Embed Size (px)
Citation preview
ECDS CQUIN Implementation Guidance for Commissioners and Providers v1.2
ECDS CQUIN Implementation Guidance
1 IntroductionECDS submissions are incentivised from 1st October 2017 in the 2017/2019 CQUIN scheme (see appendix for more detail). There are 6 components to the ECDS part of the CQUIN:
Part 1: Q1 17/18 – Providers submit demonstrable and credible planning for a 1 October 2017 Go-live.
Parts 2-6: Q3 17/18 to Q4 18/19 – Providers are assessed on data quality and submission frequency in incrementally more challenging ways. Reports will be generated from the SUS+ system which will provide reliable metrics to both providers and commissioners.
The additional detail in this guidance is designed to suggest how commissioners may wish to judge whether the requirements have been met. Once agreed at a local level, Providers can start planning with confidence.
Note: at time of writing the CQUIN incentivises Type 1 and 2 emergency departments only.
2 Principles1. No “cliff edge” to the incentives:
a. If a Provider misses the 1st of October 2017 target we do not recommend that this leads to complete withholding of the CQUIN payment.
b. Instead we suggest a sliding scale, decreasing to zero over time, as described in this guidance.
2. When applying this CQUIN, data quality is more important than submission frequency, and it is recommended that weightings reflect this. However more frequent submissions should also be clearly rewarded.
3 Implementation Guidance
3.1 Introduction for Providers and commissionersThe CQUIN is based on sites being live on 1 October 2017.
However, it is not in anyone’s interest for a Provider which has not achieved this goal to then have no incentive to implement ECDS before 1 April 2018, and therefore if a Provider is gathering ECDS data from 1 December 2017 and submits data for all of December 2017, we suggest that a proportion of the CQUIN (for that quarter) should be payable. We propose a payment of 50% in this case.
3.2 Support to implement the CQUINThe following sections of the document represent NHS England’s recommendation to commissioners of how the scheme should be implemented.
A series of reports will be made available, via the SUS+ platform, to commissioners to enable a detailed view on how the provider has performed in relation to the recommended approach.
Page 1 of 121/6/2017
ECDS CQUIN Implementation Guidance for Commissioners and Providers v1.2
3.2.1 When to run reportsIt is suggested that all CQUIN parts except the first should be assessed around 10 working days following the end of the relevant quarter.
3.2.2 Notes
a) General data quality: the data quality of all data items is important, and the CQUIN reports will also show data quality for other data set items. If data quality is shown to be poor for other data items this will be visible to the commissioner and the commissioner is encouraged to apply penalties for unacceptably poor data quality or completeness.
b) Specific data quality items mentioned below: where this guidance document mentions a specific data item section 4.8 covers the detailed suggested rules for checking the completeness of that item.
c) SUS or MESH downtime: if SUS or an associated system or service is suffering from unplanned downtime or other service disruption this should be taken into account when applying the CQUIN payment to ensure that circumstances wholly beyond a Provider’s control do not cause financial penalty.
d) Arbitration and dispute resolution: The CQUIN Guidance talks about how commissioners and providers should go about agreeing the CQUIN scheme, specifically section 5.3 in the document found here:
www.england.nhs.uk/wp-content/uploads/2016/11/cquin-2017-19-guidance.pdf
Separately, there is a joint NHS England / NHS Improvement process which supports contract signature, see pdf below, and a dispute resolution process documented within the contract itself, which can be followed if a disagreement arises once the contract (and therefore the CQUIN scheme) is in place.
www.england.nhs.uk/wp-content/uploads/2015/12/ann-c-dispute.pdfe) Partial compliance: In the event that not every ED within a Provider Trust meets the
compliance timetable at the same time, then each ED should be treated separately and we recommend that CQUIN payments be divided pro rata according to the commissioned income / expenditure levels of each ED. For example, if a Trust has two EDs and one of them, which covers 60% of the commissioned value, meets the CQUIN fully whilst the other does not, then 60% of the CQUIN should be awarded to that Trust.
The following sections describe the detail on Parts 1 and 2 of the ECDS CQUIN along with a worked example, and parts 3-6 are described in the appendix.
3.3 CQUIN Part 1 (Q1 17/18) (demonstrable & credible plans)Plans should be submitted by Providers to their CCGs for assessment, before 30 June 2017. A credible plan should include both:
A written plan detailing the activities planned and A supporting activity schedule.
We also recommend that plans and key dates are shared with the ECDS implementation team via [email protected] so that we can schedule deployment support resource.
