Embed Size (px)
Citation preview

INVASIVE HODGKIN’S DISEASE OF BRAIN Report of T w o N e w Cases and Review of American and
Eui-okean lit el-at1is.e wit 11 C linical-Pa t hologic Cowelations GERALD MARSHALL, MD,* UROS ROESSMANN, MD,’ A N D
STANLEY VAN DEN NOORT, MDS
A review of American and European literature on cases of Hodgkin’s disease invading brain is presented. T w o additional cases are reported. An unexpectedly high number of initial complaints are referable to the central nervous system. Common clinical features are lesions of nerve roots with pain and amyotrophy; there are multiple cranial nerve palsies and papilledema. T h e pattern of involvement consists of widespread meningeal lesions with subsequent invasion of brain substance. Histologic evidence of widespread meningeal involvement may occur without change i n the gross appearance.
HE ~ I R S ~ CASE OF INTRACRANIAL HODGKIN’S T diseaae was recorded by hlurchison (1869) in a 6-year-old girl.16 The tumor involved the dur‘i at the base of the brain but apparently did not invade brain substance itself. Nu- merous repoi ts of intracranial involvement followed, the great majority dealing with sec- ondny pressure changes from bone and men- ingeal tumor, or ischcmic changes due to blood vessel compression by tumor. A search of Ainerican and European literature yielded 12 ( d5es of well-documented secondary inva- sion of brain substance. We have excluded from consideration all reported cases of pri- mary Hodgkin’s disease of 1 he nervous system and other types of malignant lymphoma.10. 18, w 21 ’I hi5 iepoit concerns two additional cases and a review of the available literature.
CASE RliPORTS
Case 1, CVAH #A 16325. One month be- fore admission, this 41-year-old man noted
Fmrn the Institute of Pathology, University Hos- pitals of Cleveland, Western Reserve University, Cleve- land, Ohio.
* Resident in Pathology University Hospitals of Cleveland and Fellow of the American Cancer Society; ?Assistant Professor in Neuropatliology; $Assistant Pro- fessor in Neurology, Western Reserve University.
Address for repiints: G. Marshall, MD, Institute of Pathology, Western Reserve University, 2085 Adelbert Road, Cleveland, Ohio 4410ti.
Supported in part through a fellowship grant from the 4inerican Cancer Society.
The authors express their appreciation to Dr. G. Bogaty, who performed the autopsy for the first case report, and to Dr. W. A. Morningstar of the Cleveland VA Hospital, who provided access to autopsy reports and tissue specimens. They also wish to acknowledge the cooperation given by the Cleveland VA Hospital.
Received for publication February 13, 1968.
progressive back pain radiating into both legs. Weakness and numbness of right leg were followed by sagging of the right side of the face. Examination on October 29, 1962 showed infranuclear right facial weakness, paravertebral spasm, weak dorsiflexion of right foot, absent knee jerks and intact ankle jerks. Weakness soon affected both legs.
Routine laboratory studies were normal. Cerebrospinal fluid was yellow and con- tained 102 mononuclear and 115 polymor- phonuclear leukocytes/mm3. The protein content was 3.9 Gm/100 ml. Myelography showed a block at L-4. A long extradural tumor mass was removed from L-2 to L-4; the dura was opened and a large intradural tumor mass was also removed from C1 to L-5.
Postoperatively pain and strength slowly improved. Signs then included lethargy, con- fusion, vertical nystagmus, absent abduction of right eye, absent right facial movement and sensation, deafness on right, absent gag reflex, and immobility of right vocal cord. Roentgenograms of skull with special views of petrous bone and base were normal. A tumor dose of 3136 rads was given to base of skull in November 1962.
In the last month of life, fever, polymor- phonuclear leukocytosis (92%), and lym- phopenia (Zyo) appeared. Confluent infiltra- tion of right middle and left lower lobes was noted on chest roentgenograms. Cul- tures were negative and there was no im- provcment on antibiotics. T h e patient was found dead on anuary 21,1963.
spread Hodgkin’s disease involving all the internal lymph nodes, lungs, small bowel, kidneys and lumbar vertebrae. In addition there were bilateral recent pulmonary emboli
Autopsy fin d ings: Autopsy revealed wide-
62 1

and confluent bronchopneunioni~i. In gen- eral the tumor resembled tlie sarcomatous variety of Jackson and Parker (non-pleomor- phic reticular type of Lukes and Butler).7? 15 In several locations the granulomatous form predominated (mixed type of Lukes and Butler).
Inspection of the brain showed no abnor- mality of dura, venous sinuses, leptome- ninges, cerebral hemispheres or cerebellum. On coronal section a well-defined soft yel- low mass l cm in diameter was found dis- torting the floor of third ventricle between the ninmniillary bodies and cerebral pedun- cles.
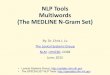
Hematoxylin and eosin, reticulum, silver impregnation and phloxine fast green stains were used in the histologic examination of tissues. Microscopically the tumor resembled that seen elsewhere in the body. Rinucleate Reed-Sternberg cell variants and cellular pleomorphism were prominent. Nost of the cells were mononuclear but there were numerous multilobate and binuclear forms with prominent nucleoli and bizarre mitotic figures. Occasional Iymphorytes, plasnia cells
and polymorphonuclear leukocytes were scattered throughout the tumor (Fig. 1). Small foci of necrosis were seen.
