a drug study of all drugs
given in the patient. Specify the diet and exercise of the patient
from the admission to discharge. Make out a nursing care plan of
the problems and needs of the patient Design a health teaching
plans for the patient.
1
II.Personal DataA.Demographic Data
Mrs. Marie is a 26 years old plain housewife who lives in Dau,
Mabalacat Pampanga. She was born on March 9, 1985. Her education
attainment is third year high school. According to her she didnt
finish her study because of financial constraints. They have 3
siblings already. The first one is a 7 years old boy, second is a 4
years old boy and third is the newly born baby girl.
B.Activities of Daily Living
At 5:30 am, Mrs. Marie wakes up to cook breakfast for her
husband who will go at work. Then at 7:00 am, she will ready her
son who will be going to the school. At 8:00 am she will do her
household chores while caring her other sibling. Then at 10:00, she
will go to the market to buy foods to cook for their lunch. At
12:00 noon she will wait for her husband and her son to eat their
lunch. At afternoon, she will spend he time watching telenovelas
and take snap. At 6:00 pm she will cook food for their dinner and
eat at 7:00 pm. Then from 8:00 pm- 10:00 pm she will watch again
telenovelas then sleeps. C.Socioeconomic, Religion, Cultural
Beliefs and Practices
Mrs. Marie is a plain housewife taking care of her children. Her
husband, Mr. Mike, is the one who earns for their living he is a
truck driver and earns 6,000 pesos a month. Her affiliation in
religious views is Roman Catholic. According to her she visits the
church when she is not busy, even there is no mass. According to
her, she believes in pasma and usog. She seldom uses herbal
medicines. They usually take medicines when they feel ill such as
biogesic when with fever, robitusin when coughing.
2
III.History of Past and Present IllnessA.Obstetric History
Mrs. Maries first menarche arouse in the age of 12, she is first
year highschool student then. She has a 4 days regular menstrual
cycle. Her GP (TPALM) is G3P3 (T3P0A0L3M0) means she has had three
pregnancies and three deliveries at terms after 24 weeks of
gestation. Her last menstrual period was November 11, 2010.
According to her she had a monthly prenatal check up in their
Barangay Health Center. She is advised to take vitamins and Ferrous
sulfate. Her expected date of delivery is August 18, 2011. Age of
Gestation is 37 weeks and 3 days
B.History of Present Illness
Mrs. Marie is admitted last July 31, 2011 with a chief complaint
of unconscious, introital mass adherent to the placenta, vaginal
bleeding, pallor with an initial assessment of flabby abdomen and
tachycardia. According to her, she is still conscious when she
delivered her baby but when the midwife is delivering her placenta
she just felt dizzy. unti-unti dumilim yung paningin ko, hanggang
sa hindi ko na alam ang mga nang yari she added.
Admitting Diagnosis: G3p3(3003) via normal spontaneous delivery,
intrapartum hemorrhage, incomplete 3rd stage of labor, inverted
uterus, anemia secondary.
3
IV. Diagnostic ProcedureDiagnostic/ Laboratory Procedure
Hemoglobin Indication/ Purposes Signifies if the patient has
anemia. To help make decision whether patient needs blood
transfusion or not. Signifies the hydration of the RBCs and WBCs
Date July 31, 2011 Result 17g/L abnormal Normal Values 115g/L
Analysis and Interpretation Patient hemoglobin level is decrease.
It means patient may have anemia.
Hematocrit
July 31, 2011
.05g/L abnormal
White Blood Cells Lymphocytes
To check whether
July 31, 2011
8.1
patient has an infection . To check if patient has a viral
infection which functions in the immune system. To check if patient
clotting factors are normal. July 31, 2011 0.20
Platelet
70
Patient hematocrit level is decrease. Patient may suffer
dehydration and lack of nutrients in the cells. 3 5-10 x 10 /L
Patients WBC count is within the normal range means no infection.
0.20-0.35 Patients Lymphocytes level is within the normal range
means no viral Infection. 3 150-400 x 10 /L Patients platelet count
is low. Patient is at risk of prolonged clotting and
bleedingtime
0.40-0.52g/L
4
RBS
To check blood glucose level
8.35
3.85-9.0 mmoL/L
Patient RBS within normal range
BUN
Urea is cleared by the kidney and diseases which compromises the
function of the kidney will frequently lead to increased blood
levels The kidneys maintain the blood creatinine in a normal range
Creatinine has been found to be a fairly reliable indicator of
kidney function A breakdown product of purines that are part of
many foods.
