-
8/13/2019 Introduction to Mol Epidemiology
1/60
-
8/13/2019 Introduction to Mol Epidemiology
2/60
Objective
To introduce students to the basic molecular
epidemiological principles and recognize key
features of molecular epidemiological
research
-
8/13/2019 Introduction to Mol Epidemiology
3/60
Contents
1. Introduction
2. Disease and causality
3. Use of biomarkers in epidemiologicalresearch
4. Test validity
5. Measures of association6. Molecular epidemiological study
designs
-
8/13/2019 Introduction to Mol Epidemiology
4/60
Introduction
Epidemiology is taken as the study of the distribution and
determinants of health-related states or events in specified
populations and the application of this study to the control
of
health problems
Populations:
animals
plants
humans etc
Molecular epidemiology entails the incorporation of
molecular, cellular, and other biologic measurements into
epidemiologic research
-
8/13/2019 Introduction to Mol Epidemiology
5/60
-
8/13/2019 Introduction to Mol Epidemiology
6/60
Biologic markers contribute the following opportunities and
capabilities to epidemiologic research
1. Delineation of events between an exposure and disease
2. Identification of exposures to smaller amounts of
xenobiotics& enhanced dose reconstruction
3. Identification of events earlier in the natural history of
clinical
diseases and on a smaller scale
4. Reduction of misclassification of dependent and
independentvariables
5. Indication of mechanisms by which an exposure and a
disease
are related
6. Better understanding of variability and effect modification7.
Enhanced individual and group risk assessment
Collectively these capabilities provide additional tools for
epidemiologist studying etiology, prevention, and control of
disease. Molecular epidemiology is essentially a supplementto
epidemiology
-
8/13/2019 Introduction to Mol Epidemiology
7/60
Traditional epidemiology
Exposure Disease
Molecular epidemiology
Markers of exposure markers of disease
1. Delineation of a continuum of events between
exposure and disease
Exposure
Internal
dose
Biologically
effective
dose
Early
biologic
effect
Altered
structure/
function
Clinical
disease
Prognostic
significance
-
8/13/2019 Introduction to Mol Epidemiology
8/60
2. Identification of smaller amounts of
xenobiotics and enhanced dose reconstruction
Molecular, analytical chemistry and other related tools
allowexposure determinations in the order of 1 part in 1018 or
1021
Molecular epidemiology is able to assess past exposures and
reconstructing doses received from past exposures by using
biologic measurements on samples taken from small groups
of subjects
This procedure is termed biologic dosimetry
Biologic dosimetry complements traditional methods of dose
reconstruction by using personal dosimeters to measure
ambient exposure, by estimating body burdens through
sampling fat, urine, or other materials, or by detecting
adducts, gene mutations, chromosome aberrations, or other
relevant markers
-
8/13/2019 Introduction to Mol Epidemiology
9/60
3. Identification of events earlier in the natural
history
When a continuum or part of a continuum between anexposure and a
disease is identified and understood, it is
possible to focus on preclinical rather than clinical events
Asymptomatic individuals who are at increased risk of
manifesting clinical disease cab be identified Examples of
indicators include decrease in CD4 lymphocytes
in HIV-infected persons; expression of p300 in bladder cells
in
people at risk of bladder cancer, elevated levels of
lipoprotein
Lp(a) in persons at risk for cardiovascular disease and
various
sperm parameters in individuals at risk of reduced fertility
Identification of prodromal events expands the pool of
potential cases for epidemiologic studies and permits
studies of interventions that can have impacts on the study
group as well as entire population
-
8/13/2019 Introduction to Mol Epidemiology
10/60
4. Reduction of misclassification of variables
Misclassification of exposure and disease variables is a
major
weakness of epidemiologic studies
Better classification of exposure than that achieved using
historical characteristics and measurements may be
accomplished by assessing markers of internal and biological
effective doses
More homogeneous disease groupings can be defined using
markers of effect such as specific mutations indicative of
exposure (mutational spectra)
The validity and precision of point estimates may be
increased
as misclassifications are reduced
-
8/13/2019 Introduction to Mol Epidemiology
11/60
5. Indication of mechanisms
Delineating a continuum of events between exposure and
disease provides opportunities for insight into the
mechanisms of action