Peripherally, the neoplasm extended into the surrounding brain through tlie Virchow- Robin spaces. Reactive astrocytosis was prominent. T h e meninge3 at the base of the brain were diffusely involved with residual Hodgkin’s disease, which did not extend into brain tissue. Chromatolysis was present in tlie facial, spinal trigeminal, and lateral vestibular nuclei on the right side.
Spinal subarachnoid tumor had produced atrophy of lumbar plexus and degeneration of tractus gracilis. Special stains did not show abnormal or increased amounts of reticulum in the tumor.
Case 2, CVAH #023877. This 51-year-old welder noted a swollen mass in his neck in September 1962. Chest roentgenogram showed mediastinal enlargement. Node bi- opsy was consistent with Hodpkin’s disease. He received local radiation and was next seen in Octoher 1964 with left cervical and axillary adenopathy which responded to
FIG. 1. Case 1. Photomicrograph of tumor invading brain in floor of third vcntricle (H and E, x125).

KO. 3 INVASIVE HODGKIN’S DISEASE OF BRAIN * Mnrshall et a / . 623
vinbl astine and cyclophosphamide. A month later left pleural effusion was treated with intrapleural nitrogen mustard. In January 1965 a left hemiparesis slowly evolved and he received two courses of vinblastine with- out effect. Four months later, low back pain radiating into both legs and associated with progressive weakness and weight loss led to hospi talii-ation.
Findings included low grade fever, mas- sive left cervical adenopathy, moderate hep- atomegaly and multiple raised reddened lesions of shin. T h e patient was confused, inattentive and showed perseverative motor responses. There was a left Horner’s syn- drome and mild left facial weakness. Horse- ness, dysphagia and poor movement of left palate were noted. Left arm and both legs were weak and wasted. There was diffuse para tonic rigidity. Tendon jerks were de- preswd. The left plantar response was ex- tensor; the right, silent. Pin and proprio- ceptive sensation were reduced in left arm and both legs.
Hematacrit was 30%) and leukocyte count ~ f00 /mm3 with 48q0 lymphocytes. BUN was 39 mg/100 ml; electrolytes, normal: serum albumin, 3.4 Gm/100 ml. Lumbar puncture on May 18, 1965 produced yellow clear acellular fluid containing 288 mg/100 ml piotein and 41 mg//100 ml sugar. Myelo- gram was normal. The pineal gland was in the midline. Skin biopsy revealed infiltration by large lymphoma cells. Fever, lethargy and conlluent left pulmonary infiltrates with pleural effusion preceded his death in June 1965.
Alifopsy findings: Death resulted from bilateral pneumonia and terminal aspira- tion. Hodgkin’s disease was found in the cervical, supraclavicular, axillary, mediasti- nal, inesenteric and periaortic lymph nodes; in the lungs and peripancreatic fat; stalk of the pituitary gland and thyroid. The tumor was predominantly of the sarcomatous retic- ular form of Lukes and Butler.16
Inspection and sectioning of the brain again showed no abnormality of the dura, venous sinuses, leptomeninges, cerebral hemispheres or cerebellum.
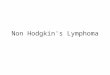
Hematoxylin and eosin, phloxine fast green, reticulin and silver impregnation stains were used in the histologic examina- tion of tissue. Microscopically, Hodgkin’s disease diffusely involved the meninges, espe- cially over the cerebellum. Extending from the meninges were small nodular and occa- sionally confluent tumor infiltrates, which widely permeated through the molecular and granular layers of the cerebellum into the underlying white matter (Fig. 2). Loss
of Purkinje cells and secondary degenera- tion were evident only in areas involved by tumor. Similar foci of invasion were found in the molecular layer of the cerebral cortex (Fig. 3) and superficial layer of the pons. In all areas the tumor appeared partially inhibited by the pia mater and spread pri- marily through the Virchow-Robin spaces. Reticulum fibers were not abnormally lo- cated or increased in amounts. Hodgkin’s disease infiltrates also involved the stalk of the pituitary gland as well as large portions of the cervical and lumbosacral plexi. There was secondary degeneration in the posterior columns.
Cytologically the tumor was composed of large pleomorphic Reed-Sternberg cells with frequent lobation, bizarre configurations, hyperchromatism and giant nucleoli. In ad- dition there were atypical mononuclear cells, occasional neutrophils, plasma cells, fibro- blasts and rare lymphocytes. Eosinophils and necrosis were absent (Fig. 4).
DISCUSSION The clinical and pathologic features of
previously reported cases and the two cases just described are summarized in Table 1.
Clinical Aspects Review of the data indicated an average
age of 41 years (range 27-61) and a slight predominance of men (7/12). Duration of illness ranged from 2 months to 7 years with an average of 2 years. It is of interest that eight of the 14 cases presented with symptoms referable to the central nervous system and in four (including our case 1) there was no concurrent evidence of involvement in any other system. Prominent clinical features are listed in Table 2. Multisegmental pain and weakness of arms and legs due to multiple root or plexus involvement were particularly common. Frequent findings were muscle wasting, absent reflexes and involvement of multiple contiguous cranial nerves. Delirium, stupor and seizures may have reflected met- abolic disorders of visceral origin as well as direct invasion of brain by tumor.
Anemia, leukocytosis and/or moderate lymphocytosis were found in ten of 14 pa- tients. Positive radiologic findings appeared at some time during the course of the disease in all cases. Chest roentgenogmm was abnor- mal in nine cases. On two occasions myelog- raphy demonstrated spinal cord compression by tumor. Cerebrospinal fluid findings are summarized in Table 3.

