Embed Size (px)
Citation preview

LABORATORY INVESTIGATIONJ Neurosurg Spine 28:10–22, 2018
Direct laryngoscopy and endotracheal intubation in patients who have unstable cervical spines is po-tentially hazardous, carrying an undefined risk of
cervical spinal cord injury. Mechanistically, in the pres-ence of an unstable cervical spine, the forces of direct la-ryngoscopy are thought to cause pathologic cervical spine motion, potentially resulting in cord injury via excessive
cord stretch and/or direct cord compression. Although airway management recommendations exist for patients with known or suspected cervical spine instability,2,9, 40,48 the evidence supporting these recommendations is weak. Current recommendations are based on 1) case reports19,26,
36, 44, 52, 53,56,73 and observational case series29 of patients with unstable cervical spines, 2) cervical spine motion studies
ABBREVIATIONS FE = finite element; MD = mean difference; Oc = occiput.SUBMITTED February 11, 2017. ACCEPTED May 12, 2017.INCLUDE WHEN CITING Published online October 20, 2017; DOI: 10.3171/2017.5.SPINE17189.
Intubation biomechanics: validation of a finite element model of cervical spine motion during endotracheal intubation in intact and injured conditionsBenjamin C. Gadomski, PhD,1 Snehal S. Shetye, PhD,1 Bradley J. Hindman, MD,2 Franklin Dexter, MD, PhD,2 Brandon G. Santoni, PhD,3 Michael M. Todd, MD,4 Vincent C. Traynelis, MD,5 Robert P. From, DO,2 Ricardo B. Fontes, MD, PhD,5 and Christian M. Puttlitz, PhD1
1Department of Mechanical Engineering, School of Biomedical Engineering, Orthopaedic Bioengineering Research Laboratory, Colorado State University, Fort Collins, Colorado; 2Department of Anesthesia, University of Iowa Roy J. and Lucille A. Carver College of Medicine, Iowa City, Iowa; 3Foundation for Orthopaedic Research and Education, Tampa, Florida; 4Department of Anesthesia, University of Minnesota, Minneapolis, Minnesota; and 5Department of Neurosurgery, Rush University Medical Center, Chicago, Illinois
OBJECTIVE Because of limitations inherent to cadaver models of endotracheal intubation, the authors’ group devel-oped a finite element (FE) model of the human cervical spine and spinal cord. Their aims were to 1) compare FE model predictions of intervertebral motion during intubation with intervertebral motion measured in patients with intact cervical spines and in cadavers with spine injuries at C-2 and C3–4 and 2) estimate spinal cord strains during intubation under these conditions.METHODS The FE model was designed to replicate the properties of an intact (stable) spine in patients, C-2 injury (Type II odontoid fracture), and a severe C3–4 distractive-flexion injury from prior cadaver studies. The authors recorded the laryngoscope force values from 2 different laryngoscopes (Macintosh, high intubation force; Airtraq, low intubation force) used during the patient and cadaver intubation studies. FE-modeled motion was compared with experimentally measured motion, and corresponding cord strain values were calculated.RESULTS FE model predictions of intact intervertebral motions were comparable to motions measured in patients and in cadavers at occiput–C2. In intact subaxial segments, the FE model more closely predicted patient intervertebral mo-tions than did cadavers. With C-2 injury, FE-predicted motions did not differ from cadaver measurements. With C3–4 injury, however, the FE model predicted greater motions than were measured in cadavers. FE model cord strains during intubation were greater for the Macintosh laryngoscope than the Airtraq laryngoscope but were comparable among the 3 conditions (intact, C-2 injury, and C3–4 injury).CONCLUSIONS The FE model is comparable to patients and cadaver models in estimating occiput–C2 motion during intubation in both intact and injured conditions. The FE model may be superior to cadavers in predicting motions of sub-axial segments in intact and injured conditions.https://thejns.org/doi/abs/10.3171/2017.5.SPINE17189KEY WORDS biomechanics; cervical spinal cord; cervical spine; endotracheal intubation; finite element model
J Neurosurg Spine Volume 28 • January 201810 ©AANS 2018, except where prohibited by US copyright law
Unauthenticated | Downloaded 05/24/22 01:36 PM UTC

Finite element model of cervical spine and spinal cord
J Neurosurg Spine Volume 28 • January 2018 11
during intubation in patients with stable spines, and 3) in-tubation studies in cadavers in which various forms of cer-vical spine injury were surgically created.1,12,13,24,33,34, 41, 54,
67,69 Findings from these sources cannot be reliably applied to the airway management of patients with unstable spines because 1) case reports comprise fewer than 10 patients, and causative links between intubation and cord injury are often uncertain;29,42 2) motion of a stable cervical seg-ment during intubation does not predict the motion of an unstable segment;31,33,34,57 and 3) during intubation, motion of the cadaveric cervical spinal segments does not always replicate motion observed in living patients.27,28 With re-gard to this last point, we recently identified multiple fac-tors that limit the clinical applicability of cadaver intuba-tion studies, chief among them advanced cadaver age and in vitro tissue preconditioning.27,28 Specifically, because of age-related cervical spine degenerative changes and at-tendant decreases in range of motion,47,50, 55, 62, 66,75 authors of cadaver intubation studies report less motion during intubation than that observed in younger patient popula-tions, especially in subaxial (C2–5) segments.27,28 In ad-dition, in cadavers, repeated laryngoscope force applica-tion changes the force/motion properties (biomechanics) of airway and spinal tissue,27,28 the consequence of in vitro tissue preconditioning.37,71 With the multiple intubations in cadavers, intubation biomechanics can change so much that primary cervical spine motion findings may not be directly applicable to clinical care.27,28 Accordingly, there is a need for a noncadaveric model to predict the motion of unstable cervical segments during endotracheal intu-bation. To address this need, our group developed a 3D finite element (FE) model of the human cervical spine and cervical spinal cord. Inclusion of the cord allows for esti-mates of cord strain during intubation. Cord strain is more likely to be a primary determinant of cord injury than spi-nal (bony) motion per se.6,39,59
This study had 2 aims. The first aim was to compare FE model predictions of cervical spine motion during in-tubation to motion experimentally measured in patients with intact (stable) spines30 and in cadavers with 2 types of surgically created cervical spine injuries.27,28 The sec-ond aim was to model cervical spinal cord strain occur-ring during intubation in the presence of an intact cervical spine and in the presence of the 2 cervical spine injuries. As in our prior studies, we used 2 laryngoscopes known to differ greatly in the amount of force applied during intu-bation, specifically, a conventional high-force line-of-sight laryngoscope (Macintosh) and a low-force indirect video laryngoscope (Airtraq).
MethodsFinite Element Model
The FE model of the complete cervical spine (occiput [Oc]–C7) was developed using CT data and material properties (Table 1).8,18, 45, 46, 58, 64, 68, 70,74 Previously published mechanical behavior data of the vertebra’s cortical shell,68 posterior elements,14 bony endplates,70 and facet cartilage46 were used. Additional details regarding the FE model of the cervical spine are provided in the Appendix.
The cervical spinal cord was modeled using human
cross-sectional geometry data at the various cervical spine levels obtained from published data.35 In addition, the ana-tomical connections between the spinal dura mater and the tissues surrounding the spinal canal were included to replicate the stability boundary conditions of the cord.10 Additional details regarding the FE model of the cervical spinal cord are provided in the Appendix.
Due to the inherent variation in the main input param-eters of the FE model among patients, specifically, varia-tions in the geometry of the structure being modeled and the material performance used to define its behavior, an-thropometric means are used to create the FE model. Be-cause of this, we consider FE model predictions accurate to the first decimal place (see Statistical Analysis).