1.9
1.7-8.3
Patient BUN Level is within normal range
Creatinine
58.6
58-100
Patient creatinine level is within normal range
Uric Acid
0.46
0.145-0.37
Uric Acid is elevated Patient is susceptible on having gout
LDH
To check if there are internal tissue damage
1.013
225-140 iu/L
Serum glutamic oxaloacetic transaminase (SGOT)
An enzyme that is normally present in liver and heart cells
levels are thus elevated with liver damage
54.4
10-40
Patient SGOT level is increase It may be indicative of liver
damage
Serum glutamic pyruvic transaminase
(SGPT) Sodium
SGPT is released into blood when the liver or heart are damaged.
A major electrolyte in the cell A water loving electrolyte To check
if patient is susceptible to hypertension To check if patient
susceptible to hypertention
27.3
0-39
Patient SGPT level is within normal range Patient has elevated
sodium level Patient may have hypertension Patient has low
Potassium level Effect of low potassium is muscle cramp and muscle
weakness Patient has increased chloride level May be indicative of
kidney problem
155.5
136-145 mmoL/L
Potassium
2.65
3.5-5.0 mmoL/L
chloride
Major electrolyte in the body To check is there proper cellular
nutrition in the body
116.7
101-111 mmoL/L
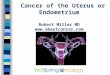
V. Anatomy and Physiology
The female reproductive system is designed to carry out several
functions. It produces the female egg cells necessary for
reproduction, called the ova or oocytes. The system is designed to
transport the ova to the site of fertilization. Conception, the
fertilization of an egg by a sperm, normally occurs in the
fallopian tubes. The next step for the fertilized egg is to implant
into the walls of the uterus, beginning the initial stages of
pregnancy. If fertilization and/or implantation do not take place,
the system is designed to menstruate (the monthly shedding of the
uterine lining). In addition, the female reproductive system
produces female sex hormones that maintain the reproductive cycle.
During menopause the female reproductive system gradually stops
making the female hormones necessary for the reproductive cycle to
work. When the body no longer produces these hormones a woman is
considered to be menopausal. The female reproductive anatomy
includes parts inside and outside the body. The function of the
external female reproductive structures (the genitals) is twofold:
To enable sperm to enter the body and to protect the internal
genital organs from infectious organisms. The main external
structures of the female reproductive system include:
Labia majora: The labia majora enclose and protect the other
external reproductive organs. Literally translated as "large lips,"
the labia majora are relatively large and fleshy, and are
comparable to the scrotum in males. The labia majora contain sweat
and oilsecreting glands. After puberty, the labia majora are
covered with hair. 7
Labia minora: Literally translated as "small lips," the labia
minora can be very small or up to 2 inches wide. They lie just
inside the labia majora, and surround the openings to the vagina
(the canal that joins the lower part of the uterus to the outside
of the body) and urethra (the tube that carries urine from the
bladder to the outside of the body). Bartholin's glands: These
glands are located beside the vaginal opening and produce a fluid
(mucus) secretion. Clitoris: The two labia minora meet at the
clitoris, a small, sensitive protrusion that is comparable to the
penis in males. The clitoris is covered by a fold of skin, called
the prepuce, which is similar to the foreskin at the end of the
penis. Like the penis, the clitoris is very sensitive to
stimulation and can become erect.
The internal reproductive organs in the female include:
Vagina: The vagina is a canal that joins the cervix (the lower
part of uterus) to the outside of the body. It also is known as the
birth canal. Uterus (womb): The uterus is a hollow, pear-shaped
organ that is the home to a developing fetus. The uterus is divided
into two parts: the cervix, which is the lower part that opens into
the vagina, and the main body of the uterus, called the corpus. The
corpus can easily expand to hold a developing baby. A channel
through the cervix allows sperm to enter and menstrual blood to
exit. Ovaries: The ovaries are small, oval-shaped glands that are
located on either side of the uterus. The ovaries produce eggs and
hormones. Fallopian tubes: These are narrow tubes that are attached
to the upper part of the uterus and serve as tunnels for the ova
(egg cells) to travel from the ovaries to the uterus. Conception,
the fertilization of an egg by a sperm, normally occurs in the
fallopian tubes. The fertilized egg then moves to the uterus, where
it implants into the lining of the uterine wall.
8
VI. PathophysiologyA.Definition It refers to the uterus turning
inside out with either birth of the fetus or delivery of the
placenta. The uterine fundus that has inverted and lies within the
endometrial cavity without extending beyond the external os is
called an incomplete inversion. Complete/ total inversion describes
an inverted fundus that extends beyond the external os. In our case
it is complete inversion. B. Predisposing and Precipitating Factors
The predisposing factor for our patient is an adherent placenta and
the precipitating factor is the Pulling of the Attached Placenta
Down, the placenta is reluctant to separate and is retained inside
the uterus, the midwife may try to remove it manually with hands
forcing the placenta down that has not easily separated, it can
bring the top of the uterus down with it.