624 CANCER September 1968 Vol. 22
The diagnosis of Hodgkin’s disease was made by lymph node biopsy in five cases and not until autopsy in four cases.
Other Systemic Involvement There was palpable or roentgenographic
evidence of lymphadenopathy in 11 of 14 cases. Skeletal tumor occurred in 10 patients, while lung and bowel invasion were noted in seven cases each. Hodgkin’s disease of the spleen was present in six cases. Infiltrates in
FIG. 2 (upper). Case 2 . Photomicrograph demonstrating marked invasion of cerebellum by tumor extending through cortex into granular layer (H and E, X25).
FIG. 3 (lower). Case 2. Photomicrograph of cerebral cortex show- ing method of tumor spread along Virchow- Robin spaces (H and E, x37.5).
decreasing frequency were described in the liver, gall bladder, pancreas, genitourinary tract and thyroid. Diabetes insipidus in three cases ~ 7 a s associated with tumor involvement of the sella turcica.
Gross Findings in the Brain Virtually all parts of tlie brain were in-
volved in metastatic Hodgkin’s disease. There is no reported case of this tumor within tlie substance of spinal cord. As ex-

No. 3 INVASIVE HODGKIN’S DISEASE OF BKAIN - AIarshnll e t nl. 625
FIG. 4. Case 2. Pho- tomicrograph of cere- bellum showing sev- eral prominent Reed- +ternberg cells (H and E, X ~ W ) .
pectcd, multiple lesions were present in eight of the 14 cases; single tumor inasses were de- scribed in four, while gross lesions were not observed in two. The last mentioned points out the need for careful microscopic evalu- ation in all suspected cases.
Gross apprxarance of the tumors varied con- sider ably from definite circumscribed masses to irregular diffuse and confluent lesions. Fre- quent association of discoloration, edema and focal hemorrhage was noted. In many instances, thickened meninges heralded un- derlying tumor. Most of the infiltrates had a hard consistency. In three cases the lesions werc soft, unlike other metastatic tumors.
Microscopic Appearance Both granulomatous and sarcomatous
types of Hodgkin’s disease (Jackson and Parker) were found within brain substance. This is in contrast to the previously stated opinion that the granulomatous variety in- volves only the meninges, while the sarcoma- tous form may invade brain substance.3 Reed- Sternberg cells o r their variants were found in a l l cases. T h e other usual cellular com- ponents of Hodgkin’s disease, namely, large histiocytes, eosinophils, polymorphonuclear leukocytes, lymphocytes and fibroblasts, var- ied in their frequency. Nevertheless, none of the cases leave any doubt about the basic nature of the tumor 011 microscopic examina- tion.
Necrosis of tumor and surrounding tissue
was frequent. Central chrornatolysis was found in cranial nerve nuclei in cases com- plicated by nerve compression. Glial reaction was prominent in well-demarcated tumors and was scant in diffusely spreading infil- trates. In almost all of the cases the dura and arachnoid were thickened and fibrotic.
In two cases degeneration of the posterior columns resulted from root compression by meningeal tumor.
Pathogenesis and Clinico-Pathologic Correla- tion
Since a large number (8) of the reported cases (14) first presented with symptoms re- ferable to the central nervous system, the tu- mor within brain substance cannot be as- cribed to prolonged survival and failure of drugs to penetrate brain as has been impli- cated in leukemias. Because of frequent cra- nial nerve involvement, the presence of papil- ledema in four cases may reflect invasion of the optic nerve sheath by tumor, rather than a generalized increase in intracranial pres- sure. However, a tumor mass or interference with spinal fluid circulation clearly produced elevated intracranial pressure in some cases.
In general, the clinical features resemble those seen in other forms of diffuse menin- geal neoplasia (reticulum cell sarcoma, car- cinomatous meningitis) and require careful distinction from primary or complicating sec- ondary processes of infectious origin (tuber- culosis, cryptococcosis).

TA
BL
E 1.
Su
mm
ariz
ed C
ase
Rep
orts
of
Hod
gkin
's D
isea
se i
n B
rain
Sub
stan
ce
31
-r
c
h
Aut
opsy
fi
ndin
gs
Bra
in
Aut
hor
Age
L
engt
h C
linic
al
Syst
emic
N
o.
Sea
r Se
x di
seas
e ob
serv
atio
ns
CN
S s
igns
L
ab f
indi
ngs
invo
lvem
ent
Gro
ss
Mic
ro
Com
plic
atio
ns
1 A
skan
azyl
1
92
1
2 H
ecke
r an
d Fi
sche
rzs
1922
3 Se
rebr
jani
klg
1933
4 Lo
uis-
Bar
14
1947
5 K
ing
and
Ric
hai d
soii'
19
50
6 V
indi
gnia
19
53
59
F
32
M
41
M
27
M
30
F 45
M
Lym
ph n
odee
nlar
ge-
Nec
k pa
in f
ollo
wed
by
X-r
ay:
5th
cerv
ical
H
D b
ilate
ral
in c
ervi
- D
iffu
se ch
ange
in
CO
T-
Peri
vasc
ular
cu
ffin
g C
ord
com
pres
- m
ent
with
po
sitiv
e w
eakn
ess
in b
oth
arm
s ve
rteb
ra c
olla
pse
cal
node
s,
vert
ebra
l te
x at
bas
e of
bra
in
of
smal
l co
rtic
al
yes-
si
on
biop
sy
colu
mn
nerv
e ro
ots
sels
in d
irec
t ext
ensi
on
from
dur
al t
umor
an
d du
ra
En
larg
ed
axil
lary
T
hree
da
ys
prem
or-
36 To
lym
phoc
ytes
in
Dif
fuse
Hod
gkin
's i
n-
Bila
tera
l mul
tipl
esof
t-
Mul
tifo
cal
accu
mul
a-
Non
e ly
mph
no
des,
liv
er
tem
ha
d re
peti
tive
pe
riph
eral
blo
od
volv
emen
t of
lym
ph
enin
gs in
the
cen
trum
ti
ons
of pl
eocy
tic t
u-
and
sple
en;
asci
tes;
se
izur
es a
fter
par
acen
- no
des.