Based on the credibility of plans that have been submitted and the timescales they represent, commissioners may wish to adjust the CQUIN payment accordingly, i.e. if the Provider does not expect to go live on 1 October 2017 but shortly thereafter the CCG may wish to take extenuating circumstances into account.
Page 2 of 121/6/2017

ECDS CQUIN Implementation Guidance for Commissioners and Providers v1.2
In the case where a go-live date will be difficult to meet due to a supplier’s deployment schedule it may be preferable to refer to the central ECDS implementation team ([email protected]) for advice, as this team can see that national picture for each IT supplier.
Sample plans have been designed and further detail is available in the appendix.
3.4 CQUIN Part 2 (Q3 17/18)
3.4.1 Priority 1: Going live with the ECDS from 1 December 2017We recommend that Trusts which gather and submit data covering at least the whole of December 2017 receive 50% of the available CQUIN money for that part.
3.4.2 Priority 2: Data quality (Chief complaint and Diagnosis)We recommend that where valid / appropriate Diagnosis and Chief Complaint are present:
Greater than 95% (Good) attracts 40% of payment 90-95% (Medium) attracts 20% of payment <90% (Poor) No payment
3.4.3 Priority 3: Frequency and timeliness (10%)We recommend that 10% of the CQUIN be given pro-rata based on the number of submissions in the quarter containing at least the previous week’s data. There are 13 weeks in Q3 so we recommend that each weekly submission will get 1/13th of the remaining 10% CQUIN money. We recommend that each measurement week be checked to see if the submission contained data for the preceding 7 days.
To count as a weekly submission there is a deadline to submit the previous week’s data, and the table in section 4.2 gives the schedule of weekly submissions for CQUIN Part 2 (Q3 2017/18).
The appendix contains a worked example for CQUIN Part 2 (Q3 17/18), as well as further detail on the other parts of the CQUIN and data quality for specific data items.
Page 3 of 121/6/2017

ECDS CQUIN Implementation Guidance for Commissioners and Providers v1.2
4 Appendix
4.1 Guidance for CQUIN Part 1 (Q1 17/18) (demonstrable & credible plans)In addition to section 3.3 the following suggested approach may be used:
4.1.1 Sample Schedule
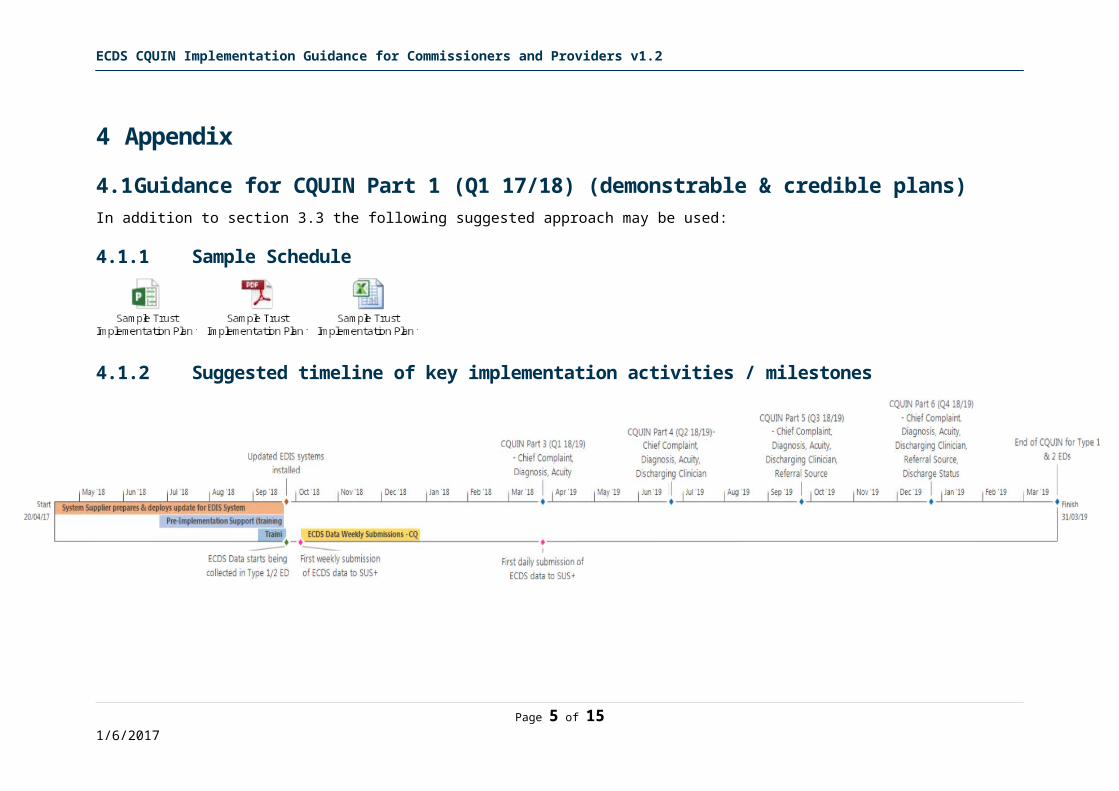
4.1.2 Suggested timeline of key implementation activities / milestones
Page 4 of 121/6/2017
ECDS CQUIN Implementation Guidance for Commissioners and Providers v1.2
4.1.3 Suggested Marking Schema for CCGsDescription of activity to be evidenced in plan and supporting schedule Plan Evidence RAG Score
Red: Not evidencedAmber: Partially evidencedGreen: Well evidenced
Schedule Evidence RAG ScoreRed: Not evidencedAmber: Partially evidencedGreen: Well evidenced
Notes:
Key information:1. Which Provider the plans are for Choose an item. Choose an item.2. Which ED(s) the plans are for Choose an item. Choose an item.3. When ECDS will start being collected in the ED Choose an item. Choose an item.4. Date of first submission to SUS+ Choose an item. Choose an item.5. Date when weekly submission to SUS+ will begin Choose an item. Choose an item.6. Date when daily submission to SUS+ will begin Choose an item. Choose an item.Engagement activities (evidence of support and commitment):
