Embed Size (px)
Citation preview

Introduction toIntroduction toRandomized Clinical TrialsRandomized Clinical Trials
Deborah GradyDeborah Grady
Professor of MedicineProfessor of Medicine
University of California, San University of California, San FranciscoFrancisco

Randomized TrialsRandomized Trials
–RationaleRationale–Basic designsBasic designs–ParticipantsParticipants–InterventionIntervention–BlindingBlinding–OutcomesOutcomes–AdherenceAdherence–Follow-upFollow-up

RationaleRationale
•Why do a randomized blinded trialWhy do a randomized blinded trial–minimize confoundingminimize confounding–minimize co-interventionsminimize co-interventions–minimize biased outcome ascertainmentminimize biased outcome ascertainment
•Why not do a randomized trialWhy not do a randomized trial–major ethical issuesmajor ethical issues–narrow research questionnarrow research question–expensiveexpensive–long time from idea to paperlong time from idea to paper
•Generally reserved for mature Generally reserved for mature questionsquestions

Basic Trial DesignBasic Trial Design
PopulationPopulation
SampleSample
InterventionIntervention
RandomizationRandomization
OutcomeOutcomeOutcomeOutcome
ControlControlControlControl OutcomeOutcomeOutcomeOutcome
+ Blinding+ Blinding+ Blinding+ Blinding
PlaceboPlacebo

RandomizationRandomization
•Participants are assigned to Participants are assigned to treatment groups by chance treatment groups by chance with a known probabilitywith a known probability
•Random number table or computerRandom number table or computer
•Tamper-proof systemTamper-proof system–ordered, sealed envelopes ordered, sealed envelopes –centralized system (phone, fax, centralized system (phone, fax, web)web)

Value of RandomizationValue of Randomization
•Balances Balances baselinebaseline characteristics of the characteristics of the treatment groupstreatment groups–eliminates confounding due to eliminates confounding due to measured measured andand unmeasuredunmeasured factors factors
–provides an unbiased comparison provides an unbiased comparison between groupsbetween groups
•Does Does NOTNOT maintain balance maintain balance after randomizationafter randomization

Variations of RandomizationVariations of Randomization
•Fixed Allocation - probability fixedFixed Allocation - probability fixed–Simple - flip a coinSimple - flip a coin–Blocked - randomize consecutive small Blocked - randomize consecutive small batchesbatches
–Stratified - separate randomization in Stratified - separate randomization in stratastrata
–Clustered - randomize groupsClustered - randomize groups
•Adaptive - probability changes Adaptive - probability changes –N in the groups (biased coin) N in the groups (biased coin) –baseline characteristicsbaseline characteristics–outcome (play the winner; two-armed outcome (play the winner; two-armed bandit)bandit)

Cross-over DesignCross-over Design
PopulationPopulation
SampleSample
InterventionIntervention
RandomizationRandomization
PlaceboPlacebo
WashoutWashout
WashoutWashout
PlaceboPlacebo
InterventionIntervention
OutcomeOutcome OutcomeOutcome

Factorial DesignFactorial Design
PopulationPopulation
SampleSample
Int A and Int BInt A and Int B
Int A and Pbo BInt A and Pbo B
Pbo A and Int BPbo A and Int B
Pbo A and Pbo BPbo A and Pbo B
OutcomeOutcome
OutcomeOutcome
OutcomeOutcome
OutcomeOutcome

Vitamin D and Strength in the Vitamin D and Strength in the ElderlyElderly
• MMuscle strength and renal uscle strength and renal function decline with agingfunction decline with aging
•Declining renal function Declining renal function results in low levels of 1,25 Dresults in low levels of 1,25 D
•Vitamin D deficiency causes Vitamin D deficiency causes myopathy and treatment improves myopathy and treatment improves strengthstrengthRQ: Does treatment with vitamin D
improve strength?RQ: Does treatment with vitamin D
improve strength?