m
edia
stin
um.
sem
iova
le
near
th
e m
or,
incl
udin
g R
-S
posi
tive
lym
ph n
ode
tesi
s of
4.5
1 ri
bs,
liver
, sp
leen
, ca
udat
e ce
lls,
plas
ma
cells
. bi
opsy
m
esen
tery
, pa
ncre
as
lym
phob
last
sand
lym
- an
d lu
ng
phoc
ytes
. Nec
rosi
s and
pe
riva
scul
ar c
uffi
ng
z w
eakn
ess,
bila
tera
l V
I sp
inal
flu
id;
prot
ein
bow
el a
nd r
nese
nter
ic
of br
ain
stem
. B
ilat-
w
ith
man
y R-S ce
lls.
n
m
era1
dif
fuse
dis
colo
ra-
lym
phoc
ytes
and
gian
t 75
Abd
omin
al
tum
or
Lef
t pto
skri
ghtf
acia
l 36
0 ly
mph
ocyt
es i
n T
umor
in
st
omac
h,
Tum
or
in
men
inge
s D
iffu
se t
umor
sp
read
N
one
and
head
ache
ne
rve
pals
y, w
eakn
ess
and
pres
sure
ele
vate
d ly
mph
nod
es
an
d
nu
mb
nes
s of
tio
n of
whi
te m
atte
r ce
lls, p
erip
hera
l gl
iosi
s.
sign
s. L
ater
dev
elop
ed
and
tegm
entu
m
of fi
ng
delir
ium
po
ns
limbs
wit
h m
enin
geal
of
cent
rum
sem
iova
le
and
peri
vasc
ular
cuf
- 2 % 3 u-
L
ow b
ack
pain
, di
f-
Rem
itti
ngpa
rapa
resi
s L
euko
cyto
sis
and
15
Tu
mo
r in
sp
leen
. T
umor
in
pi
tuit
ary,
Pr
edom
inat
ely
peri
- D
iab
etes
in
- rn
't
fuse
ly
mp
ha
de
- fo
llow
ed
by
prog
res-
ce
lls i
n sp
inal
fl
uid
lym
phno
desa
nd l
ungs
R
. m
amm
illar
y bo
dy,
vasc
ular
sp
read
of
sipi
dus
(0
nopa
tliy
liepa
tosp
le-
sive
in
volv
emen
t of
w
ith e
leva
ted
prot
ein
floo
r of
thir
d ve
ntri
cle
typi
cal
infi
ltrat
es c
on-
nom
egal
p.
anor
exia
, cr
ania
l ne
rves
11
1 an
d ba
sal
gang
lia
tain
ing
R-S
cel
ls. a
nd
m
a,
vom
iting
and
hea
d-
thro
ugh
XII
. U
lti-
lym
phoc
ytes
ac
he
mat
ely
deve
lope
d m
y-
oclo
nus
follo
wed
by
co
nfus
ion
and
com
a
I
Swel
ling
righ
t si
de o
f N
ysta
gmus
, de
afne
ss
Slig
ht
leuk
ocyt
osis
. G
ener
aliz
ed l
ymph
ad-
Sin
gle
har
d
tum
or
Ty
pic
al H
odgk
in's
T
uber
culo
us
neck
and
diz
zine
ss
on l
eft,
righ
t pt
osis
. no
CSF
repo
rt.
Skul
l en
opat
hy a
nd s
plen
o-
mas
s in
lef
t cer
ebel
lo-
tum
or
wit
h ce
ntra
l m
enin
gitis
an
d im
pair
ed f
unct
ion
x-ra
ys n
orm
al
meg
aly
pont
ine
angl
e d
egen
erat
ion
. In
- vo
lved
cra
nial
ner
ves
of r
ight
Vth
and
VII
th
and
inva
ded
unde
r-
cran
ial
nerv
es.
Lat
er.
deve
lope
d pa
pill
e-
lyin
g ce
rebe
llum
alo
ng
dem
a. w
eakn
ess
of le
ft
smal
l ve
ssel
s pa
late
and
com
a
App
rox.
W
eakn
ess,
m
alai
se,
Rig
ht
hem
ipar
esis
In
crea
sed
prot
ein
in
Hod
gkin
's g
ranu
lom
a N
o du
ral i
nvol
vem
ent.
Hod
gkin
's t
umor
wit
h N
one
of
lung
s Si
iiglt:
m
ass
in
L.