Trust senior management, including Directors of Finance and IT Choose an item. Choose an item. ED staff (management, clinical and clerical) Choose an item. Choose an item. ED Clinicians (Doctors, Nurses, etc.) Choose an item. Choose an item. ED Management and Clerical (Administration / Reception) staff Choose an item. Choose an item. Trust ICT department Choose an item. Choose an item. Trust information and analytics department Choose an item. Choose an item. Trust Administrators (incl. coding team) Choose an item. Choose an item. Ambulance staff (if they use / interact with Trust IT systems) Choose an item. Choose an item.
Engagement with system supplier/s (commitment and support): EDIS (Emergency Department Information System) Choose an item. Choose an item. Patient Administration Systems (PAS) if relevant Choose an item. Choose an item. Other relevant IT suppliers e.g. XML broker Choose an item. Choose an item. Where appropriate (where suppliers have multiple target sites), there
should be an overarching “all customer” supplier plan to more easily view clashes and tensions within overall rollout plans
Choose an item. Choose an item.
Consideration of risks and issues for the following key areas: Implementation into clinical environment Choose an item. Choose an item. Implementation of new ED IT system/s Choose an item. Choose an item. Clinical / patient safety (Hazard Assessment and workarounds) Choose an item. Choose an item. Training Choose an item. Choose an item.
Implementation Plan and Schedule – see model templates below for suggested high level activities:Early activity ahead of go-live (before 1 October 2017) Examples:
Business process changes Choose an item. Choose an item. Prepare communication materials Choose an item. Choose an item. Wall charts and laminated “crib sheets” for new code sets Choose an item. Choose an item. New questions “crib sheets” for receptionists / clinicians Choose an item. Choose an item. Posters / patient leaflets explaining the need for the new questions
being askedChoose an item. Choose an item.
Training needs for IT, clinical, clerical and ambulance staff Choose an item. Choose an item.Implementation first weeks (1-31 October 2017) Examples:
Floorwalkers (people with understanding of CDS011) to provide on-site support and remind staff to code activity properly
Choose an item. Choose an item.
Wall charts and “crib sheets” available Choose an item. Choose an item. Technical support available Choose an item. Choose an item.
Post Implementation (1 November 2017 onwards): CQUIN parts 3-6:e.g. covering plans to achieve daily feeds and also
meet the increasingly stringent data quality requirements of the Choose an item. Choose an item.
Page 5 of 121/6/2017

ECDS CQUIN Implementation Guidance for Commissioners and Providers v1.2
CQUIN
Page 6 of 121/6/2017

ECDS CQUIN Implementation Guidance for Commissioners and Providers v1.2
4.2 Worked example for CQUIN Part 2 (Q3 17/18)Based on a Commissioner implementing the CQUIN scheme as recommended above, here are some worked examples of how the payment would be applied.
NHS Digital will provide a report based on the recommended methodology, which the commissioner and Provider will be able to run from the SUS+ platform.
The reports will give a clear breakdown of the data submission quality / frequency / completeness etc. and will have weightings to which the commissioner can refer and decide whether to apply the recommended level of CQUIN payment or an alternative level.