Modeling Methods for All Intubation SimulationsIn our FE model simulations, we entered laryngoscope
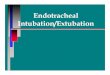
force values that were measured using 2 different force-sensing laryngoscopes (high force, Macintosh; low force, Airtraq) obtained in our prior clinical30 and cadaver27,28 studies. We did so to test FE model predictions under dif-ferent loading conditions. As shown in Fig. 1, to simulate intubation force in the FE model, we applied force as a point source. For Macintosh intubations, force was applied to the midpoint of the anterior surface of the C-3 vertebral body directed at 70° from the coronal plane. For Airtraq intubations, force was applied to the midpoint of the ante-rior surface of the C-2 vertebral body (~11 mm cephalad to the Macintosh force point) directed at 90° from the coro-nal plane. These force locations and vectors were based on 1) a review of radiographic images from our prior clinical study,30 showing the position of the laryngoscopes relative to the cervical spine at the point of maximum laryngo-scope force application; and 2) simultaneous laryngoscope force distribution measurements that showed that the cen-ter point of force application was 11 mm more cephalad with the Airtraq than with the Macintosh laryngoscope. In all simulations, the occiput was allowed to rotate in place and translate inferiorly and superiorly as necessitated by the model simulation, while the inferior surface of the C-7 vertebral body was kinematically constrained to prevent movement.
To replicate variable loading conditions (i.e., varia-tion in laryngoscope force), a range of force values was entered into the FE model using values measured ex-perimentally in our prior clinical and cadaver studies; see Cervical Spine Motion Data From Prior Studies. In all simulations, force was applied incrementally using mini-mum and maximum increments of 1 × 10-7% and 1% of the total force, respectively, depending on the complexity of the simulation until converging on the maximum as-signed force value (100%).
In all simulations, calculations were made for both inter-vertebral motion of the bony spine in the sagittal plane and peak values of spinal cord strain. Strain quantitates tissue deformation (e.g., change in length or width) in response to an applied stress (force/area = pressure) as a percentage of the starting value of the parameter. Compression results in negative strain values, whereas stretch results in positive strain values. Additional details regarding calculation of cord strains are provided in the Appendix.
Unauthenticated | Downloaded 05/24/22 01:36 PM UTC

B. C. Gadomski et al.
J Neurosurg Spine Volume 28 • January 201812
Modeling Methods for Injured Spine SimulationsThe FE C-2 injury model was designed to replicate the
injury that was surgically created in our earlier cadaver C-2 injury study (a Type II odontoid fracture).28 Specifi-cally, in the FE C-2 injury model, complete disassociation of the odontoid from the C-2 vertebral body was achieved without disruption of the transverse ligament by removing 2 layers of elements in the horizontal plane and creating finite sliding contact surfaces such that fracture fragments could translate with respect to each other during loading but not penetrate each other’s surface (i.e., occupy the same volume).
The FE C3–4 injury model was designed to replicate C3–4 injury, a severe distractive-flexion injury, that had been surgically created in our prior cadaver C3–4 injury study.27 Specifically, the mechanical properties of the su-praspinous, interspinous, and posterior longitudinal liga-ments; ligamentum flavum; and facet articular capsule were greatly decreased so that they did not restrict motion at the C3–4 level. In addition, the properties of the annulus fibrosis and nucleus pulposus were decreased by 90% so that the disc did not substantially contribute to resisting the forces of intubation. In both the FE and cadaver C3–4 injury models, the anterior longitudinal ligament was in-tact and the facet joints were in anatomical position.
In injured spine simulations, intervertebral translation in the anteroposterior plane (subluxation) was calculated. To be consistent with our prior cadaver C-2 injury study, in the corresponding FE model, we calculated the change in canal space at C1–2 during intubation. To be consistent with our prior C3–4 injury study in cadavers, in the corre-sponding FE model, a negative value for subluxation was assigned when the inferior (C-4) vertebral segment trans-lated posteriorly in relation to the superior (C-3) vertebral segment.
Cervical Spine Motion Data From Prior StudiesIntact Cervical Spine
In the FE model, we entered individual laryngoscope force data measured in our prior study conducted in pa-tients (n = 14) with intact (stable) cervical spines.30 In that study, patients were intubated twice in random order us-
ing a force-sensing Macintosh laryngoscope and force-sensing indirect Airtraq video laryngoscope. Simultane-ous measurements of laryngoscope force application and sagittal plane cervical spine motion in the sagittal plane were obtained throughout intubation. In each patient, a maximum value for laryngoscope force application and simultaneous intervertebral rotation (flexion/extension) at each cervical interspace was measured.30
Injured Cervical SpineIn FE modeling studies, we entered the individual la-
ryngoscope force data measured in 2 earler cadaver in-tubation studies conducted with cervical spine injuries at C-2 (Type II odontoid fracture, n = 12)28 and C3–4 (severe distractive-flexion injury, n = 14).27 In both of these studies, cadavers with surgically injured cervical segments were intubated twice in random order using force-sensing Mac-intosh and Airtraq laryngoscopes utilizing the same meth-ods and personnel from the clinical study. In both of these cadaver studies, motion of the injured segment in the sagit-tal plane was analyzed for intervertebral rotation (flexion/extension) and anteroposterior motion (subluxation).
In the cadaver C-2 injury study, experimentally mea-sured motion of the injured segment (primary data) was mathematically corrected (“force corrected”) to account for decreased (subclinical) intubation forces that occurred with repeated intubations.28 This use of force correction was based on the assumption of a linear relationship be-tween laryngoscope force and spinal motion. In the FE modeling studies, the same individual force-corrected ca-daver laryngoscope force values were used to create a sec-ond set of loading conditions and resulting force-corrected FE modeled spine motions.
In contrast, in the cadaver C3–4 injury study, although subclinical intubation forces were (again) measured us-ing both laryngoscopes, force-corrected motions were not calculated.27 In the FE modeling studies, Macintosh and Airtraq intubation forces measured in patients with stable spines30 were used to create a second, more clinically re-alistic, set of loading conditions and FE model predictions for spine motion in the presence of the modeled C3–4 in-jury.
TABLE 1. Summary of mechanical properties used in the FE model
Material Elastic Modulus (MPa) Poisson Ratio (υ) Authors & Year
Cortical bone 11,000.00 0.30 Ueno & Liu, 1987Trabecular bone* Crawford et al., 2003Articular cartilage† Noailly et al., 2005Bony endplates 1,000.00 0.30 Whyne et al., 2001Ligaments‡ Yoganandan et al., 2001 & Rohlmann et al., 2006Spinal cord§ Sparrey & Keaveny, 2009Nucleus pulposus 1.50 0.49 Fagan et al., 2002 & Natarajan et al., 2004Annulus fibrosus 5.00 0.40
* Spatially varying orthotropic material coefficients based on CT data.† Marlow initial bulk modulus = 1.80 MPa; initial υ = 0.40.‡ Exponential force-displacement data.§ Ogden μp = 0.45, αp = 4.70.
Unauthenticated | Downloaded 05/24/22 01:36 PM UTC

Finite element model of cervical spine and spinal cord
J Neurosurg Spine Volume 28 • January 2018 13
Statistical AnalysisOriginal experimental data from our prior clinical30
and cadaver27,28 studies were used. All values for laryngo-scope intubation forces, cervical spine motion, and spi-nal cord strains were rounded to a single decimal prior to analysis (see Finite Element Model above). This was done so that data from all sources (patients, cadavers, and FE model) were compared and reported with an equal degree of precision. In a few instances, rounding result-ed in small changes in reported means, standard devia-
tions, and/or p values from prior published values. In no instance did rounding change any conclusions made in prior studies. Continuous variables are reported as mean ± SD.
Nonpaired comparisons between groups (patients vs FE model; FE model vs cadavers) of intervertebral ex-tension and subluxation were made using Welch’s t-test (i.e., 2 groups with normal distributions but with unequal variances) and the 95% confidence intervals for the dif-ferences in the group mean values are reported. Groups
FIG. 1. Anterior (coronal, A), lateral (sagittal, B), and axial (C) views of the Oc–C7 cervical spine finite element model. Only the caudal portion of the occiput is shown. The spinal cord can be most easily visualized in the axial view. D: For Macintosh intuba-tions, the intubation force vector (FINT) originated from the midpoint of the anterior face of the C-3 vertebral body at an angle of 70° from the coronal plane and consisted of anterior and inferior vector components. E: For Airtraq intubations, the intubation force vector originated from the anterior face of the C-2 vertebral body (11 mm cephalad to the Macintosh force point) at an angle 90° from the coronal plane. The inferior surface of the C-7 vertebral body was fixed in all directions. The occiput was allowed to rotate around the sagittal (X) axis for all simulations and translate in the axial (Z) direction.