R-S
cells
, pl
asm
a 3
mo
anor
exia
. na
usea
, w
ith in
crea
sing
stu
por
CSF
rig
ht
ches
t p
ain
. oc
cipi
topa
riet
al w
hite
ce
lls,
gian
t ce
lls.
lyrn
- e
head
ache
, di
zzin
ess,
an
d em
esis
or
rbag
ic f
oci
mat
ter,
wit
hsof
t hem
- ph
ocyt
es a
nd n
eutr
o-
0
wsi
g
E
phils
. Pr
omin
ent
ne-

7 \V
epIe
r*s
1053
8 Fe
in a
nd N
ewill
6 19
54
9 L
asce
lles
and
Rur
ston
'l 19
62
10
Lit
vak,
Led
er
and
Kou
var'?
19
64
11
Lju
ngda
hl.
Str
ang
and
Toui
'3 19
65
12
Kau
fman
s 19
65
33
11 y
r F 34
A
ppro
x.
M
7 yr
36
App
rox.
F
7
mo
56
App
rox.
M
8
mo
29
5 yr
. an
d F
st
ill a
live
a
t tim
e of
re
port
61
7
mo
M
Rig
ht s
ided
E
vide
nce
of i
ncre
ased
In
crea
sed
prot
ein
in
Dif
fuse
HD
in
lym
ph
Ja
clis
onia
n se
iiur
es
intr
acra
nial
pr
essu
re
CSF
no
des,
sp
leen
, liv
er.
and
righ
t V1
nerv
e G
I. G
U s
yste
ms.
and
pa
iij-
L rr
r&ra
i co
iuni
ri
Lym
phad
enop
athy
, Se
izur
es a
nd
papi
lle-
Nor
mal
CS
F
Gen
eral
ized
lym
phad
- w
eakn
ess a
nd w
eigh
t de
ma
follo
wed
by
en
opat
hy w
ith
Hod
g-
loss
tr
ansi
ent l
eft a
nd fi
xed
kin'
s in
volv
emen
t of
ri
ght h
emip
ares
is.
Lef
t pt
osis
. T
erm
inal
stu
por
liver
and
bon
e
Hea
dach
e, d
ysar
thri
a Pa
pill
edem
a, d
eafn
ess
No
CS
F e
xam
inat
ion
Hod
gkin
's d
isea
se i
n an
d dy
spha
gia
A. S
. and
pal
sy o
f le
ft
SII
fol
low
ed b
y a
s-
cend
ing
affe
ctio
n of
cr
ania
l ne
rves
; te
r-
min
al p
olyd
ipsi
a an
d po
lyur
ia
lung
s
Low
gra
de f
ever
and
Pe
rson
alit
y ch
ange
. Sp
inal
flui
d su
gar
=
Lym
phad
enop
athy
w
eigh
t lo
ss
papi
lled
ema
wit
h pr
o-
19 m
g/10
0 m
l an
d an
d sp
leno
meg
aly
gres
sive
bli
ndne
ss
prot
ein
= 8
5 m
g, 1
00
ml
Lym
phad
enop
athy
N
umbn
ess,
pa
in a
nd
wea
knes
s in
lef
t ar
m;
late
r, p
apil
lede
ma a
nd
dipl
opia
and
head
ache
Wea
knes
s,
wei
ght
Con
fusi
on,
para
pare
- lo
ss a
nd f
atig
abil
ity
sis.
po
lydi
psia
an
d po
lyur
ia f
ollo
wed
by
pr
ogre
ssiv
e co
nfus
ion.
bi
late
rial
pto
sis.
an
d m
utte
ring
spe
ech
CS
F n
ot r
ecor
ded
HD
in l
eft
hila
r ce
rvi-
ca
l lym
ph n
odes
. Lat
er
deve
lope
d ab
dom
inal
m
ass
CS
F p
rote
in w
as35
8 L
ym
ph
aden
op
ath
y
mg/
100
ml
falli
ng t
o w
ith
HD
in
volv
ing
73 m
g/10
0 m
l. 3
whi
te
stom
ach,
jeju
num
and
ce
lls a
lso
pres
ent
gall
blad
der
Dif
fuse
m
en i n
gca
I th
ick
enin
g.
sing
le
mas
s in
rig
ht p
rece
n-
rrai
gyr
us
Fir
m
sing
le
mas
s a
t th
e m
edia
n su
rfac
e of
th
e le
ft
hem
isph
ere
ante
rior
ly, c
onti
guou
s w
ith
over
lyin
g tu
mor
in
dur
a an
d ca
lvar
ium
D
iffu
se
invo
lvem
ent
Diff
use
peri
vasc
ular
in
filt
rati
on
in
th
e m
enin
ges
wit
h sp
read
in
to
the
brai
n st
em
and
mai
n tu
mor
mas
s.
Tum
or
com
pose
d of
ly
mph
ocyt
es,
plas
ma
cell
s, n
eutr
op
hil
s.
eosi
noph
ils
Tum
or
desc
ribe
d as
ty
pica
l of
H
odgk
in's
gr
anul
oma
Tu
mo
r tv
oic
al
of
._
or
dur
a in
left
mid
dle
Hod
gkin
's d
isea
se i
n-
and
post
erio
r fo
ssae
vo
lvin
g m
enin
ges
and
wit
h di
rect
ext
ensi
on
exte
ndin
g in
to
brai
n in
to th
e pi
tuit
ary.
lef
t su
bsta
nce
and
cran
ial
tem
pora
l lo
be,
pons
ne
rves
an
d fl
oor o
f th
ird
ven-
tr
icle
T
hick
enin
g of
me-
D
escr
ibed
as
typi
cal
ning
es,
opti
c ne
rves
H
odgk
in's
dis
ease
an
d ch
iasm
; m
ulti
ple
area
s of
hem
orrh
age
and
di
scol
orat
ion;
so
ften
ing i
n L
. fro
ntal
, oc
cipi
tal,
and
R.
tem
- po
ral
lobe
s w
ith
dis-
cr
ete
tum
or
in
L.
par
ieta
l lo
be
an
d
hypo
thal
amus
O
n su
rgic
al e
xam
ina-
T
ypic
al
R-S
ce
lls,
tion
a s
ingl
e, g
rayi
sh-
plas
ma
cells
. ly
mph
o-
yello
w f
irm m
ass
was
cy
tes.
fib
robl
asts
and
en
ucle
ated
fr
om
the
eosi
noph
ils.