ParticipantsParticipants
•Inclusion criteria to Inclusion criteria to maximize:maximize:–rate of outcomes (old, weak)rate of outcomes (old, weak)–likely benefit from intervention likely benefit from intervention (renal dz, institutionalized, (renal dz, institutionalized, vitamin D deficiency)vitamin D deficiency)
–generalizabilitygeneralizability–ease of recruitmentease of recruitment
(none of the above)(none of the above)(none of the above)(none of the above)

Exclusion CriteriaExclusion Criteria
• Intervention unsafeIntervention unsafe• Intervention unlikely to be effectiveIntervention unlikely to be effective• Unlikely to adhere to the Unlikely to adhere to the interventionintervention– Run inRun in
• Unlikely to complete follow-upUnlikely to complete follow-up
• Practical problemsPractical problems
Practice Parsimony
Preserve Generalizability
Practice Parsimony
Preserve Generalizability

Choice of InterventionChoice of Intervention
•MaximizeMaximize–effectiveness effectiveness (highest (highest tolerable dose)tolerable dose)
–safety safety (lowest effective dose)(lowest effective dose)–generalizabilitygeneralizability–trial design/conducttrial design/conduct
•recruitmentrecruitment•compliancecompliance•blindingblinding

Vitamin D for Muscle StrengthVitamin D for Muscle Strength
•Consider Consider –DoseDose - in renal insufficiency 0.25 - in renal insufficiency 0.25 - 1.0 ug SQ 1,25 D daily - 1.0 ug SQ 1,25 D daily normalizes calciumnormalizes calcium
–DurationDuration - few months usually - few months usually restores strength in patients with restores strength in patients with rickets and myopathyrickets and myopathy
–RouteRoute - SQ vs. PO? - SQ vs. PO?–TitrationTitration to normal 1, 25-D level to normal 1, 25-D level or normal (safe) urine calcium?or normal (safe) urine calcium?

Choice of ControlChoice of Control
•Inert placebo usually bestInert placebo usually best
•Active therapy or “standard of Active therapy or “standard of care”care”– Active Comparator Trial - new therapy more Active Comparator Trial - new therapy more effective than standardeffective than standard• Ho: two treatments equally effectiveHo: two treatments equally effective• Ha: one treatment more effectiveHa: one treatment more effective
– Equivalence Trial - new therapy equivalentEquivalence Trial - new therapy equivalent• Ho: two treatments differ by at least XHo: two treatments differ by at least X• Ha: two treatments differ by less than XHa: two treatments differ by less than X

Equivalence TrialsEquivalence Trials
•AdvantageAdvantage–answers clinical questionanswers clinical question–may be more ethicalmay be more ethical
•DisadvantageDisadvantage–maymay require larger sample size require larger sample size–negative result may be due to low negative result may be due to low powerpower
–can’t tell if either better than can’t tell if either better than placeboplacebo
Only reasonable if potential Only reasonable if potential advantage of new therapyadvantage of new therapy
Only reasonable if potential Only reasonable if potential advantage of new therapyadvantage of new therapy

Trial of New Depression DrugTrial of New Depression Drug
•Approved SSRIs effective for Approved SSRIs effective for depression, but often cause depression, but often cause loss of libidoloss of libido
•New drug thought to be as New drug thought to be as effective as old with no effective as old with no effect on libidoeffect on libido
•Untreated depression can Untreated depression can result in suicideresult in suicide

Trial of Smiletraline for Trial of Smiletraline for DepressionDepression
•Placebo controlled trial–expected improvement 25% over placebo–Ho: no difference Ha: 20% difference with a =.05, b =.90
–sample size 100/group
•Compare smiletraline to sertraline–expect no difference–Ho: difference no greater than +/-10%–sample size 125/group

Why Blind?Why Blind?
•Maintains balanced groups Maintains balanced groups during follow-upduring follow-up
•Eliminates Eliminates –cointerventioncointervention–biased outcome ascertainmentbiased outcome ascertainment–biased measurement of outcomebiased measurement of outcome