C. Signs and Symptoms with rationale (patient centered)
Introital mass adherent to the placenta o Due to complete
inversion of the fundus that extends beyond external os. Vaginal
Bleeding o Because of incomplete placental separation and not
contracted uterus. Pallor o Because of excessive blood loss, the
body will supply first the important organs resulting to decreased
blood supply to the peripheral organs including the skin.
Unconscious o The blood supply in the brain cells decreased.
9
D.Schematic Diagram Predisposing factor: Adherent Placenta
Precipitating factor: Pulling of the Attached Placenta Down
Forcing the placenta down
Uterus will be pulled down ( where placenta is still
attached)
Introital mass adherent to the placenta
10
Open blood vessels large amount of Blood suddenly gushes Not
contracted uterus Decreased in circulating blood in the body
Vaginal bleeding compensatory mechanism tachycardia
Increased blood supply in important/main organs(brain,
kidneys,lungs,hear t) Blood loss continues decreased supply in the
brain dizziness
unconscio us
11
VII. Treatment and ManagementA. Surgical Intervention An
abdominal hysterectomy involves the removal of the uterus through a
long incision in the abdomen. The surgeon will either make a
vertical or horizontal incision in the abdomen, and the direction
of the incision is dependent upon the reason for the hysterectomy
and the size of the uterus. In the case of our patient vertical
incision is made.
During the surgery, the surgeon separates the uterus from the
vagina, ovaries, and fallopian tubes. The cervix is usually removed
along with the body of the uterus, which is called a total
hysterectomy that is done in our patient. If the cervix is not
removed as well, the procedure is called a partial hysterectomy,
after the uterus is removed; the layers of the abdominal tissue are
closed with stitches and staples. Intravenous Fluids Patient IV
fluid at right arm is D5LRS 1L regulated at 30 gtts /min infusing
well in the left arm started on august 2, 2011 at 7:00 in the
morning with side drip of D5W 500 ml with tramadol regulated at 12
gtts/min started. with D5W 500ml connected to a CVP line at 12
gtts/ min. At her left hand is 0.9% NACL I liter regulated at 12
gtts/min started on august 1, 2011 at 8:00 in the evening with side
drip of amino acid 5% sorbitol regulated at 12 gtts/min. Nursing
responsibilities: (prior/during/after)
check the patient's name before administration verify
physician's order indicating the type of solution, amt to be
administered, the rate of flow of solution, client allergies.
explain the procedure to the patient and/ or SO and wash hands.
explain the skin status at IV site, status of dressing and
consistency of IV flow rate with that ordered In administering and
starting line of the patient always start with identifying the
patient and explain the procedure to gain patient's trust. Count
drops per minute in the drip chamber, and adjusts the drip rate if
necessary. Ensure that the infusion rate and other controls on the
pump or the controller are correctly set and the pump or controller
is operating. Be sure to label the bottle with the following: date
started patient's name and number of IV bottle. After removing IV,
apply warm compress.
The patient had 16 bags of blood for transfusion.
12
C.Drug Study Name of The Drug & Stock Dose Dosage, Route,
Frequency of administratio n 200mg /cap BID( twice a day) Nursing
responsibilities
General action
Indication
Side effects
Generic : Ferrous Sulfate Brand : feosol Stock Dose :
200mg/cap
Anti-anemia
The patient hemoglobin is 17 g/L
Dark Stool Constipation Stomach upset
Generic name: 250 mg Electrolytes Hypokalemia GI discomfort
Warn patient that stool maybe dark If drug will be continue at
home, teach patient to: Do not take with antacids take with Vitamin
C rich food and fluid like calamansi juice. Increase fluid intake
Administer
Kalium Durulle Stock Dose: 250 mg/tab TID(thrice a day)
drug with food and full glass of water to decrease GI
discomfort. Teach patient to not break or chew the drug. Take it as
a whole.
Generic : Mefanamic Acid Brand : Ponstan Stock Dose : 500mg
500mg TID(three times a Day)
Analgesic
To relieve Pain -Pain due to surgical incision made
che ss
Heada Dizzine GI Pain
Teach patient take drug with food Provi de bed rest Take only
the prescribe dose Take the meds on time Do not administer oral
drugs
Generic name: Calcium Carbonate
1000mg TID(three times a day) Antacid, Electrolyte
Treatment of calcium deficiency
Nausea Vomiting constipation
Stock Dose: 1000mg
in tetany of the newborn Prevention of hypocalce mia during
exchange transfusion Improves weak or ineffective myocardial
contraction s when epinephrin e fails in cardiac resuscitatio n
abdominal pain dry mouth thirst
within 1-2 hours of antacid administrat ion Give calcium
carbonate antacid 1 and 3hr after meals and at bedtime Monitor
cardiac response closely during parenteral treatment with
calcium
C. DietDuring the time of the researchers visit last august 1
2011 the patient diet is on Nothing per Orem and at August 2,
2011is soft diet.