T
um
or
post
erio
r par
ieta
l lob
e.
also
in
su
bara
chno
id
Men
inge
s re
port
ed a
s sp
ace
not
invo
lved
G
ross
ly n
orm
al
Dif
fuse
in
volv
emen
t of
bo
th
hem
isph
eres
a
nd
c
ere
be
llu
m
thro
ugh
peri
vasc
ular
in
vasi
on o
f H
odgk
in's
tu
mor
wit
h R
-S c
ells
an
d re
ticu
lum
ce
lls.
Als
o in
vasi
on o
f po
s-
teri
or
root
s of
th
e sp
inal
cor
d
Son
e
Non
e
Dia
bete
s in
sipi
dus
Non
e
Non
e to
dat
e
Dia
bete
s in
sipi
dus

n
rc T
AB
LE
1.
( Con
tinlie
d)
m
Aut
hor
Age
L
engt
h C
linic
al
No.
Y
ear
Sex
di
seas
e ob
serv
atio
ns
CN
S s
igns
Sy
stem
ic
Lah
fin
ding
s in
volv
emen
t
13
Mar
shal
l,
11
Roe
ssm
ann.
M
an
d va
n de
n N
oort
(1)
14
Mar
shal
l,
51
Roe
ssm
ann
ILI
and
van
den
Noo
rt
(2)
3 rn
o
3 yr
Low
bdc
k pa
in r
adi-
at
ing
into
bot
h le
gs
Ly
mp
had
eno
pat
hy
in
nec
k pr
ogre
ssin
g to
ge
nera
lized
form
wit
b he
pato
meg
aly
and
skin
les
ions
Num
bnes
s an
d w
eak-
ne
ss i
n R
. le
g an
d R
. fa
ce.
Prog
ress
ive
in-
volv
emen
t of
R
. cr
a-
nial
ner
ves
and
both
le
gs.
Ter
min
al
leth
- ar
gy a
nd c
onfu
sion
L.
hem
ipar
esis
, co
n-
fusi
on,
L.
Hor
ner's
. bi
late
ral
leg
wea
knes
s
3.9
Grn
/lOO
ml
pro-
te
in,
102
mon
ocyt
es
and
115
poly
s in
sp
inal
flu
id
Ace
llula
r sp
inal
flu
id
wit
h 28
8 m
g/10
0 m
l pr
otei
n an
d 41
mg/
10
0 ni
l gl
ucos
e
Aut
opsy
fin
ding
s
L y
m p
h a
d e n
o p
a t h
y
and
tum
or
in l
ungs
, sm
all
bow
el,
kidn
eys
and
lum
bar
vert
ebra
e
Gen
eral
ized
lym
phad
- en
opat
hy a
nd t
umor
in
lun
gs a
nd t
hyro
id
Bra
in
Gro
ss
Mic
ro
Com
plic
atio
ns
Sing
le
soft
ye
llow
fo
cus
in t
he f
loor
of
the
thir
d ve
ntri
cle
No
gros
s ch
ange
R-S
cel
ls a
nd c
ellu
lar
Non
e pl
eom
orph
ism
in
th
e tu
mor
. M
enin
geal
in-
vo
lvem
ent
alon
g th
e br
ain
stem
. C
hrom
a-
toly
sis
in s
ever
al c
ra-
nial
ne
rve
nucl
ei
on
righ
t. D
egen
erat
ion
in
trac
tus
grac
illis
Dif
fuse
in
volv
emen
t N
one
of th
e m
enin
ges
wit
h F
spac
es, m
ost e
xten
sive
5;i 3 2
brai
n in
vasi
on
alon
g 2:
th
c V
irch
ow-R
obin
n
in c
ereb
ellu
m,
also
in
the
pitu
itar
y st
alk.
T
ypic
al H
odgk
in's
in-
3 in
filt
rate
s w
ith
R-S
ce
lls.
Deg
ener
atio
n of
Q-
the
trac
tus
grac
illis
an
d bo
th l
umba
r an
d br
achi
al p
lexu
ses
cb
't -

No. 3 INVASIVE HODGKIN’S DISEASE OF BRAIN - I\.larshalZ et al. 629 ,. I ABLE 2. Clinical Findings in 14 Cases __-____
Delirium or confusion 8 Crani a1 polyneiiropathy 7 Papilledema 6 Cauda equina or lumbosacral plexus signs 5 Cervical roots or brachial plexus signs 5 Hemiparesis 4 Seizures 4 Diabetes insipidus 3
TABLE 3 . Cerebrospinal Fluid in Eight Cases*
Normal 1 Increased pressure 1 Low sugar 2 Pleocytosis 3 Increased protein 7 * All of the cases had incomplete CSF reports.