Much epidemiologic research has been based on theorization
about mechanisms, or at least some prior speculation that
exposure and outcome are related
Molecular epidemiologic approaches facilitate testing the
association between mechanistic events in a defined
continuum
Knowledge about the mechanism can guide future research
and intervention applications
-
8/13/2019 Introduction to Mol Epidemiology
12/60
6. Accounting for variability and effect
modification
Perhaps one of the greatest contributions of
molecularepidemiology is the ability to discern the role of host
factors,
particularly genetic factors, in accounting for variation in
response
Why similarly exposed people do not get the same diseases is
a target question for molecular epidemiology
In most disease systems, susceptibility markers are being
identified and evaluated
These markers can be incorporated into epidemiologic models
as effect modifiers
-
8/13/2019 Introduction to Mol Epidemiology
13/60
7. Enhanced individual and group risk
assessment
Individual risk functions have played a strong role
incardiovascular disease research and control, in pulmonary and
occupational medicine, in infectious disease control, and in
genetic epidemiology and counseling
Molecular epidemiology can enhance individual and group
risk assessments by providing more person-specific
information, allowing extrapolation of risk from one group
to
another, from animal species to humans, and from groups to
individuals
A marker appropriate to both animals and humans that can
be related to exposure-disease relationships in the animal
can
serve as the basis for predicting effects in exposed humans
-
8/13/2019 Introduction to Mol Epidemiology
14/60
Extrapolation from group to group, group to individual, or
individual to group follows the same general model
Identification of a detailed continuum of events between an
exposure and disease, coupled with covariates of the
eventvariables in multivariate models, permits calculation of
individual risk functions (e.g. using serum lipid biomarkers
and
cardiovascular disease risk functions)
Molecular markers can heighten the specificity of thesefunctions
and allow reduced confidence intervals around
estimates
Not only is it now possible to say that a middle-aged man
with
heart disease and a cholesterol level above 240 mg/dl willhave a
one-in-five chance of dying from heart attack in 10
years; it may soon be possible to indicate which individual
will
be
-
8/13/2019 Introduction to Mol Epidemiology
15/60
Epidemiology VS molecular epidemiology
Epidemiology relies on observation and inference of
associations between variables
Molecular and cellular sciences use experimental proof of
cause and effect
Molecular sciences and epidemiology are thus compatible
and linked
Epidemiologists long have used biomarkers (e.g. antibody
titers, serum lipids, blood lead)
However, in the past when high exposures and single
outcomes were more prevalent and frequent, epidemiologists
argued that knowledge of associations was more useful than
understanding the mechanisms, since prevention through
control of exposures was often feasible even in the absence
of
understanding of cellular processes
-
8/13/2019 Introduction to Mol Epidemiology
16/60
Epid. vs molecular epidemiology
Previous success in public health led to the identification
of
the major single or primary causes of diseases
Today, exposures are often smaller and mixed; understanding
mechanisms could be more important in determining
appropriate intervention strategies
The health conditions today are multicausal; to investigate
them requires a wide array of disciplines
Molecular epidemiology is an enhanced capability of
epidemiology to understand disease in terms of the
interaction of environment and heredity
The focus of epidemiology on the other hand is the group
rather than the individual; understanding is gained through
inferences drawn from observations within and among
groups. Causation is inferred rather than proved
-
8/13/2019 Introduction to Mol Epidemiology
17/60
Epid. vs molceular epidemiology
At molecular and cellular level it is possible to make
assessment based on preclinical events such as abnormal DNA
content, or oncogene alteration, once these end points are
established as predictive of clinical disease
Additionally, molecular methods make it possible to
distinguish subtypes of clinical disease that have
potentially
different etiologies
It is therefore plausible to integrate molecular biologic
capabilitiesmeasurements made in individualsinto a
science that uses comparisons of groups to find causes of
disease and opportunities for health protection
-
8/13/2019 Introduction to Mol Epidemiology
18/60
Disease and causality
What is meant by disease?