The reports are designed to give commissioners a consistent view of Provider performance in line with the recommended approach, and at all times commissioners will be able to decide an alternative method of applying the CQUIN payment.
4.2.1 Example scenarios based on recommended criteriaScenari
oGo Live Date Data Quality (Diagnosis &
Chief Complaint)No. of weekly
submissions (out of 13)A 1 October 2017 95% (Good) 13B 20 November 2017 93% (Medium) 6C 1 December 2017 93% (Medium) 1D 2 December 2017 95% (Good) 4
4.2.2 Calculation of recommended CQUIN value for scenariosSay the maximum payment available for CQUIN Part 2 is £100.4.2.2.1 Going live (recommended £50)
A. £50 (data is for all of December 2017)B. £50 (data is for all of December 2017)C. £50 (data is for all of December 2017)D. £0 (data is not for all of December 2017)
4.2.2.2 Data quality (recommended £40)A. Good = £40B. Medium = £20C. Medium = £20D. Good = £40
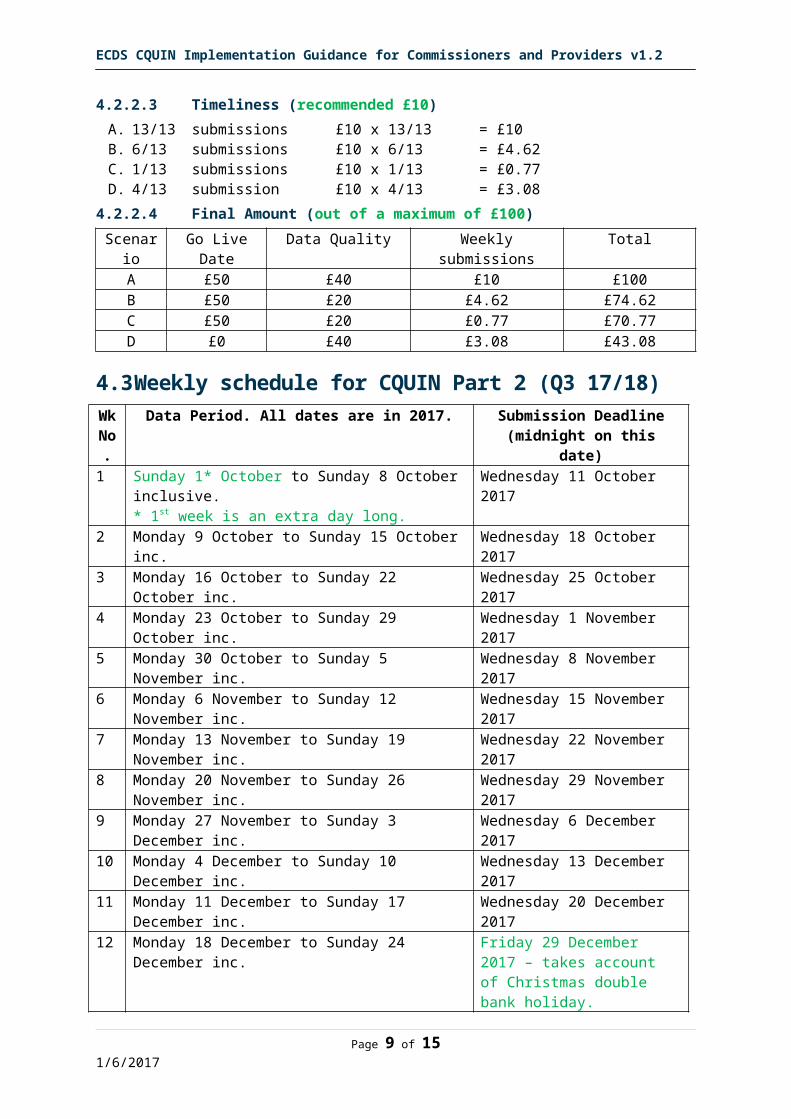
4.2.2.3 Timeliness (recommended £10)A. 13/13 submissions £10 x 13/13 = £10B. 6/13 submissions £10 x 6/13 = £4.62C. 1/13 submissions £10 x 1/13 = £0.77D. 4/13 submission £10 x 4/13 = £3.08
4.2.2.4 Final Amount (out of a maximum of £100)Scenari
oGo Live Date Data Quality Weekly submissions Total
A £50 £40 £10 £100B £50 £20 £4.62 £74.62C £50 £20 £0.77 £70.77D £0 £40 £3.08 £43.08
Page 7 of 121/6/2017