Unauthenticated | Downloaded 05/24/22 01:36 PM UTC

B. C. Gadomski et al.
J Neurosurg Spine Volume 28 • January 201814
were also compared using the Wilcoxon-Mann-Whitney test as a sensitivity analysis. All p values are 2-sided and exact. Bonferroni corrections were made for multiple comparisons to the same group; corrected p values and 95% confidence intervals are designated as “corrected.” FE model predictions for spinal cord strains were com-pared pairwise between laryngoscopes using both the Student 1-group t-test and the Wilcoxon signed-rank test. All calculations were performed using StatXact-11 (Cytel Software).
ResultsCervical Spine Motion: Intact Spine
Patient, FE model, and cadaver values for maximum in-tervertebral cervical spine motion (extension) during Mac-
intosh and Airtraq intubations in the presence of an intact (stable) spine are shown graphically in Fig. 2 and sum-marized in Table 2. With both laryngoscopes, the laryn-goscope total forces were comparable among the 3 groups. At Oc–C2, there were no significant extension differences between groups (patients vs FE model and FE model vs cadavers) with either laryngoscope. In contrast, at C2–5 with the Macintosh laryngoscope, there may have been borderline extension differences between groups: patients versus FE model (mean difference [MD] 4.3° [corrected 95% CI -0.3° to 8.9°]; corrected p = 0.069); FE model versus cadavers (mean difference 3.3° [corrected 95% CI -0.0° to 6.6°]; corrected p = 0.053). At C2–5 with the Airtraq laryngoscope, there were no significant extension differences between groups, although the same pattern in
FIG. 2. Macintosh (upper) and Airtraq (lower) values for segmental intervertebral extension in patients, FE model, and cadav-ers. Values are mean ± SD. Each group comprises 14 subjects. With each laryngoscope, total force is comparable among the 3 groups.
Unauthenticated | Downloaded 05/24/22 01:36 PM UTC

Finite element model of cervical spine and spinal cord
J Neurosurg Spine Volume 28 • January 2018 15
the group mean extension values was apparent (patients > FE model; FE model > cadavers).
Cervical Spine Motion: Injured C-2 (Type II Odontoid Fracture)Preinjury Control Values
As shown in Table 2, average C1–2 extension values in the preinjury baseline state (intact spine, normal intuba-tion forces) were comparable among patients, the FE mod-el, and cadavers: Macintosh (8.1° ± 4.7°, 7.6° ± 0.2°, and 6.8° ± 5.5°, respectively); Airtraq (5.5° ± 4.8°, 5.5° ± 0.2°, and 4.8° ± 3.8°, respectively).
Primary ResultsThe FE model predicted that during intubation in the
presence of a Type II odontoid fracture, 1) C-1 subluxes posterior to C-2; 2) C-1 carried the free odontoid process posteriorly; and 3) the posterior movement of the odontoid process resulted in a decrease in canal space at the C-1 and C-2 interspace. FE model and cadaver experimental values for C1–2 extension and C1–2 canal space change during Macintosh and Airtraq intubations in the presence of a Type II odontoid fracture are summarized in Table 3. Using the primary (experimentally measured) force and motion results, there were no differences between the FE model and cadavers in C1–2 extension or change in C1–2
canal space with either laryngoscope, although marginally less change in the C1–2 canal space (~1.2 mm) was pre-dicted by the FE model for the Airtraq (p = 0.045).
Force-Corrected ResultsIn our cadaver C-2 injury study, forces applied by Mac-
intosh and Airtraq laryngoscopes during intubations in the presence of C-2 injury were 20%–50% less than clini-cally normal forces, the result of tissue preconditioning from earlier intubations.28 Accordingly, in our previous study, primary experimental C1–2 motion results were force corrected to estimate motion that would occur with the application of clinically normal intubation forces. Our previous force corrected method assumed a linear rela-tionship between laryngoscope force and motion and was expected to overestimate motion.28 Force-corrected val-ues for injured C1–2 motion in the FE model and cadavers are shown in Table 3. There are no significant differences between the FE model and cadavers in force-corrected C1–2 extension or subluxation with either laryngoscope, although marginally less change in the canal space (~2.7 mm) was predicted by the FE model for the Airtraq laryngosocpe (p = 0.077). As expected, the magnitudes of the force corrections were less in the FE model than those obtained by linear force correction of primary cadaver data, although absolute differences between the force-
TABLE 2. Segmental intervertebral motion during endotracheal intubation in patients, FE model, and cadavers with intact cervical spines
LaryngoscopeTotal Force,
NIntervertebral Segment, Degrees of Extension
Oc–C1 C1–2 C2–3 C3–4 C4–5 Oc–C2* C2–5*
Macintosh Patients (n = 14)† 48.8 ± 15.8 11.4 ± 6.5 8.1 ± 4.7 2.5 ± 3.0 5.1 ± 3.8 2.5 ± 3.5 19.5 ± 10.3 10.0 ± 6.8 FE model (n = 14) 48.8 ± 15.8 12.2 ± 0.1 7.6 ± 0.2 3.5 ± 0.7 1.8 ± 0.6 0.5 ± 0.0 19.8 ± 0.1 5.7 ± 1.3 Cadavers (n = 14)‡ 46.5 ± 14.2 15.2 ± 6.0 6.8 ± 5.5 1.5 ± 2.5 2.1 ± 3.3 −1.2 ± 3.0 22.0 ± 10.0 2.4 ± 4.9 Patients vs FE model MD (corrected 95% CI) −0.2 (−7.2 to 7.0) 4.3 (−0.3 to 8.9) Corrected p values 0.99, 0.99 0.069, 0.033 FE model vs cadavers MD (corrected 95% CI) −2.2 (−9.0 to 4.6) 3.3 (−0.0 to 6.6) Corrected p values 0.84, 0.43 0.053, 0.058Airtraq Patients (n = 14)† 10.4 ± 2.8 9.6 ± 4.5 5.5 ± 4.8 1.8 ± 3.6 2.0 ± 3.3 0.2 ± 2.6 15.1 ± 7.4 4.0 ± 5.6 FE model (n = 14) 10.4 ± 2.8 8.9 ± 0.1 5.5 ± 0.2 1.1 ± 0.1 0.2 ± 0.0 0.5 ± 0.0 14.4 ± 0.2 1.9 ± 0.1 Cadavers (n = 14)‡ 12.9 ± 9.6 9.1 ± 3.8 4.8 ± 3.8 0.3 ± 1.4 −0.7 ± 2.8 −0.9 ± 4.6 13.8 ± 4.8 −1.2 ± 5.2 Patients vs FE model MD (corrected 95% CI) 0.8 (−4.2 to 5.7) 2.1 (−1.7 to 6.0) Corrected p values 0.99, 0.99 0.36, 0.99 FE model vs cadavers MD (corrected 95% CI) 0.5 (−2.7 to 3.8) 3.1 (−0.4 to 6.6) Corrected p values 0.99, 0.23 0.089, 0.113
Values are mean ± SD unless indicated otherwise. Extension is represented by positive values and flexion by negative values.* The 95% CIs for MD were calculated using Welch’s t-test (i.e., with unequal variances). The p values are presented as Welch’s test, Wilcoxon-Mann-Whitney test. The p values and 95% CIs are Bonferroni corrected for the 2 comparisons with the same FE model data for each of the 2 combined segments (Oc–C2 and C2–5).† All patient data are from Hindman et al., 2014.‡ All cadaver data are from Hindman et al., 2015, Intubation Set 1 (intubations 1 and 2), preinjury (baseline).
Unauthenticated | Downloaded 05/24/22 01:36 PM UTC

B. C. Gadomski et al.
J Neurosurg Spine Volume 28 • January 201816
corrected FE model and force-corrected cadaver values remained small.
Cervical Spine Motion: Injured C3–4 (severe distractive-flexion injury)Preinjury Control Values
In our cadaver C3–4 injury study, C3–4 extension dur-ing Macintosh intubations in the preinjury baseline state (intact spine, normal intubation force) was less than that measured previously in patients (0.3° ± 3.0° vs 5.1° ± 3.8°, respectively; Wilcoxon-Mann-Whitney, p = 0.0016).27 The FE model prediction for C3–4 extension under compa-rable conditions (1.8° ± 0.6°; Table 2) was also less than that measured in patients (Wilcoxon-Mann-Whitney, p = 0.0012).