Alteration of health state and all determinants
Disease is not a random event; the objective of medical
science is to understand how disease is caused so that it
may
be prevented or cured
Epidemiology has contributed to finding causes and remedies
-
8/13/2019 Introduction to Mol Epidemiology
19/60
E.g. Kochs postulates
The germ theory of disease and the growth of knowledge in
microbiology lead to the formulation of a set of
conditions(Kochs postulates) to be satisfied if an organism was to
be
accepted as the cause of a specific disease
1. The microorganism must be found in every case of disease
and not in healthy subjects
2. It must be isolated from the case and grown in the
laboratory
apart from all other organisms
3. It must reproduce the disease when inoculated by itself
into
healthy susceptible individuals
4. The same organism must be found again in these inoculated
individuals and recovered in laboratory cultures
-
8/13/2019 Introduction to Mol Epidemiology
20/60
Kochs postulates said restrictive
From epidemiological perspective, these conditions were
perceived to be too restrictive; not least, because not
alldisease is caused by micro-organisms.
Austen Bradford-Hill suggested a new set of conditions to
indicate whether or a not a particular factor caused a
particular disease:-
1. Strength of associationa strong association is unlikely
to
arise by chance or bias
2. Consistencyrepeated observation of the same association
is different circumstances
3. Specificitya putative cause should lead to a single
effect
4. Temporalitya cause must precede the disease
-
8/13/2019 Introduction to Mol Epidemiology
21/60
5. Biological gradienti.e. a dose-response curve
6. Plausibilitythe suggested cause must be biologically
reasonable
7. Coherencethe suggested cause does not conflict with
existing knowledge of the natural history of the disease
8. Experimental evidencecan support a hypothesized cause
9. Analogye.g. if one drug has teratogenic effects, perhaps
another does as well.
Hill did not suggest that all of these conditions must be
satisfied
to accept that a factor was a cause of a disease; nor that
satisfying any of these necessarily implied a factor was a
cause of a disease (Hill, 1965). Apart from temporality, noneof
these conditions provide a test of causality, although they
are useful as discussion points.
-
8/13/2019 Introduction to Mol Epidemiology
22/60
-
8/13/2019 Introduction to Mol Epidemiology
23/60
Consider possible sufficient causes for a disease
with which you are familiar
Model of disease
Sufficient cause 1: A, B, C, D & E
Sufficient cause 2: A, B, F, G & H
Sufficient cause 3: A, C, F, I & J
A = Necessary cause (e.g. M. bovis)
BCDEFGHIJ = contributory causes
-
8/13/2019 Introduction to Mol Epidemiology
24/60
This simple model permits some importantobservations
In sufficient cause 1, imagine that A, B, C, and D are all
very
common but that component E is rare. By definition, disease
willonly result when E is also present. Since many individuals
arealready exposed to the other four component causes,
theassociation between E and disease will be strong. Although
thisfinding may be important for disease control, this strong
associationneed not be biologically important. In another
population, factor E
might be common and factor C rare, thus altering the strength
ofassociation between factor E and disease without altering
thesufficient cause.
The components of a sufficient cause interact to produce
disease.Thus, it is possible to observe the interaction between
e.g. B and D.However, in the absence of C, disease will not be
produced and the
interaction between B and D will not be observable. When a
newfactor is introduced, it may act to complete a new sufficient
causeas interactions that previously were not apparent
becomeimportant.
-
8/13/2019 Introduction to Mol Epidemiology
25/60
Since the absence of any one of the components of a
sufficientcause will prevent disease, it is not useful to attempt
to proportioncases of disease to individual components. Although no
disease willbe seen in the absence of A, suggesting that 100% of
disease is
attributable to this necessary and component cause, if B and C
areabsent, then no disease will be seen even in the presence of
A.