ECDS CQUIN Implementation Guidance for Commissioners and Providers v1.2
4.3 Weekly schedule for CQUIN Part 2 (Q3 17/18)Wk No.
Data Period. All dates are in 2017. Submission Deadline (midnight on this date)
1 Sunday 1* October to Sunday 8 October inclusive.* 1st week is an extra day long.
Wednesday 11 October 2017
2 Monday 9 October to Sunday 15 October inc. Wednesday 18 October 20173 Monday 16 October to Sunday 22 October inc. Wednesday 25 October 20174 Monday 23 October to Sunday 29 October inc. Wednesday 1 November 20175 Monday 30 October to Sunday 5 November inc. Wednesday 8 November 20176 Monday 6 November to Sunday 12 November inc. Wednesday 15 November
20177 Monday 13 November to Sunday 19 November inc. Wednesday 22 November
20178 Monday 20 November to Sunday 26 November inc. Wednesday 29 November
20179 Monday 27 November to Sunday 3 December inc. Wednesday 6 December 201710 Monday 4 December to Sunday 10 December inc. Wednesday 13 December
201711 Monday 11 December to Sunday 17 December inc. Wednesday 20 December
201712 Monday 18 December to Sunday 24 December inc. Friday 29 December 2017 –
takes account of Christmas double bank holiday.
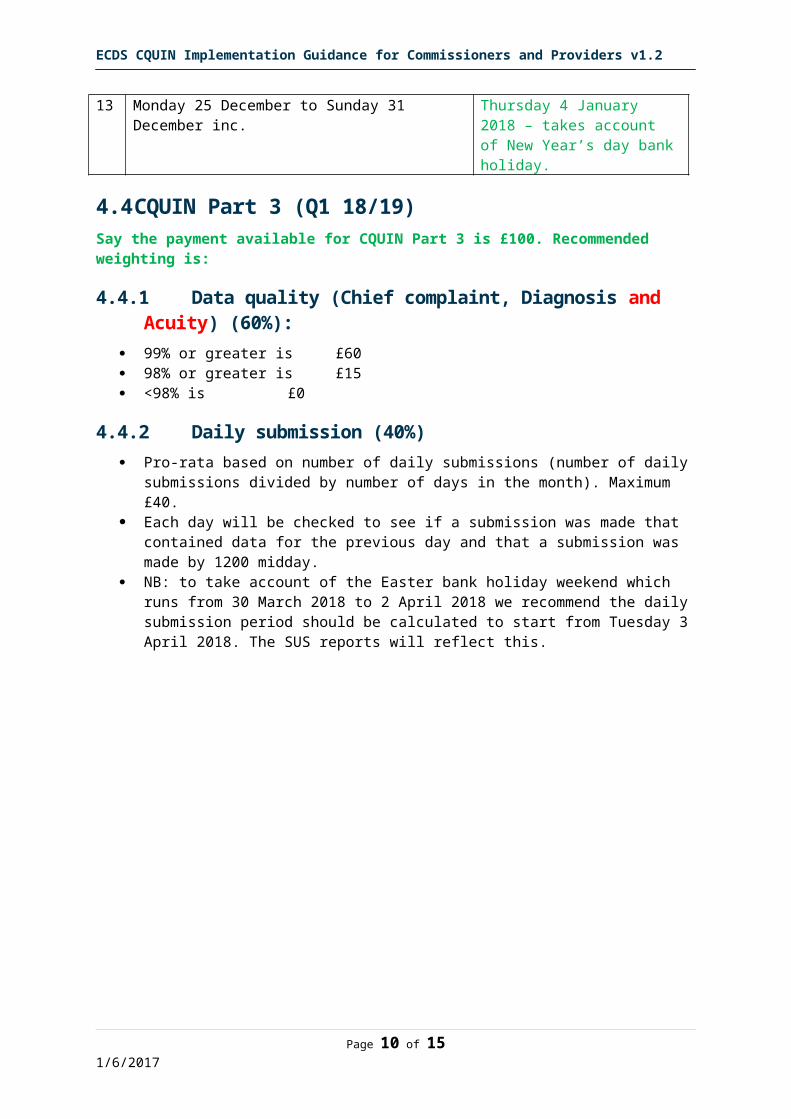
13 Monday 25 December to Sunday 31 December inc. Thursday 4 January 2018 – takes account of New Year’s day bank holiday.
4.4 CQUIN Part 3 (Q1 18/19)Say the payment available for CQUIN Part 3 is £100. Recommended weighting is:
4.4.1 Data quality (Chief complaint, Diagnosis and Acuity) (60%): 99% or greater is £60 98% or greater is £15 <98% is £0
4.4.2 Daily submission (40%) Pro-rata based on number of daily submissions (number of daily submissions divided
by number of days in the month). Maximum £40. Each day will be checked to see if a submission was made that contained data for
the previous day and that a submission was made by 1200 midday. NB: to take account of the Easter bank holiday weekend which runs from 30 March
2018 to 2 April 2018 we recommend the daily submission period should be calculated to start from Tuesday 3 April 2018. The SUS reports will reflect this.