Primary ResultsThe FE model predicts that, during intubation in the
presence of a severe C3–4 injury, C-4 subluxes posterior to C-3, the result of which is a decrease in canal space at the C-3 and C-4 interspace. FE model and cadaver val-ues for C3–4 extension and subluxation during Macintosh and Airtraq intubations in the presence of a severe C3–4 distractive-flexion injury are summarized in Table 4. With the Macintosh laryngoscope, C3–4 extension was approx-imately 8-fold greater in the FE model than in cadavers: 3.3° ± 1.1° vs 0.4° ± 2.7° (MD 2.9° [95% CI 1.3°–4.6°], p = 0.0017). With the Macintosh laryngoscope, C3–4 sub-luxation was approximately 3-fold greater in the FE model than in cadavers: -0.9 ± 0.1 vs -0.3 ± 0.6 mm (MD -0.6 mm [95% CI -0.9 to -0.2 mm], p = 0.0024). With the Airtraq laryngoscope, C3–4 extension values did not dif-fer between the FE model and cadavers, but subluxation was greater in the FE model than in cadavers: -0.6 ± 0.2
mm vs 0.0 ± 0.7 mm (MD -0.6 mm [95% CI -0.1 to -1.0 mm], p = 0.015).
Force-Corrected ResultsIn our cadaver C3–4 injury study, the amount of force
applied by both laryngoscopes in the presence of C3–4 injury was less than clinically normal values, especially for the Airtraq laryngoscope.27 Lesser force application likely results in an underestimate of motion. Thus, normal (clinical average) force values for the Macintosh (48.8 ± 15.8 N) and Airtraq (10.4 ± 2.8 N) laryngoscopes from our prior clinical study30 were used in the C3–4 injury FE model; the results are summarized in Table 4. In the FE model, force-corrected results do not substantively differ from primary results, with extension and subluxation val-ues that are clinically small.
Cervical Spinal Cord StrainIn all FE strain models, a range of clinically normal
intubation force values was entered using values from our patient study (14 patients) (Macintosh, 48.8 ± 15.8 N; and Airtraq, 10.4 ± 2.8 N).30 Table 5 summarizes FE model predictions for peak minimum principal strain (compres-sion) and peak maximum principal strain (stretch) dur-ing intubations with the intact (stable) spine, C-2 injury (Type II odontoid fracture), and C3–4 distractive-flexion injury. In all 3 conditions, peak minimum principal strain (compression) was present in the posterior region of the spinal cord approximately at the level of the C-3 vertebral body (Fig. 3). In all 3 conditions, peak spinal cord strains (both compression and stretch) were 2- to 20-fold greater with the Macintosh than with the Airtraq laryngoscope. In all 3 conditions, the mean peak minimum principal (compressive) strain values did not exceed -20%, which is
TABLE 3. FE model and cadaver values for C1–2 extension and canal space change during Macintosh and Airtraq intubations in the presence of a Type II odontoid fracture
Laryngoscope
Type II Odontoid FracturePrimary Results Force-Corrected Results
Total Force, N
C1–2 Extension, degrees*
Change in C1–2 Canal Space, mm*
Total Force, N
C1–2 Extension, degrees*
Change in C1–2 Canal Space, mm*
Macintosh FE model (n = 12) 35.2 ± 12.3 6.5 ± 0.9 −1.1 ± 0.6 45.6 ± 12.7 7.3 ± 0.8 −1.6 ± 0.7 Cadavers (n = 12)† 35.2 ± 12.3 7.3 ± 4.2 −1.0 ± 1.4 45.6 ± 12.7 9.9 ± 6.3 −1.1 ± 1.7 FE model vs cadavers MD (95% CI) −0.8 (−3.6 to 1.9) −0.1 (−1.0 to 0.9) −2.6 (−6.6 to 1.4) −0.5 (−1.7 to 0.6) p values 0.52, 0.66 0.87, 0.79 0.18, 0.99 0.29, 0.24Airtraq FE model (n = 11) 6.0 ± 4.0 1.6 ± 0.6 −0.1 ± 0.1 14.4 ± 10.2 2.5 ± 0.9 −0.4 ± 0.6 Cadavers (n = 11)† 6.0 ± 4.0 2.3 ± 3.3 −1.3 ± 1.7 14.4 ± 10.2 4.2 ± 7.8 −3.1 ± 4.5 FE model vs cadavers MD (95% CI) −0.7 (−3.0 to 1.5) 1.2 (0.0 to 2.3) −1.7 (−7.0 to 3.5) 2.7 (−0.4 to 5.8) p values 0.48, 0.81 0.045, 0.002 0.48, 0.60 0.077, 0.007
Values are mean ± SD unless indicated otherwise. Extension is represented by positive values and flexion by negative values.* The 95% CIs for MD were calculated using Welch’s t-test (i.e., with unequal variances). The p values are presented as Welch’s test, Wilcoxon-Mann-Whitney test.† All cadaver data from Hindman et al., 2015, Table 4 (primary results) and Table 5 (force-corrected results).
Unauthenticated | Downloaded 05/24/22 01:36 PM UTC

Finite element model of cervical spine and spinal cord
J Neurosurg Spine Volume 28 • January 2018 17
the approximate threshold for compression-mediated cord injury.6,38 In all 3 conditions, the mean peak maximum principal strain (stretch) did not exceed 10%, which is the approximate threshold for stretch injury.3,39,59
DiscussionBased on these findings, we suggest that our FE model
is a tool that will advance understanding of the behavior of the intact and injured cervical spine and spinal cord. At present, the focus of our FE model is endotracheal intuba-tion in the presence of cervical spine injury. However, with inclusion of additional features (see Current Model Limi-tations and Model Adaptability), FE models can likely ad-dress a wide range of questions regarding the pathogenesis
of injury and management of patients with diverse cervical spine pathologies.
Modeling Spinal Cord StrainsAlthough quantifying spine motion during intubation
is of interest, it cannot answer the critical question of how much motion is too much motion. Thus, a fundamental advantage of an FE model over cadavers is its ability to predict mechanical parameters that are difficult to experi-mentally quantify, specifically spinal cord strain. This is important because cord strain is the mechanistic basis of cord injury rather than spinal (bony) motion per se.6,39,59
Although the FE model shows that the cervical spinal cord experiences strain during routine intubation (both
TABLE 4. FE model and cadaver values for C3–4 extension and subluxation during Macintosh and Airtraq intubations in the presence of a severe C3–4 distractive-flexion injury
Laryngoscope
Severe C3–4 Distractive-Flexion InjuryPrimary Results Force-Corrected Results
Total Force, N
C3–4 Extension, degrees*
C3–4 Subluxation, mm*
Total Force, N
C3–4 Extension, degrees
C3–4 Subluxation, mm
Macintosh FE model (n = 14) 41.3 ± 21.4 3.3 ± 1.1 −0.9 ± 0.1 48.8 ± 15.8 3.7 ± 0.8 −1.0 ± 0.1 Cadavers (n = 14)† 41.3 ± 21.4 0.4 ± 2.7 −0.3 ± 0.6 FE model vs cadavers MD (95% CI) 2.9 (−1.3 to 4.6) −0.6 (−0.9 to −0.2) p values 0.0017, 0.0010 0.0024, 0.0036Airtraq FE model (n = 14) 5.5 ± 4.6 1.3 ± 0.4 −0.6 ± 0.2 10.4 ± 2.8 1.7 ± 0.2 −0.8 ± 0.0 Cadavers (n = 14)† 5.5 ± 4.6 0.3 ± 3.3 0.0 ± 0.7 FE model vs cadavers MD (95% CI) 1.0 (−0.9 to 2.9) −0.6 (−1.0 to −0.1) p values 0.28, 0.44 0.015, <0.0001
Values are mean ± SD unless indicated otherwise. Extension is represented by positive values and flexion by negative values. A negative value for subluxation indi-cates that the inferior (C-4) vertebral segment translated posteriorly in relation to the superior (C-3) vertebral segment.* The 95% CIs for MD were calculated using Welch’s t-test (i.e., with unequal variances). The p values are presented as Welch’s test, Wilcoxon-Mann-Whitney test.† All cadaver data from Hindman et al., 2016, Table 2.