Physicians’ Health StudyPhysicians’ Health StudyPhysicians’ Health StudyPhysicians’ Health Study
• 22,071 male physicians22,071 male physicians
• Aspirin 325 mg QOD or placeboAspirin 325 mg QOD or placebo
• Follow-up 5 yearsFollow-up 5 years
• Outcomes - CVD events and deathOutcomes - CVD events and death
• Many physicians had study drug Many physicians had study drug tested for ASAtested for ASA
• 22,071 male physicians22,071 male physicians
• Aspirin 325 mg QOD or placeboAspirin 325 mg QOD or placebo
• Follow-up 5 yearsFollow-up 5 years
• Outcomes - CVD events and deathOutcomes - CVD events and death
• Many physicians had study drug Many physicians had study drug tested for ASAtested for ASA

CointerventionsCointerventions
•Unintended effective interventionsUnintended effective interventions–participantsparticipants use other therapy or use other therapy or change behaviorchange behavior
–study staff, medical providers, study staff, medical providers, family or friendsfamily or friends treat participants treat participants differentlydifferently
•Nondifferential - decreases powerNondifferential - decreases power
•Differential - causes biasDifferential - causes bias

Oral Contraceptive Pills Oral Contraceptive Pills to Prevent Pregnancy to Prevent Pregnancy
Oral Contraceptive Pills Oral Contraceptive Pills to Prevent Pregnancy to Prevent Pregnancy
• 18,000 women age 21-35 years18,000 women age 21-35 years
• Randomly assigned to OCPs or Randomly assigned to OCPs or usual birth control methodusual birth control method
• Followed Q6 months for 2 Followed Q6 months for 2 yearsyears
• Pregnancy risk decreased 75%Pregnancy risk decreased 75%
• VTE risk increased 5-foldVTE risk increased 5-fold
• 18,000 women age 21-35 years18,000 women age 21-35 years
• Randomly assigned to OCPs or Randomly assigned to OCPs or usual birth control methodusual birth control method
• Followed Q6 months for 2 Followed Q6 months for 2 yearsyears
• Pregnancy risk decreased 75%Pregnancy risk decreased 75%
• VTE risk increased 5-foldVTE risk increased 5-fold

Biased Outcome Biased Outcome AscertainmentAscertainmentBiased Outcome Biased Outcome AscertainmentAscertainment
• If group assignment is known If group assignment is known – participantsparticipants may report may report symptoms or outcomes symptoms or outcomes differentlydifferently
– physicians or investigatorsphysicians or investigators may elicit symptoms or may elicit symptoms or outcomes differently outcomes differently
• If group assignment is known If group assignment is known – participantsparticipants may report may report symptoms or outcomes symptoms or outcomes differentlydifferently
– physicians or investigatorsphysicians or investigators may elicit symptoms or may elicit symptoms or outcomes differently outcomes differently

Canadian Cooperative MS TrialCanadian Cooperative MS TrialCanadian Cooperative MS TrialCanadian Cooperative MS Trial
•165 patients with multiple 165 patients with multiple sclerosissclerosis–plasma exchange + cyclo + predplasma exchange + cyclo + pred–sham plasma exchange + placebo medssham plasma exchange + placebo meds
•Outcome = structured neurologic Outcome = structured neurologic exam by blinded and unblinded exam by blinded and unblinded neurologistsneurologists
•More improvement with plasma More improvement with plasma exchange by unblinded, but not exchange by unblinded, but not blinded assessmentblinded assessment
•165 patients with multiple 165 patients with multiple sclerosissclerosis–plasma exchange + cyclo + predplasma exchange + cyclo + pred–sham plasma exchange + placebo medssham plasma exchange + placebo meds
•Outcome = structured neurologic Outcome = structured neurologic exam by blinded and unblinded exam by blinded and unblinded neurologistsneurologists
•More improvement with plasma More improvement with plasma exchange by unblinded, but not exchange by unblinded, but not blinded assessmentblinded assessmentNoseworthy, Neurology, 1994
Noseworthy, Neurology, 1994