Page 8 of 121/6/2017
ECDS CQUIN Implementation Guidance for Commissioners and Providers v1.2
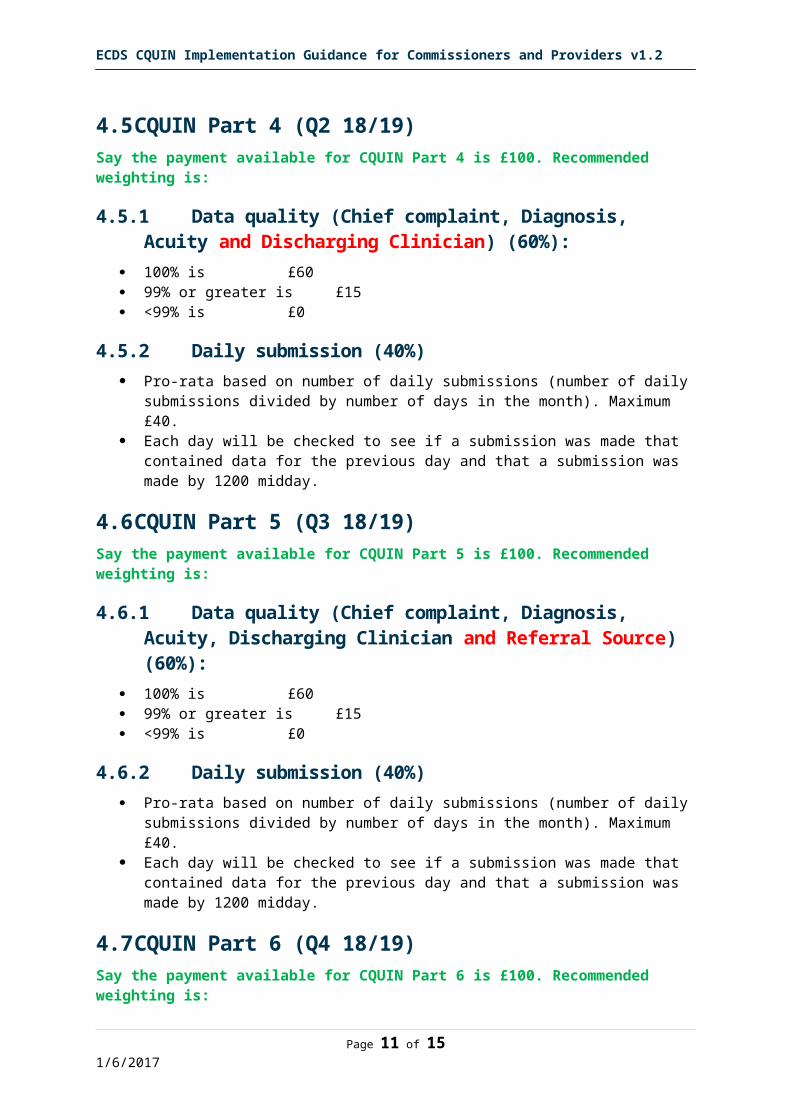
4.5 CQUIN Part 4 (Q2 18/19)Say the payment available for CQUIN Part 4 is £100. Recommended weighting is:
4.5.1 Data quality (Chief complaint, Diagnosis, Acuity and Discharging Clinician) (60%):
100% is £60 99% or greater is £15 <99% is £0
4.5.2 Daily submission (40%) Pro-rata based on number of daily submissions (number of daily submissions divided
by number of days in the month). Maximum £40. Each day will be checked to see if a submission was made that contained data for
the previous day and that a submission was made by 1200 midday.
4.6 CQUIN Part 5 (Q3 18/19)Say the payment available for CQUIN Part 5 is £100. Recommended weighting is:
4.6.1 Data quality (Chief complaint, Diagnosis, Acuity, Discharging Clinician and Referral Source) (60%):
100% is £60 99% or greater is £15 <99% is £0
4.6.2 Daily submission (40%) Pro-rata based on number of daily submissions (number of daily submissions divided
by number of days in the month). Maximum £40. Each day will be checked to see if a submission was made that contained data for
the previous day and that a submission was made by 1200 midday.