TABLE 5. Finite element model estimates for peak strains in the cervical spinal cord during intubation with an intact cervical spine and with 2 forms of cervical spine injury using clinically normal intubation forces
Spinal Cord Strain Parameter Intact (stable) Spine Type II Odontoid Fracture Severe C3–4 Distractive-Flexion Injury
Peak minimum principal strain (compression), %* Macintosh −16.6 ± 2.7 −16.2 ± 3.8 −16.4 ± 2.5 Airtraq −7.1 ± 1.0 −0.8 ± 0.4 −4.4 ± 0 .7 p values† <0.0001, 0.0002 <0.0001, <0.0001 <0.0001, <0.0001Peak maximum principal strain (stretch), %* Macintosh 4.4 ± 0.4 4.7 ± 1.3 5.1 ± 0.6 Airtraq 2.5 ± 0.4 0.3 ± 0.1 1.6 ± 0.1 p values† <0.0001, 0.0001 <0.0001, 0.0001 <0.0001, 0.0001
Values are mean ± SD.* Intubation forces were those measured experimentally during patient intubations (n = 14) reported in Hindman et al., 2014 (Macintosh = 48.8 ± 15.8 N; Airtraq = 10.4 ± 2.8 N).† The p values are presented as Student t-test, Wilcoxon signed-rank test.
Unauthenticated | Downloaded 05/24/22 01:36 PM UTC

B. C. Gadomski et al.
J Neurosurg Spine Volume 28 • January 201818
compression and stretch), these strains are briefly applied (typically < 30 seconds) and do not exceed the thresholds for producing clinically apparent spinal cord injury. If they did, spinal cord injury with routine intubation in the pres-ence of an intact (stable) cervical spine would be common-place. Notably, in the 2 modeled injuries, using clinically normal Macintosh forces, peak cord strains did not exceed those observed during intubation when the spine was in-tact. Thus, consistent with the FE model’s predictions of small differences in spine motion between intact and in-jured states, the FE model predicts that the cervical spi-nal cord is not likely to experience injurious strain during Macintosh intubation in the presence of either a Type II odontoid fracture or a severe C3–4 distractive-flexion in-jury. Because the current FE model tends to underestimate subaxial motion in the intact (stable) spine, it is possible that the FE model underestimates the strains that would occur during intubation in the presence of the C3–4 injury (see Current Model Limitations).
Cord strain parameters were 2- to 20-fold less during Airtraq intubations than during Macintosh intubations. In the absence of prior injury, brief periods (seconds to min-utes) of moderate cord compression are relatively well tol-erated,7,11 whereas, with preexisting cord injury/compres-sion, the amount and duration of “tolerable” compression is likely to be much less.4 Thus, although accomplishing intubation with lesser cord strain is not necessarily “safer” in the setting of an uninjured cord, we speculate that ac-complishing intubation with less cord strain has the po-tential to be advantageous in the presence of preexisting cord injury. Additional studies are needed to determine the
magnitudes and durations of spinal cord strains that result in injury.
The Absence of Preconditioning Effects in the FE ModelUntil now, cadaver models have been the only method
of predicting motion of the injured cervical spine during endotracheal intubation. When cadavers are intubated, the first and second intubations appear to replicate the rela-tionship between the force applied by the laryngoscope and the motion of the cervical spine.27,28 However, with ad-ditional intubations (e.g., intubations 3, 4, 5), the motion/force (biomechanical) properties of the airway and spine change,27,28 a process referred to as tissue precondition-ing.37,71 As a result, in cadavers, the amount of laryngo-scope force required to accomplish intubation decreases by 20%–50% of the original (first intubation) values,27,28 and cervical spine motion also decreases.28 This raises the possibility that prior cadaver studies in which repeated intubations have been used in each cadaver (4–6 intuba-tions,24,33,41,67 9–16 intubations,34,54 or 52 intubations69) un-derestimate cervical spine motion that would occur during intubations in patients in whom greater (clinically normal) laryngoscope forces would be used. A fundamental advan-tage of the FE model over cadavers is that the biomechani-cal properties of the FE model are constant, and model outputs (spine motion and cord strain) are not dependent on the previous number of loading cycles.
Modeling Motion of the Intact Cervical SpineIn the upper cervical segments (Oc–C2), the patient, FE
model, and cadaver extension values were comparable (Ta-
FIG. 3. Finite element model strain field maps of minimum principal strain (compression) of the spinal cord during endotracheal intubation in the presence of an intact (stable) spine (A–D), Type II odontoid fracture (E–H), and severe C3–4 distractive-flexion injury (I–L). For these maps, the model was loaded with the normal (clinical average) Macintosh force profile (48.8 N) and the normal (clinical average) Airtraq force profile (10.4 N). Panels in the upper row show peak minimum principal strain in the midline sagittal plane. Panels in the lower row show peak minimum principal strain values in the transverse plane corresponding to the level of the cord with greatest minimum principal strain. The lower boundary of the scale (−1.00e−01 [−10%], red) is limited to enhance contrast among regions with varying strain. Black indicates minimum principal strain values exceeding -10%.
Unauthenticated | Downloaded 05/24/22 01:36 PM UTC

Finite element model of cervical spine and spinal cord
J Neurosurg Spine Volume 28 • January 2018 19
ble 2). In contrast, in the more caudad segments (especially C3–4 and C4–5), the extension values appeared to differ among patients, the FE model, and cadavers. Specifically, the FE model predicted slightly less average extension than was measured in patients. Differences in C2–5 exten-sion predicted by the FE model versus extension measured in patients (Macintosh ~4°; Airtraq ~2°) were small in comparison with the maximum extension that can occur in these segments (total C2–5 extension ~30°).72 Impor-tantly, at C2–5, cadaver extension values were even less than those predicted by the FE model. Thus, it appears that the baseline motion characteristics of cadaver seg-ments (especially subaxial segments) under typical (clini-cal) intubation forces do not necessarily replicate those of living patients. Thus, the current FE model appears to be superior to cadaver models in predicting the motion of in-tact (stable) subaxial segments.
Modeling Motion of the Injured Cervical SpineAs summarized in Table 3, the FE model closely pre-
dicted the average primary (experimentally measured) motion characteristics of the injured C-2 segment (Type II odontoid fracture) in cadavers intubated with both Mac-intosh and Airtraq laryngoscopes. This is consistent with our observation that the FE model and cadavers exhibit comparable motion in Oc–C1 and C1–2 segments in the intact (stable) state (Table 2 and Fig. 2).
In our prior cadaver C-2 injury study, to account for sub-clinical intubation forces caused by tissue preconditioning, we also reported corrected motion data, assuming a simple linear relationship between force and motion.28 We antici-pated that using a linear motion/force relationship would result in an overestimate of spinal motion, and the FE model indicates that this is so. As summarized in Table 3, using the clinically obtained values for intubation forces of Macintosh and Airtraq laryngoscopes, the FE model pre-dicted motions of the injured C-2 segment that were less than those predicted by linear force correction of the pri-mary cadaver data. Therefore, cadaver data cannot be read-ily back-corrected to adjust for preconditioning effects and nonlinear relationships between force and motion.
In our prior cadaver C3–4 injury study, the preinjury baseline C3–4 extension during Macintosh intubations (0.3° ± 3.0°) was much less than that observed in patients (5.1° ± 3.8°).27 Therefore, in this cohort of cadavers, prein-jury baseline motion/force characteristics of intact C3–4 segments were significantly different (less) than those of living patients. Although the FE model preinjury baseline C3–4 extension during Macintosh intubations (1.8° ± 0.0°) was also less than that observed in patients, it is consider-ably (~6-fold) greater than the baseline extension observed in the cadaver cohort. The same pattern was observed in the presence of C3–4 injury. As summarized in Table 4, in the presence of a severe distractive-flexion injury at C3–4, the FE model predicted greater (~8-fold) extension as well as greater (~3-fold) subluxation than was measured in ca-davers, particularly with the use of the high-force Macin-tosh laryngoscope. Rather than concluding that this finding demonstrates a limitation of the FE model, we contend that this finding suggests that the FE model is likely superior to cadaver models in predicting motion of injured subax-
ial segments. Nevertheless, because the current FE model tends to underestimate subaxial motion in the intact (sta-ble) spine, it is possible that the FE model underestimates motion that would occur during intubation in the presence of the C3–4 injury in living patients.