If it is a assumed that the components of a sufficient cause
actsequentially, then the time to develop the disease will depend
uponwhich of the components is considered. Thus, for example
inreactivation of a latent TB infection, this period would be long
if
measured from infection but short if measured from the stimulus
toreactivation.
This model is very simple and does not allow for chance.
Neitherdoes it allow for dose-response effects. However, these
canarguably be incorporated by creating many sufficient causes,
eachwith different levels of exposure to a particular component.
More
importantly, the model is equally applicable to infectious and
non-infectious disease and provides a conceptual approach for
diseasesof multifactorial and unknown etiology
-
8/13/2019 Introduction to Mol Epidemiology
26/60
Use of biologic markers in epidemiologic
research
Molecular epidemiology is the use of biologic markers orbiologic
measurements in epidemiologic research
Biomarkers include:
Biochemical
Molecular Genetic
Immunologic
Or physiologic signals of events in biologic systems
The events represented can be depicted as part of a continuum
between
initiating event (e.g. exposure to a xenobiotic) and resultant
disease
Each marker represents an event in the continuum (e.g. cigarette
smoking
and lung cancer)
-
8/13/2019 Introduction to Mol Epidemiology
27/60
Use of biomarkers
Molecular epidemiology is an approach to understanding the
origins of disease at the molecular level and to predicting
the
risk that an individual may carry in his or her genome or
the
risk that results from a given toxic or carcinogenic
exposure
It offers the possibility of producing much more specific
estimates of risk, based on a knowledge of events at the
gene
level
The contribution of molecular epidemiology to etiologic
research, risk assessment, or disease prevention and control
depends on the use of valid biomarkers
Validity is the best approximation of the truth or falsehood
of
a marker (need to understand relationship between marker
and event or condition marked)
-
8/13/2019 Introduction to Mol Epidemiology
28/60
-
8/13/2019 Introduction to Mol Epidemiology
29/60
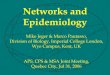
Purpose of a diagnostic test Differentiate between those
individuals that have a particular
condition (e.g. a disease, pregnancy, genetic disorder etc) and
those
that do not. All tested individuals will fall into one of the
followinggroups:
1. Test positive and disease positive (true positive)
2. Test positive and disease negative (false positive)
3. Test negative and disease positive (false negative)
4. Test negative and disease negative (true negative)
The possibilities are summarized:
DISEASE STATUS (TRUE)
+ -
TEST STATUS + a b(marker) - c d
Sensitivity = a/(a+c); specificity = d/(b+d);
Positive predictive value = a/(a+b); Negative PV = d/(c+d)
-
8/13/2019 Introduction to Mol Epidemiology
30/60
-
8/13/2019 Introduction to Mol Epidemiology
31/60
Probably most valuable indicator whether a
marker is valid is the predictive value
Predictive value for a marker of disease is the proportion
of
people studied with a particular disease among all the
people
who have the marker
Predictive value true positives
true positives and false positives
PV can be calculated in terms of those with (positive PV) or
without
(negative PV) a marker
The positive predictive value is defined as the probability that
a test
positive individual is truly positive
The negative predictive value is the probability that a test
negative
individual is truly negative
Validity pertains to predictive value, i.e. that the person who
has a marker
actually experiences the event being indicated
A marker will be valid and useful if it reduces
misclassification, provides
better interpretation of exposure-disease associations, or is
useful inprevention or control of disease
-
8/13/2019 Introduction to Mol Epidemiology
32/60
-
8/13/2019 Introduction to Mol Epidemiology
33/60
What criteria can be used to assess the
usefulness of a method?