4.7 CQUIN Part 6 (Q4 18/19)Say the payment available for CQUIN Part 6 is £100. Recommended weighting is:
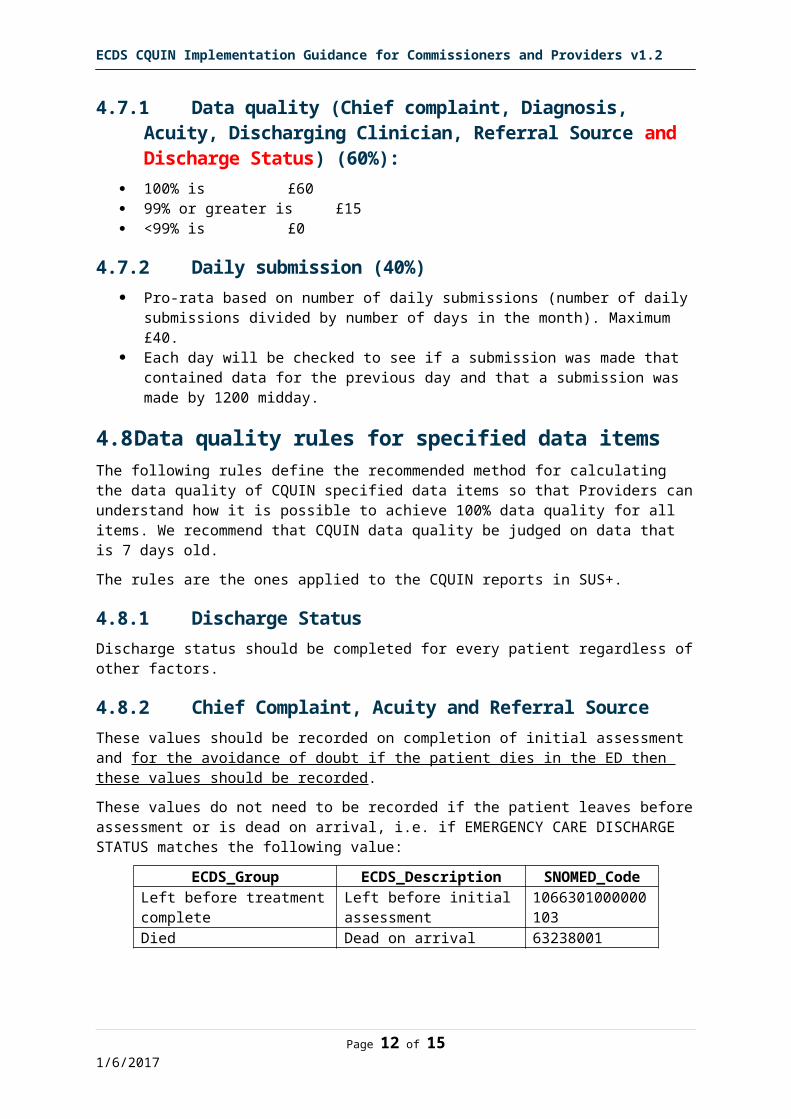
4.7.1 Data quality (Chief complaint, Diagnosis, Acuity, Discharging Clinician, Referral Source and Discharge Status) (60%):
100% is £60 99% or greater is £15 <99% is £0
4.7.2 Daily submission (40%) Pro-rata based on number of daily submissions (number of daily submissions divided
by number of days in the month). Maximum £40. Each day will be checked to see if a submission was made that contained data for
the previous day and that a submission was made by 1200 midday.
Page 9 of 121/6/2017
ECDS CQUIN Implementation Guidance for Commissioners and Providers v1.2
4.8 Data quality rules for specified data itemsThe following rules define the recommended method for calculating the data quality of CQUIN specified data items so that Providers can understand how it is possible to achieve 100% data quality for all items. We recommend that CQUIN data quality be judged on data that is 7 days old.
The rules are the ones applied to the CQUIN reports in SUS+.
4.8.1 Discharge StatusDischarge status should be completed for every patient regardless of other factors.
4.8.2 Chief Complaint, Acuity and Referral SourceThese values should be recorded on completion of initial assessment and for the avoidance of doubt if the patient dies in the ED then these values should be recorded.
These values do not need to be recorded if the patient leaves before assessment or is dead on arrival, i.e. if EMERGENCY CARE DISCHARGE STATUS matches the following value:
ECDS_Group ECDS_Description SNOMED_CodeLeft before treatment complete Left before initial assessment 1066301000000103Died Dead on arrival 63238001
4.8.3 Diagnosis and Discharging ClinicianFor the avoidance of doubt if the patient dies in the ED then these data items should be recorded.