Current Model LimitationsFirst, when compared with patients, the current FE
model underestimates motion in intact subaxial segments. Lesser subaxial motion in the FE model may be due, at least in part, to the imposed kinematic constraint of the C-7 vertebral body. In a future version of the FE model, inclusion of additional caudal vertebral segments (T-1, T-2) will permit C-7 motion, and this may increase FE-mod-eled motion in subaxial segments. Although the difference between observed and predicted motion is quantitatively small in the intact (stable) spine, we cannot estimate how much this affects model predictions of motion and/or cord strain in the presence of subaxial injury.
Second, although most of the materials implemented in the FE model were defined with nonlinear material prop-erties, several material assignment simplifications were re-quired for computational purposes, most notably the linear elastic material definition assigned to the annulus fibrosis. While these simplifications directly affect model predic-tions of the localized mechanical environment of the disc (not germane to the current study), they do not alter the spinal kinetics, and they do not have an effect on the inter-nal mechanical parameter predictions of spinal cord strain.
Third, because model anatomy was derived from a sin-gle cadaver and mean material property data were used to define the model, the lack of geometric and material property input variation produces deterministic (i.e., sin-gle-valued) spinal kinematic behavior as compared with both the patient and cadaver cohorts, which return distri-butions of intervertebral motions. Accordingly, the current FE model does not simulate the inherent variation across the human population but rather represents an anthropo-metrical mean. In the future, to account for the variation in both geometry and material properties across the gen-eral population, probabilistic methods will be dovetailed with the current FE model. Probabilistic analyses allow for uncertainty and natural variation to be incorporated into FE models and have been used recently in FE analyses of the spine,22,23,25 hip,15,16,43,51 and knee.20,21,60,61 The under-lying principle of probabilistic analyses is that the input parameters (anatomy, material properties) are not defined by a single value but are strategically sampled from a dis-tribution that represents the population’s variation, and the model is solved many times to develop a distribution of the output variables of interest.17 Ultimately, these data will more accurately inform clinicians as to the magnitude of risk of spinal cord compression during intubation in the setting of specific injuries.
Fourth, the current FE model does not include a rep-resentation of CSF,59 which has been shown to affect FE model predictions of spinal cord compression under dy-namic loading conditions, with the CSF providing a damp-ening or “cushioning” effect. However, because quasi-static loading conditions were used in the current study, the absence of CSF is not likely to substantially affect the
Unauthenticated | Downloaded 05/24/22 01:36 PM UTC

B. C. Gadomski et al.
J Neurosurg Spine Volume 28 • January 201820
reported results. The inclusion of CSF in future modeling efforts will allow for predictions of transient changes in internal mechanical parameters (most notably, spinal cord stresses and strains), wherein both the duration and mag-nitude of supraphysiological cord compression has been shown to play a key role in the resulting acute and perma-nent neurological impairment.63
Fifth, our current FE model does not include an ex-plicit representation of spinal cord gray and white matter.35 These tissues may32 (or may not49) have different biome-chanical properties,5,65 and gray matter may have lesser strain tolerances than white matter.38,59 Thus, both cord strain fields65 and cord (gray vs white matter) susceptibil-ity to strain injury are likely more complex than are rep-resented in the current version of our FE model. Finally, some work indicates that not only strain but also the strain rate (the time rate of change of strain) play vital roles in the resulting neuronal injury, with greater strain rates causing greater damage.38
Model AdaptabilityThe FE model can predict cervical spine motion and
spinal cord strain with any type of laryngoscope. The only information that is required for any type of laryngoscope is the maximum force that is applied, the force vector, and the center point of force application relative to the cervical spine. Thus, intubation force data collected in patients with intact cervical spines with any type of laryngoscope can be used to predict the motion that would occur with that laryn-goscope in the presence of cervical spine injuries.
The FE model can predict cervical spine motion and spinal cord strain with any type of cervical spine injury or any combination of multiple injuries. The only informa-tion that is required by the FE model is bony anatomy and the nonbony structures (e.g., ligaments) that are affected by the injury. Future FE modeling studies may allow for determination of combinations of spinal abnormalities/in-juries and intubation devices that place patients at risk for injurious cervical spinal cord strain during intubation and/or identify laryngoscopes that are best suited to a specific form of injury.
Future variations of the FE model may be able to rep-licate cervical spine degenerative disease (spondylosis/ste-nosis). This would allow modeling of cord strains during intubation and/or other dynamic motion conditions in the presence of chronic cord compression.
ConclusionsWe have developed an FE model of the complete hu-
man cervical spine and spinal cord that closely predicts cervical spine motion of living patients with intact spines undergoing endotracheal intubation, albeit with slightly less motion in subaxial segments. Nevertheless, the FE model appears to be superior to cadavers in predicting subaxial motion and is superior to cadavers by being free of preconditioning effects. When compared with cadaver injury models, the FE model predicts measured motions in an injured C-2 segment and predicts greater motions in an injured subaxial (C3–4) segment. The FE model predicts the magnitude and location of spinal cord compressive and
tensile (stretch) strains, which are the likely determinants of cord injury. In the 2 modeled injuries, cord strains dur-ing intubation do not exceed clinically normal values and would seem unlikely to cause primary cord injury. The FE model can be adapted to study a wide range of cervical spine pathologies.
AcknowledgmentsThis study was supported by a National Institutes of Health
grant (R01EB012048) to Drs. Puttlitz, Hindman, and Santoni.
References 1. Aprahamian C, Thompson BM, Finger WA, Darin JC: Ex-
perimental cervical spine injury model: evaluation of airway management and splinting techniques. Ann Emerg Med 13:584–587, 1984
2. Austin N, Krishnamoorthy V, Dagal A: Airway management in cervical spine injury. Int J Crit Illn Inj Sci 4:50–56, 2014
3. Bain AC, Meaney DF: Tissue-level thresholds for axonal damage in an experimental model of central nervous system white matter injury. J Biomech Eng 122:615–622, 2000
4. Batchelor PE, Wills TE, Skeers P, Battistuzzo CR, Macleod MR, Howells DW, et al: Meta-analysis of pre-clinical studies of early decompression in acute spinal cord injury: a battle of time and pressure. PLoS One 8:e72659, 2013
5. Bhatnagar T, Liu J, Yung A, Cripton PA, Kozlowski P, Ox-land T: In vivo measurement of cervical spinal cord deforma-tion during traumatic spinal cord injury in a rodent model. Ann Biomed Eng 44:1285–1298, 2016
6. Bhatnagar T, Liu J, Yung A, Cripton P, Kozlowski P, Tetzlaff W, et al: Relating histopathology and mechanical strain in experimental contusion spinal cord injury in a rat model. J Neurotrauma 33:1685–1695, 2016
7. Carlson GD, Gorden CD, Oliff HS, Pillai JJ, LaManna JC: Sustained spinal cord compression: part I: time-dependent effect on long-term pathophysiology. J Bone Joint Surg Am 85-A:86–94, 2003
8. Crawford RP, Rosenberg WS, Keaveny TM: Quantitative computed tomography-based finite element models of the human lumbar vertebral body: effect of element size on stiff-ness, damage, and fracture strength predictions. J Biomech Eng 125:434–438, 2003
9. Crosby ET: Airway management in adults after cervical spine trauma. Anesthesiology 104:1293–1318, 2006