By far the most common route of invasion was that of direct extension into brain sub- stance by overlying meningeal tumor through the Virchow-Robin spaces. The ef- fectiveness of the arachnoid membranes in limitin? the extent of tumor was remarkable. Man) cases of meningeal invasion by Hodg- kin’s disease were reported in which the bar- rier was not broken; and although the tumor was found in the Virchow-Robin spaces, it did not invade brain substance itself.
Eleven of the 14 cases in Table I show a consistent pattern clinically and pathologi- cally and indicate a widespread meningeal invasion by tumor resulting in nerve root conipres\ion, invasive spread into brain sub- stance, and multifocal or focal growth of meningeal tumor masses which may compress adjacent brain or spinal cord. In only three reported cases was there evidence of direct parent h) matous Hodgkin’s disease in brain substance without clear meningeal connec- tion. A critical ieview of these cases does not provide adequate proof of parenchymatous metastn5is without eviclent e of contiguous spread.
Hecker (in 1922) described symmetrical invabion arid softening of centrum semiovale in a patient whose clinical evidence of neu- rologic involvement came with the onset of repetitive seizures following a 4.2 liter para- centesis 3 days before death. The role played by ischemic anoxia must be considered but the microscopic description does suggest the presence of lymphoma. Such changes may represent perivascular spread from anterior perforate substance or Sylvian fissure ad- mixed with ischemic infarction. The clinical and pathologic description of Vindigni’s case does not permit detailed analysis. I t is not clear that microscopic study of dura or arach- noid was made or that sections other than those relating directly to the tumor were ex- amined. The third case was a surgical speci- men in which no careful search for menin- geal origin was possible.
COMMENTS Since Murchison’s original case, identify-
ing Hodgkin’s disease within the cranial cav- ity, there have been numerous publications citing clinical and pathologic manifestations of Hodgkin’s disease in the central nervous system. Close examination of these publica- tions indicates that many of the reported cases describe only secondary changes, such as pressure from adjacent dural or meningeal tumor nodules, or vascular ischemic changes in the brain and spinal cord from blood ves- sel impingement by tumor outside the nerv- ous tissue. Other authors have reported on cases that may represent Hodgkin’s disease in brain, but these cases lack microscopic or au- topsy proven evidence.zt4.6,17,22,23,27
From the 14 cases reviewed in this paper, several significant and interesting observa- tions have been made.
T h e frequency with which these cases of Hodgkin’s disease first presented with com- plaints referable to the central nervous sys- rem has not previously been recognized.
Hodgkin’s disease within brain substance cannot be ascribed to prolonged survival and failure of drugs to penetrate the brain, since in several cases nervous system involvement preceded any treatment.
The diffuse ineningitic presentation of in- tracranial Hodgkin’s disease clinically re- quires the careful distinction from primary or complicating infectious meningeal disease.
In almost all cases widespread meningeal tumor led to affection of nerve roots, the de- velopment of meningeal tumor masses, with resultant compression of surrounding brain or spinal cord, and frank invasion of adjacent brain. A preponderance of evidence indicates that brain tissue invasion is accomplished through perivascular spaces as extensions from overlying meningeal tumor. None of the cases demonstrated Hodgkin’s disease within spinal cord tissue.
Microscopic investigation of the brain demonstrated Hodgkin’s disease in two cases in which there was no evidence of gross ab- normality.

ti30 CANCER September 1968
REFERENCES
VOl. 22
1. Askanazy, M.: Lymphogranuloni dcs Knochen- marks. Verh. Deutsch. Ges. Path. 18:78-83, 1921.
2. Berkman, J.. Netsky, M. G., and Zimmermaii, H. hl.: Malignant lymphomas within the central ner- vous system. J . ATetiropatlt. E x p . A’eutol. 1O:lOO-102, 1951.
3. Denny-Brown, D., and Foley, J. M.: Clinical pathologic conference. Neurology (Minneap.) 3:615- 620, 1953.
4. Favre. M.. aud Croizat, P.: Caracthres g6nCraus d u granulome malin, tires de son Ctude anatomo-clinique. Ann. Anat. Path. (Paris) 8:838-914, 1931.
5. Fcin, S. B., and Newill, V. A.: Cerebral Hodgkin’s disease-Case report of Hodgkin’s gmnuloma with cerebral invasion. A m . J. Med. 17:291-294, 1954.
6. __ , and Parker, F., Jr.: Hodgkin’s disease- V. Involvement of certain other organs. New Eng. J. Aled. 233:369-376, 1945.
7. Jackson, H.. Jr., and Parker, F., Jr.: Hodgkin’s Disease. In Nelson Loose-Leaf Living Medicine, vol. 111. W. W. I’almcr. cd. New York, Thomas Nelson and
8. Kaufinati, G.: Hodgkin’s discase involving the central nervous system. Arch. A‘eurol. (Chicago) 13:
9. King, D. P., and Richardson, J. S.: Hodgkin’s dis- ease of the cerebellum. S t . Thomas Hosfi. Rep. 6273- 277, 1950.
10. Kinnev. T. D.. and Adams. R. D.: Reticulum
Sons, 1946; pp. 347-360.
555-558, 1965.
cell sarcomi of the blain. Aich. Xeziiol. Pyychiat. 50: 552-564, 1943.
11. Lascelles, R. G., and Burston, J.: Hodgkin’s dis- ease-Disease presenting with symptoms of cranial nerve involvement. Arch. Neurol. (Chicago) 7:359-364, 1962.
12. Iitvak, J., Leder, M. M., and Kauvar, A. J.: Case reports-Hodgkin’s disease involving optic nerve and brain. J. Neurostirg. 21:798-801, 1964.