Diagnosis and Discharging Clinician do not need to be recorded if the patient is streamed to another service, or leaves before treatment is completed, or is dead on arrival i.e. if EMERGENCY CARE DISCHARGE STATUS is any of the following values:
ECDS_Group ECDS_Description SNOMED_CodeStreamed at assessment Streamed to primary care service / GP 1077021000000100Streamed at assessment Streamed to Urgent Care Centre 1077031000000103Streamed at assessment Streamed to Emergency Department 1077781000000101Streamed at assessment Streamed to Ambulatory Emergency Care service 1077081000000104Streamed at assessment Streamed to falls service 1077091000000102Streamed at assessment Streamed to frailty service 1077101000000105Streamed at assessment Streamed to mental health service 1077041000000107Streamed at assessment Streamed to pharmacy service 1077071000000101Streamed at assessment Streamed to dental service 1077051000000105Streamed at assessment Streamed to ophthalmology service 1077061000000108Left before treatment complete
Left before initial assessment 1066301000000103
Left before treatment complete
Left after assessment with intent to attend other healthcare provider
1066311000000101
Left before treatment complete
Left after assessment but before treatment complete (destination unknown)
1066321000000107
Died Dead on arrival 63238001
Page 10 of 121/6/2017
ECDS CQUIN Implementation Guidance for Commissioners and Providers v1.2
4.8.4 Clinics and scheduled return patientsFor patients that attend a clinic or other form of scheduled return, i.e. if Attendance Category is the following value then Discharge Status, Chief Complaint, Acuity, Referral Source, Diagnosis and Discharging Clinician do not need to be recorded to achieve 100% of the CQUIN.
ECDS_UniqueID Sort1 ECDS_Description ECDS_Code
2018511100 51 PLANNED FOLLOW-up emergency care attendance within 7 days of the emergency care attendance at THIS emergency care department
4
4.9 Extract from the 2017/19 CQUIN schemeDate / period milestone relates to
Rules for achievement of milestones (including evidence to be supplied to commissioner)
Date milestone to be reported
Q1 Year 1 (2017/18)Part b)
Q3 Year 1Part b)
i) Type 1 or 2 A&E provider has demonstrable and credible planning in place to make the required preparations (e.g. by upgrading IT systems and training staff) so that the Emergency Care Data Set (ECDS) can be collected and returned from 1st October 2017.
ii) Type 1 or 2 A&E provider is returning data at least weekly AND 95% of patients have both a valid Chief Complaint and a Diagnosis (unless that patient is streamed to another service) so that 95% of patients have a diagnosis. Chief complaint should be any value from the ECDS Chief Complaint code set (SNOMED CT). Diagnosis should be any value from the ECDS diagnosis code set (SNOMED CT).
End of Quarter 1
End of Quarter 3
Q1 Year 2Part b)
Q1 Year 2Part b)
Q1 Year 2Part b)
Type 1 or 2 A&E provider is returning data daily AND 99% of patients have both a valid Chief Complaint and a Diagnosis (unless that patient is streamed to another service) so that 99% of patients have a diagnosis AND 99% of patients have a measure of acuity recorded. Acuity should be any value from the ECDS acuity set.
Type 1 or 2 A&E provider is returning data daily AND 100% of patients have both a valid Chief Complaint and a Diagnosis (unless that patient is streamed to another service) so that 100% of patients have a diagnosis AND 100% of patients have a measure of acuity recorded AND 100% of patients record the discharging clinician (using the GMC/NMC/HCPC number).
Type 1 or 2 A&E provider is returning data daily AND 100% of patients have both a valid Chief Complaint and a Diagnosis (unless that patient is streamed to another service) so that 100% of patients have a diagnosis AND 100% of patients have a measure of acuity recorded AND 100% of patients record the discharging clinician (using the GMC/NMC/HCPC number) AND 100% of patients have the referral source recorded. Referral source should be any value from the EDCS referral source set.
End of Q1
End of Q2
End of Q3
Q1 Year 2Part b)
Type 1 or 2 A&E provider is returning data daily AND 100% of patients have both a valid Chief Complaint and a Diagnosis (unless that patient is streamed to another service) so that 100% of patients have a diagnosis AND 100% of patients have a measure of acuity recorded AND 100% of patients record the discharging clinician (using the GMC/NMC/HCPC number) AND 100% of patients have the referral source recorded AND 100% of patients have discharge status recorded. Discharge status should be any value from the EDCS discharge status set.
End of Q4
4.10 CQUIN full spec (ECDS is in indicator 8a):
Page 11 of 121/6/2017
ECDS CQUIN Implementation Guidance for Commissioners and Providers v1.2
4.11 CQUIN Value Calculator
Page 12 of 121/6/2017