10. Dean NA, Mitchell BS: Anatomic relation between the nu-chal ligament (ligamentum nuchae) and the spinal dura mater in the craniocervical region. Clin Anat 15:182–185, 2002
11. Delamarter RB, Sherman J, Carr JB: Pathophysiology of spinal cord injury. Recovery after immediate and delayed decompression. J Bone Joint Surg Am 77:1042–1049, 1995
12. Donaldson WF III, Heil BV, Donaldson VP, Silvaggio VJ: The effect of airway maneuvers on the unstable C1-C2 segment. A cadaver study. Spine (Phila Pa 1976) 22:1215–1218, 1997
13. Donaldson WF III, Towers JD, Doctor A, Brand A, Donald-son VP: A methodology to evaluate motion of the unstable spine during intubation techniques. Spine (Phila Pa 1976) 18:2020–2023, 1993
14. Dooris AP, Goel VK, Grosland NM, Gilbertson LG, Wilder DG: Load-sharing between anterior and posterior elements in a lumbar motion segment implanted with an artificial disc. Spine (Phila Pa 1976) 26:E122–E129, 2001
15. Dopico-González C, New AM, Browne M: A computational tool for the probabilistic finite element analysis of an unce-mented total hip replacement considering variability in bone-implant version angle. Comput Methods Biomech Biomed Engin 13:1–9, 2010
Unauthenticated | Downloaded 05/24/22 01:36 PM UTC

Finite element model of cervical spine and spinal cord
J Neurosurg Spine Volume 28 • January 2018 21
16. Dopico-González C, New AM, Browne M: Probabilistic fi-nite element analysis of the uncemented hip replacement—ef-fect of femur characteristics and implant design geometry. J Biomech 43:512–520, 2010
17. Easley SK, Pal S, Tomaszewski PR, Petrella AJ, Rullkoetter PJ, Laz PJ: Finite element-based probabilistic analysis tool for orthopaedic applications. Comput Methods Programs Biomed 85:32–40, 2007
18. Fagan MJ, Julian S, Siddall DJ, Mohsen AM: Patient-specific spine models. Part 1: Finite element analysis of the lumbar intervertebral disc—a material sensitivity study. Proc Inst Mech Eng H 216:299–314, 2002
19. Farmer J, Vaccaro A, Albert TJ, Malone S, Balderston RA, Cotler JM: Neurologic deterioration after cervical spinal cord injury. J Spinal Disord 11:192–196, 1998
20. Fitzpatrick CK, Clary CW, Laz PJ, Rullkoetter PJ: Relative contributions of design, alignment, and loading variability in knee replacement mechanics. J Orthop Res 30:2015–2024, 2012
21. Fitzpatrick CK, Clary CW, Rullkoetter PJ: The role of pa-tient, surgical, and implant design variation in total knee replacement performance. J Biomech 45:2092–2102, 2012
22. Francis WL, Eliason TD, Thacker BH, Paskoff GR, Shender BS, Nicolella DP: Implementation and validation of probabi-listic models of the anterior longitudinal ligament and pos-terior longitudinal ligament of the cervical spine. Comput Methods Biomech Biomed Engin 17:905–916, 2014
23. Galbusera F, Anasetti F, Bellini CM, Costa F, Fornari M: The influence of the axial, antero-posterior and lateral positions of the center of rotation of a ball-and-socket disc prosthesis on the cervical spine biomechanics. Clin Biomech (Bristol, Avon) 25:397–401, 2010
24. Gerling MC, Davis DP, Hamilton RS, Morris GF, Vilke GM, Garfin SR, et al: Effects of cervical spine immobilization technique and laryngoscope blade selection on an unstable cervical spine in a cadaver model of intubation. Ann Emerg Med 36:293–300, 2000
25. Goel VK, Faizan A, Palepu V, Bhattacharya S: Parameters that effect spine biomechanics following cervical disc re-placement. Eur Spine J 21 (5 Suppl 5):S688–S699, 2012
26. Hastings RH, Kelley SD: Neurologic deterioration associated with airway management in a cervical spine-injured patient. Anesthesiology 78:580–583, 1993
27. Hindman BJ, Fontes RB, From RP, Traynelis VC, Todd MM, Puttlitz CM, et al: Intubation biomechanics: laryngoscope force and cervical spine motion during intubation in cadav-ers-effect of severe distractive-flexion injury on C3-4 motion. J Neurosurg Spine 25:545–555, 2016
28. Hindman BJ, From RP, Fontes RB, Traynelis VC, Todd MM, Zimmerman MB, et al: Intubation biomechanics: Laryngoscope force and cervical spine motion during intubation in cadavers—cadavers versus patients, the effect of repeated intubations, and the effect of Type II odontoid fracture on C1-C2 motion. Anesthesiology 123:1042–1058, 2015
29. Hindman BJ, Palecek JP, Posner KL, Traynelis VC, Lee LA, Sawin PD, et al: Cervical spinal cord, root, and bony spine injuries: a closed claims analysis. Anesthesiology 114:782–795, 2011
30. Hindman BJ, Santoni BG, Puttlitz CM, From RP, Todd MM: Intubation biomechanics: laryngoscope force and cervical spine motion during intubation with Macintosh and Airtraq laryngoscopes. Anesthesiology 121:260–271, 2014
31. Hino H, Abumi K, Kanayama M, Kaneda K: Dynamic mo-tion analysis of normal and unstable cervical spines using cineradiography. An in vivo study. Spine (Phila Pa 1976) 24:163–168, 1999
32. Ichihara K, Taguchi T, Shimada Y, Sakuramoto I, Kawano S, Kawai S: Gray matter of the bovine cervical spinal cord is
mechanically more rigid and fragile than the white matter. J Neurotrauma 18:361–367, 2001
33. Lennarson PJ, Smith D, Todd MM, Carras D, Sawin PD, Brayton J, et al: Segmental cervical spine motion during orotracheal intubation of the intact and injured spine with and without external stabilization. J Neurosurg 92 (2 Sup-pl):201–206, 2000
34. Lennarson PJ, Smith DW, Sawin PD, Todd MM, Sato Y, Traynelis VC: Cervical spinal motion during intubation: effi-cacy of stabilization maneuvers in the setting of complete seg-mental instability. J Neurosurg 94 (2 Suppl):265–270, 2001
35. Li XF, Dai LY: Three-dimensional finite element model of the cervical spinal cord: preliminary results of injury mecha-nism analysis. Spine (Phila Pa 1976) 34:1140–1147, 2009
36. Liang BA, Cheng MA, Tempelhoff R: Efforts at intubation: cervical injury in an emergency circumstance? J Clin Anes-th 11:349–352, 1999
37. Lim YJ, Deo D, Singh TP, Jones DB, De S: In situ measure-ment and modeling of biomechanical response of human cadaveric soft tissues for physics-based surgical simulation. Surg Endosc 23:1298–1307, 2009
38. Maikos JT, Shreiber DI: Immediate damage to the blood-spi-nal cord barrier due to mechanical trauma. J Neurotrauma 24:492–507, 2007
39. Maikos JT, Qian Z, Metaxas D, Shreiber DI: Finite element analysis of spinal cord injury in the rat. J Neurotrauma 25:795–816, 2008
40. Mayglothling J, Duane TM, Gibbs M, McCunn M, Legome E, Eastman AL, et al: Emergency tracheal intubation im-mediately following traumatic injury: an Eastern Association for the Surgery of Trauma practice management guideline. J Trauma Acute Care Surg 73 (5 Suppl 4):S333–S340, 2012
41. McCahon RA, Evans DA, Kerslake RW, McClelland SH, Hardman JG, Norris AM: Cadaveric study of movement of an unstable atlanto-axial (C1/C2) cervical segment during laryngoscopy and intubation using the Airtraq®, Macintosh and McCoy laryngoscopes. Anaesthesia 70:452–461, 2015
42. McLeod AD, Calder I: Spinal cord injury and direct laryngos-copy—the legend lives on. Br J Anaesth 84:705–709, 2000
43. Mehrez L, Browne M: A numerically validated probabilistic model of a simplified total hip replacement construct. Com-put Methods Biomech Biomed Engin 15:845–858, 2012
44. Muckart DJ, Bhagwanjee S, van der Merwe R: Spinal cord injury as a result of endotracheal intubation in patients with undiagnosed cervical spine fractures. Anesthesiology 87:418–420, 1997
45. Natarajan RN, Williams JR, Andersson GB: Recent advances in analytical modeling of lumbar disc degeneration. Spine (Phila Pa 1976) 29:2733–2741, 2004
46. Noailly J, Lacroix D, Planell JA: Finite element study of a novel intervertebral disc substitute. Spine (Phila Pa 1976) 30:2257–2264, 2005
47. Okada E, Matsumoto M, Ichihara D, Chiba K, Toyama Y, Fujiwara H, et al: Aging of the cervical spine in healthy vol-unteers: a 10-year longitudinal magnetic resonance imaging study. Spine (Phila Pa 1976) 34:706–712, 2009
48. Ollerton JE, Parr MJ, Harrison K, Hanrahan B, Sugrue M: Potential cervical spine injury and difficult airway man-agement for emergency intubation of trauma adults in the emergency department--a systematic review. Emerg Med J 23:3–11, 2006
49. Ozawa H, Matsumoto T, Ohashi T, Sato M, Kokubun S: Com-parison of spinal cord gray matter and white matter softness: measurement by pipette aspiration method. J Neurosurg 95 (2 Suppl):221–224, 2001
50. Park MS, Lee YB, Moon SH, Lee HM, Kim TH, Oh JB, et al: Facet joint degeneration of the cervical spine: a computed tomographic analysis of 320 patients. Spine (Phila Pa 1976) 39:E713–E718, 2014
Unauthenticated | Downloaded 05/24/22 01:36 PM UTC