Biased Outcome AdjudicationBiased Outcome Adjudication
•Study staff who decide if a Study staff who decide if a change or outcome has occurred change or outcome has occurred maymay–classify similar events classify similar events differently in treatment groupsdifferently in treatment groups
•Problematic with “soft” Problematic with “soft” outcomesoutcomes–investigator judgementinvestigator judgement–participant reported symptoms, participant reported symptoms, scalesscales

Why Not Blind?Why Not Blind?
• ImpossibleImpossible– surgerysurgery– exerciseexercise– dietdiet– educationeducation
• Possible, butPossible, but– dangerousdangerous– painfulpainful– cumbersomecumbersome

Is It Really Blinded? Is It Really Blinded? Is It Really Blinded? Is It Really Blinded?
• Difficult even for drugsDifficult even for drugs– identical placebo difficult to identical placebo difficult to prepareprepare
– drug may smell, taste, feel drug may smell, taste, feel differentdifferent
– drug may cause side effectsdrug may cause side effects– test results may unblindtest results may unblind– participants may test drugparticipants may test drug
• Difficult even for drugsDifficult even for drugs– identical placebo difficult to identical placebo difficult to prepareprepare
– drug may smell, taste, feel drug may smell, taste, feel differentdifferent
– drug may cause side effectsdrug may cause side effects– test results may unblindtest results may unblind– participants may test drugparticipants may test drug

What if You “Can’t” What if You “Can’t” Blind?Blind?
•Be courageousBe courageous
•Do the best you canDo the best you can–minimize differential minimize differential cointerventioncointervention
–blind those measuring outcome blind those measuring outcome –use “hard” outcomesuse “hard” outcomes
•Measure degree of unblindingMeasure degree of unblinding

Be CourageousBe Courageous
•Laparoscopic lysis of adhesions Laparoscopic lysis of adhesions for pelvic painfor pelvic pain
•Internal mammary ligation for Internal mammary ligation for anginaangina
•Orthoscopic debridement for OAOrthoscopic debridement for OA
•Sham burr holes for fetal Sham burr holes for fetal tissue implants for Parkinson’stissue implants for Parkinson’s

Do the Best You CanDo the Best You Can
•Exercise to prevent coronary Exercise to prevent coronary eventsevents–exercise - supervised exercise to exercise - supervised exercise to 80% maximum capacity 30 min 3/wk80% maximum capacity 30 min 3/wk
–control - supervised exercise to control - supervised exercise to 40% maximum capacity 30 min 3/wk40% maximum capacity 30 min 3/wk
•Psychotherapy for schizophreniaPsychotherapy for schizophrenia–therapy - psychotherapy weeklytherapy - psychotherapy weekly–control - advice about diet, control - advice about diet, exercise, and smoking weeklyexercise, and smoking weekly

Use a “Hard” OutcomeUse a “Hard” Outcome
• DeathDeath
• MeasurementsMeasurements– test resultstest results
• MVOMVO2 2 vs.. self-reported exercise vs.. self-reported exercise abilityability
• Doppler evaluation vs.. swollen Doppler evaluation vs.. swollen leg for DVT leg for DVT
– scales and diaries vs. investigator scales and diaries vs. investigator judgmentjudgment• Geriatric Depression Scale vs. Geriatric Depression Scale vs. “improved”“improved”
• 7-day urinary diary vs. “dry”7-day urinary diary vs. “dry”

AdherenceAdherence
•Intervention cannot work if it Intervention cannot work if it isn’t usedisn’t used
•Adherence measuresAdherence measures–interventionintervention•pill count, diaries, biologic pill count, diaries, biologic measure, measuring device in measure, measuring device in dispenserdispenser
–visitsvisits–study measurementsstudy measurements