D.ActivityOn August 01, 2011 patient is advice to be flat on bed
for at least eight hours but patient may turn to sides every hour.
On August 02, 2011 the patient is advice to begin early and
frequently to start recovering with the surgery like doing her
personal hygiene and begin to sit and ambulate with assistance.
VIII. Nursing Care Plan
IX.Problems and Difficulties EncounteredI encountered many
difficulties in doing this case study, starting from caring the
patient in the hospital; she is my patient for 2 days, taking her
CVP line every hour at first day. Then at second day I checked her
5 IVF fluids, her vital signs, intake and output, again her CVP
line. Though that is the case, I learned a lot in taking care of
this patient, especially in measuring the CVP line. It is my first
time to see and measure such. I learned the technique in proper
measurement. I dont have problems encountered in making the
Demographic data of the patient, only in making the
Pathophysiology. I spent almost half of the day in doing it,
getting data in the net and books that will help me a lot, making
it step by step, knowing it will be the heart of our case study.
And also I have difficulty in compiling the whole case study
because I need to wait for my group mates first to send their part
and edit them. -Samson, Evangeline
The problems that I encountered was first in doing a drug study
because other drugs are difficult to find and a lot of effort and
patience is required in it and at the same time I dont even know
how to start and if I am doing the correct/right thing. The second
is the copying of some data that is needed for our case study
because some words in the chart are difficult to understand. The
third one is that the internet connection was having a technical
problem and it is difficult to send a data/ a finished part to our
leader because of the internet connection. Soriano, Mary Grace
The problems I have encountered in making our group case study
is in the process of disseminating the workloads. And the time
frame before the submission of the paper. Other members are in a
rush because their own case study is also coinciding with the group
case study. also maybe lack of resources. Some may find it hard to
do the work especially if there is lack of comput ,laptop, esp
internet shops for those who are staying at dormitories. The
possible solutions for the time frame may be time management, in
the dissemination of workload may be in the process of fishbowl
method wherein a member will pick up a paper ,inside it corresponds
the particular part that member will be doing. Also, in the case of
"resources", it is not enough that we have our online resources; we
should also browse in our books for possible ideas. some may find
it hard to do the work especially if there is
lack of computer, laptop, esp internet shops for those who are
staying at dormitories.
I have encounters problems while doing and copying our patients
chart for our case study like I cant understand some words in the
doctors order where in fact it is hard to read the writings of the
doctor. And one thing is the chart is not always in our hands thats
why there are some information that has not been collect. Pradilla,
Angelica E.
I have encountered problem especially while copying the chart of
our patient in this case study. Many words in the doctors order are
hard to read, many term that I cannot understand that I think that
the first time I have encountered such. I think one of the problem
also is having lack of the time, each of us have a very busy day
and I dont know how to spare some time doing this because of a lot
thing to do. -Sagcal, Ramil C. The problems I have encountered in
making our group case study is in the process of dissiminating the
workloads. and the time frame before the submission of the paper.
Other members are in a rush because their own case study is also
coinciding with the group case study. also maybe lack of resources.
Some may find it hard to do the work especially if there is lack of
computer,laptop,esp internet shops for those who are staying at
dormitories. The possible solutions for the time frame may be time
management, in the dissimination of workload may be in the process
of fishbowl method wherein a member will pick up a paper ,inside it
corresponds the particular part that member will be doing. Also, in
the case of "resources", it is not enough that we have our online
resources,we should also browse in our books for possible
ideas.some may find it hard to do the work especially if there is
lack of computer,laptop,esp internet shops for those who are
staying at dormitories. -Tayag,Patrisha Marie N.
XI.
Bibliography
Books:
Maternal and Child Health Nursing 5th ed. By Adele Pilliteri
2007 Lippincott Williams & Wilkins
Nurses Pocket Guide edition ed. Doenges, Moorhouse, Murr 207
Nursing drug guide ed. Amy M. Karch 2007 Lippincott
Websites:
http://www.innerbody.com/image/repfov.html
http://www.medscape.com/viewarticle/405770_3
http://www.mims.com.ph/Philippines/drug/info/Kalium/Kalium%20durule
http://www.babycenter.com.ph/pregnancy/complications/uterusabnormal/
http://www.medterms.com/script/main/art.asp?articlekey=9968