13. Ljungdahl, I., Strang, R. R., and Tovi, D.: In- tracerebral Hodgkin’s granuloma-Report of a case and review of the literature. Netirochirzirgia (Stutt- gart) 8:113-118, 1965.
14. I.ouis-Bar, D.: Sur les manifestations cCrCbrales de la lymphogranulomatose maligne ct le probleme de I’encCphalite lytnphogranulomateuse. J. Belg. Neurol. Psych jut. 47:703-728, 1947.
15. Lukes, R. J., and Butler, J. J.: T h e pathology and riomeuclature of Hodgkin’s disease. Cancer Res.
16. hfurcliison, C.: Case of “lymphadcnoma” of the lymphatic system, spleen, liver, lungs, heart, dia- phragm, dura matcr, etc. Trmrs. Path. Soc. London 21:372-389, 1870.
17. Schiipe, hl.: Zur Frage “Blastom”-“Encepllalitis.” Arch. Psychiat. Nemenkr. 109:755-784, 1939.
18. Schricker, J. L., Jr., and Smith, D. E.: Primary intracerebral Hodgkin’s disease. Cancer 8:629-633, 1955.
19. Serebrjanik, B.: Lymphogranulomatose Meningo- encephalitis und Polyradiculitis. Dtsch. Z . Neruenheilk.
20. Sparling, H. J., Jr., and Adanis, R . D.: Primary Hodgkin’s sarcoma of the brain. Arch. Path. (Chicago)
21. Sparling, H. J., Jr., Adams, R. D., and Parker, F., Jr.: Involvement of the nervous system by malig- nant lymphoma. Medicine 26:285-332, 1947.
22. Urechia, C. I., and Goia, I.: Contribution 5 I’6tutlc de la lymphogranulomatose tle la moelle. Presse AJed. 35:179-181, 1927.
23. Viets, H. R., and Hunter, F. T.: Lymphoblas- totnatous involvement of the nervous system. Arch. A‘ezirol. Psychiat. 29: 1246-1262, 1933.
24. Vindigni, E.: Sul linfogranuloma localizzato- Duplice focolaio polmonare e cerebrale. Policlinico (iVJed.) 60:123-140, 1953.
25. \’on Hecker, H., and Fischer, W.: Zur Kenntnis der Lymphogranulomatose. Dtsch. bled. Wschr. 48:
26. Wepler, W.: Uher Lymphogranulomatose Me- ningoencephalitis. Virch07u Arch. Path. Anat. 323:49- 59, 1953.
27. Ziegler, K.: Die Hodgkinsche Krankheit (Mono-
26: 1063-1081, 196G.
129:103-130, 1933.
42:338-344, 1946.
482-484, 1922.
graphie). ,Jena, G. Fischvr, 191 1 .
ADDENDUM ’ro REFERENCES
1. Conybeare, E. T.: Some features of Hodgkin’s dis- ease. Guy Hosp. Rep. 83:53-62, 1933.
2. Cooper, M. J.: Lymphogranulomatosis maligna (Hodgkin’s disease)-With invasion of the spinal canal and paraplegia. JAMA 102:917-921, 1934.
3. Diiring, M.: Zur Pathologie und Klinik des Lyni- phogranuloms. Dtsch. Arch. Klin. Med. 127:76-109, 1918.
4. Ginsburg, S.: Hodgkin’s disease-With predomi- nant localization in the nervous system; early diag- nosis and radiotherapy. Arch. Intern. Med. (Chicago) 39571 -595, 1927.
5. Gray, R. C., Baker, A. B., Cottrell, L., and Skog- land, J. E.: Hodgkin’s disease of the central nervous system. Int. Clin. 4230-236 (new series), 1941.
6. John, H . T., and Nabarro, J . 1). N.: Intracranial manifcstaiions of malignaut lymphoma. Brit. J . Cancer
7. Johnsson, V.: NPgra fall av lymfogranulomatos med nervsymtom. Hygiea 93:39-54, 1931.
8. Martin, H. E., and Courville, C. B.: Hodgkin’s disease with involvement of the cranial dnra mater. Bull. Los Angeles Netirol. S O C . 1:145-148, 1936.
9~386-400, 1955.
9. Rizzi, I.: II granuloma rnaligno del sistema ner- voso. Riv. Nezcrol. 11:377-402, 1938.
10. Russell, D. S. , and Rubinstein, L. J.: Pathology of tumours of the nervous system, 2nd ed. London, Edward Arnold Ltd., 1963.
11. Saalfeld, U.: Zur frage der Hautlokalisationen der Lymphogranulomatose. Arch. Dernmt. Syph . 148: 158-165, 1925.
12. Shapiro, P. F.: Changes of the spinal cord in Hodgkin’s disease-Report of two cases, with an un- usual skin manifestation in one. Arch. Neurol. Psych iat.
13. Sternberg, C.: Die Lymphogranulomatose. Klin.
14. Vogel, P. J., and Richland, K. J.: Involvement of the central nervous system by Hodgkin’s disease- Case report with five year interval between primary spinal and cerebral lesions. Bull, Los Angeles Neicrol.
15. \’on Hagen, K . 0.: Lymphogranuloma (Hodg- kin’s disease) with involwment of the spinal cord. Zbid. 2:20-25, 1937.
24 509-524, 1930.
Wbch~ . 4:529-531, 1925.
SOC. 20:83-86, 1955.