Women’s Health Initiative Women’s Health Initiative
RQRQ: Does calcium plus vitamin D reduce : Does calcium plus vitamin D reduce risk of fractures in postmenopausal risk of fractures in postmenopausal women?women?
DesignDesign: Randomized trial: Randomized trial
Subjects:Subjects: 36,282 PM women enrolled in 36,282 PM women enrolled in WHIWHI
Intervention:Intervention: 1 gm calcium + 400 IU 1 gm calcium + 400 IU vitamin Dvitamin D
OutcomeOutcome: clinical fractures: clinical fractures
Adherence at end of trial 60% and about Adherence at end of trial 60% and about 60% of placebo group was taking calcium60% of placebo group was taking calcium

Follow-upFollow-up
RQRQ: Does diet and exercise reduce risk : Does diet and exercise reduce risk of developing type 2 diabetes in of developing type 2 diabetes in persons with glucose intolerance?persons with glucose intolerance?
DesignDesign: Randomized trial: Randomized trial
Subjects:Subjects: 2500 with glucose intolerance 2500 with glucose intolerance
Intervention:Intervention: low fat weight loss diet low fat weight loss diet and moderate intensity aerobic exerciseand moderate intensity aerobic exercise
MeasurementsMeasurements: Predictor = treatment: Predictor = treatment
outcome = development of frank diabetesoutcome = development of frank diabetes

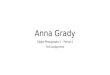
Diet and Exercise to Prevent Diet and Exercise to Prevent Diabetes in Persons with Glucose Diabetes in Persons with Glucose
IntoleranceIntolerance
DMDM No DM No DM
D & ED & E
No D& ENo D& E
6565 560560
125125 500500
625625
625625
10601060190190 12501250
RR = .5; p = .001RR = .5; p = .001

Maximizing Adherence and Follow-Maximizing Adherence and Follow-upup
• Choose subjects likely to adhereChoose subjects likely to adhere– exclude if likely nonadherentexclude if likely nonadherent– complete several visits before randomizationcomplete several visits before randomization– ?complete a run-in?complete a run-in
• Intervention easy and safeIntervention easy and safe
• Visits easy and enjoyableVisits easy and enjoyable– frequent enough to be engagingfrequent enough to be engaging– evening visits, travel and parking evening visits, travel and parking reimbursementreimbursement
– personal relationships with participantspersonal relationships with participants
• Measurements easy, safe and painlessMeasurements easy, safe and painless
• Never discontinue participants Never discontinue participants

Outcomes in Clinical TrialsOutcomes in Clinical Trials
•Efficacy OutcomesEfficacy Outcomes–PrimaryPrimary–SecondarySecondary–SurrogateSurrogate–CompositeComposite
•Adverse EffectsAdverse Effects–rarerare–commoncommon

Raloxifene Use for the HeartRaloxifene Use for the Heart
•Potential OutcomesPotential Outcomes–MortalityMortality–CHD events (death, MI, CHD events (death, MI, ACS)ACS)
–StrokeStroke–Breast cancerBreast cancer–FractureFracture–LDL-cholesterolLDL-cholesterol–Quality of lifeQuality of life

How to Proceed?How to Proceed?
•Measure all outcomesMeasure all outcomes
•Pick one primary outcomePick one primary outcome–estimate sample sizeestimate sample size–FDA requirementFDA requirement
•Make all the rest secondaryMake all the rest secondary

Adverse Events and Side EffectsAdverse Events and Side Effects
• AnticipatedAnticipated– use specific questionsuse specific questions
• UnanticipatedUnanticipated– ask about general adverse ask about general adverse experiencesexperiences
• RareRare– sample size inadequatesample size inadequate
• CommonCommon– multiple differences between multiple differences between groupsgroups

High Quality Randomized TrialsHigh Quality Randomized Trials
•Tamper-proof randomizationTamper-proof randomization
•Blinding of participants, study Blinding of participants, study staff, lab staff, outcome staff, lab staff, outcome ascertainment and adjudicationascertainment and adjudication
•Adherence to study interventionAdherence to study intervention
•Complete follow-upComplete follow-up
•Adequate powerAdequate power