B. C. Gadomski et al.
J Neurosurg Spine Volume 28 • January 201822
51. Pérez MA, Grasa J, García-Aznar JM, Bea JA, Doblaré M: Probabilistic analysis of the influence of the bonding degree of the stem-cement interface in the performance of cemented hip prostheses. J Biomech 39:1859–1872, 2006
52. Powell JF, Woodcock T, Luscombe FE: Atlanto-axial sublux-ation in Down’s syndrome. Anaesthesia 45:1049–1051, 1990
53. Powell RM, Heath KJ: Quadraplegia in a patient with an undiagnosed odontoid peg fracture. The importance of cervi-cal spine immobilisation in patients with head injuries. J R Army Med Corps 142:79–81, 1996
54. Prasarn ML, Conrad B, Rubery PT, Wendling A, Aydog T, Horodyski M, et al: Comparison of 4 airway devices on cervical spine alignment in a cadaver model with global ligamentous instability at C5–C6. Spine (Phila Pa 1976) 37:476–481, 2012
55. Prescher A: Anatomy and pathology of the aging spine. Eur J Radiol 27:181–195, 1998
56. Redl G: Massive pyramidal tract signs after endotracheal intubation: a case report of spondyloepiphyseal dysplasia congenita. Anesthesiology 89:1262–1264, 1998
57. Richter M, Wilke HJ, Kluger P, Claes L, Puhl W: Load-dis-placement properties of the normal and injured lower cervi-cal spine in vitro. Eur Spine J 9:104–108, 2000
58. Rohlmann A, Bauer L, Zander T, Bergmann G, Wilke HJ: De-termination of trunk muscle forces for flexion and extension by using a validated finite element model of the lumbar spine and measured in vivo data. J Biomech 39:981–989, 2006
59. Russell CM, Choo AM, Tetzlaff W, Chung TE, Oxland TR: Maximum principal strain correlates with spinal cord tissue damage in contusion and dislocation injuries in the rat cervi-cal spine. J Neurotrauma 29:1574–1585, 2012
60. Salas C, Mercer D, DeCoster TA, Reda Taha MM: Experi-mental and probabilistic analysis of distal femoral peripros-thetic fracture: a comparison of locking plate and intramed-ullary nail fixation. Part A: experimental investigation. Com-put Methods Biomech Biomed Engin 14:157–164, 2011
61. Salas C, Mercer D, DeCoster TA, Reda Taha MM: Experi-mental and probabilistic analysis of distal femoral peripros-thetic fracture: a comparison of locking plate and intramed-ullary nail fixation. Part B: probabilistic investigation. Com-put Methods Biomech Biomed Engin 14:175–182, 2011
62. Simpson AK, Biswas D, Emerson JW, Lawrence BD, Grauer JN: Quantifying the effects of age, gender, degeneration, and adjacent level degeneration on cervical spine range of motion using multivariate analyses. Spine (Phila Pa 1976) 33:183–186, 2008
63. Sjovold SG, Mattucci SF, Choo AM, Liu J, Dvorak MF, Kwon BK, et al: Histological effects of residual compres-sion sustained for 60 minutes at different depths in a novel rat spinal cord injury contusion model. J Neurotrauma 30:1374–1384, 2013
64. Sparrey CJ, Keaveny TM: The effect of flash freezing on variability in spinal cord compression behavior. J Biomech Eng 131:111010, 2009
65. Sparrey CJ, Manley GT, Keaveny TM: Effects of white, grey, and pia mater properties on tissue level stresses and strains in the compressed spinal cord. J Neurotrauma 26:585–595, 2009
66. Teraguchi M, Yoshimura N, Hashizume H, Muraki S, Ya-mada H, Minamide A, et al: Prevalence and distribution of intervertebral disc degeneration over the entire spine in a population-based cohort: the Wakayama Spine Study. Osteo-arthritis Cartilage 22:104–110, 2014
67. Turner CR, Block J, Shanks A, Morris M, Lodhia KR, Gujar SK: Motion of a cadaver model of cervical injury during en-dotracheal intubation with a Bullard laryngoscope or a Mac-intosh blade with and without in-line stabilization. J Trauma 67:61–66, 2009
68. Ueno K, Liu YK: A three-dimensional nonlinear finite ele-
ment model of lumbar intervertebral joint in torsion. J Bio-mech Eng 109:200–209, 1987
69. Wendling AL, Tighe PJ, Conrad BP, Baslanti TO, Horodyski M, Rechtine GR: A comparison of 4 airway devices on cervi-cal spine alignment in cadaver models of global ligamentous instability at C1-2. Anesth Analg 117:126–132, 2013
70. Whyne CM, Hu SS, Lotz JC: Parametric finite element analysis of vertebral bodies affected by tumors. J Biomech 34:1317–1324, 2001
71. Wilke HJ, Werner K, Häussler K, Reinehr M, Böckers TM: Thiel-fixation preserves the non-linear load-deformation characteristic of spinal motion segments, but increases their flexibility. J Mech Behav Biomed Mater 4:2133–2137, 2011
72. Wu SK, Kuo LC, Lan HC, Tsai SW, Chen CL, Su FC: The quantitative measurements of the intervertebral angulation and translation during cervical flexion and extension. Eur Spine J 16:1435–1444, 2007
73. Yaszemski MJ, Shepler TR: Sudden death from cord com-pression associated with atlanto-axial instability in rheuma-toid arthritis. A case report. Spine (Phila Pa 1976) 15:338–341, 1990
74. Yoganandan N, Kumaresan S, Pintar FA: Biomechanics of the cervical spine Part 2. Cervical spine soft tissue responses and biomechanical modeling. Clin Biomech (Bristol, Avon) 16:1–27, 2001
75. Yukawa Y, Kato F, Suda K, Yamagata M, Ueta T: Age-related changes in osseous anatomy, alignment, and range of motion of the cervical spine. Part I: Radiographic data from over 1,200 asymptomatic subjects. Eur Spine J 21:1492–1498, 2012
DisclosuresThe authors report the following. Dr. Todd: has received research funding from Karl Storz Endoscopy. Dr. Fontes: consultant for Medtronic and Stryker.
Author ContributionsConception and design: Hindman, Gadomski, Shetye, Puttlitz. Acquisition of data: Hindman, Gadomski, Shetye, Santoni, Todd, Traynelis, From, Fontes, Puttlitz. Analysis and interpretation of data: Hindman, Gadomski, Dexter, Santoni, Todd, Fontes, Put-tlitz. Drafting the article: Hindman. Critically revising the article: Hindman, Gadomski, Dexter, Puttlitz. Reviewed submitted ver-sion of manuscript: all authors. Approved the final version of the manuscript on behalf of all authors: Hindman. Statistical analysis: Dexter. Administrative/technical/material support: Hindman, San-toni, Puttlitz. Study supervision: Hindman, Santoni, Puttlitz.
Supplemental InformationOnline-Only ContentSupplemental material is available with the online version of the article.
Appendix. https://thejns.org/doi/suppl/10.3171/2017.5.SPINE17189.
Previous PresentationsPortions of the work were presented in poster format at the Inter-national Anesthesia Research Society 2016 Annual Meeting and International Science Symposium, San Francisco, California, May 21–24, 2016.
CorrespondenceBradley J. Hindman, Department of Anesthesia, University of Iowa Hospitals and Clinics, 200 Hawkins Dr., Iowa City, IA 52242. email: [email protected].
Unauthenticated | Downloaded 05/24/22 01:36 PM UTC























![InTech-Finite Element Analysis in Orthopaedic Biomechanics[1]](https://img.pdfslide.us/doc/110x75/577d29171a28ab4e1ea5f5fe/intech-finite-element-analysis-in-orthopaedic-biomechanics1.jpg)