Independent comparison with gold standard
Evaluated in a full range of individuals from normal to
severely
affected
Reproducibility and observer variation
How to be used: screening or confirmation
It is cost effective etc
-
8/13/2019 Introduction to Mol Epidemiology
34/60
Criteria for validation and selection of
biomarkers1. Biologic relevance - (exposuredose/response
relationships)
2. Temporal relevancetemporal relationship of markers to
external
exposure or to disease end points must be clear. Timing of
marker
measurement in relation to exposure influences ability to detect
response
3. Understanding noise or background variability and
confounding
variablesvariability is the result of genetic and environmental
factors,
separately and interactingthe natural variability necessitates
knowing
range of biomarker values in a normal population. Since
biologic
markers can be potentially more sensitive than indicators used
in
conventional epidemiologic methods, there is a greater need to
control for
confounding or mitigating factors (age, sex, race, diet, drugs
etc)
Since most biomarkers are nonspecific, i.e. different exposures
may cause
the same marker response, attention should be paid to the impact
of their
use in studies
-
8/13/2019 Introduction to Mol Epidemiology
35/60
4. Reproducibility, sensitivity, specificity, and predictive
value
of assays
Assays should be reproducible with limited variability
The same criteria of adequate sensitivity, specificity, and
predictive value that apply to the validation of screening
methods should be met by biomarkers
Markers of exposure should be sensitive and specific to
toxic
exposures, picking up a high percentage of individuals in
theexposed group and attributing negative results to a high
percentage of unexposed persons
Markers of effect or response should detect a high number of
individuals at elevated risk of adverse outcomes Both types of
markers should give a high proportion of
correct answers
-
8/13/2019 Introduction to Mol Epidemiology
36/60
Measures of association
Epidemiological reasoning is essentially simple. If there is
more disease amongst a group of persons exposed to a
particular factor (a risk factor, disease determinant or
contributory cause) than amongst a similar unexposed group,
then perhaps that exposure is involved in the etiology of
thedisease
By quantifying the association between exposure and disease,
it becomes possible to use statistical methods to judge
whether or not associations arise by chance
-
8/13/2019 Introduction to Mol Epidemiology
37/60
-
8/13/2019 Introduction to Mol Epidemiology
38/60
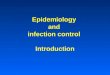
Further;EXPOSURE
+ -
DISEASE + a b- c d
We can also calculate the odds of disease for each group.
Amongst exposed animals, the odds is a/c and amongst
theunexposed animals, the odds is b/d.
The odds can be thought of as an indication of how much likely
asubject is to be diseased than not diseased. Thus, anothermeasure
of epidemiological association is;
odds ratio = (a/c)/(b/d) = (ad)/(bc)
Just as with the risk ratio, if there were no associations
betweenexposure and disease, the odds ratio would be expected to be
1.00and values more extreme than 1.00 indicate association.
-
8/13/2019 Introduction to Mol Epidemiology
39/60
Rate ratio
The final measure of epidemiological association is given by
the rate ratio. Consider the following table;
EXPOSURE
+ -
No. EVENTS a b
Subject TIME AT RISK star1 star0
The incidence rate amongst exposed subjects is IR1=
a/star1and
the incidence rate amongst unexposed subjects is IR0=
b/star0. The rate ratio is IR1/IR0. As with the risk ratio and
the
odds ratio, a rate ratio of 1.00 indicates no association and
arate ratio more extreme than unity indicates an
epidemiological association.
l l d l l d
-
8/13/2019 Introduction to Mol Epidemiology
40/60
Molecular epidemiological study
designs
Molecular epidemiology does not differ in purpose from
epidemiology in general, as molecular epidemiology studies
are based on classic epidemiologic designs
What makes molecular epidemiology distinctive is its ability
to
look inside the black box of exposure-disease continuum
There are a number of study designs that can make use of the
markers
-
8/13/2019 Introduction to Mol Epidemiology
41/60
A. Transitional Studies
Evaluate biomarkers for their optimal use in subsequent
population-based etiologic studies
These studies do not have the capability to directly assess
the
predictive value of a biomarker for developing clinically
apparent disease
They are divided into biomarker development and biomarker
characterization studies
1. Biomarker development studies
Assess the reliability of the assay to be performed on the
specimens and optimize conditions for collecting, processing,and
storing biologic specimen prior to assay
Reproducibility of the laboratory assay
Assay reproducibility should be addressed before the
initiation of a field study
-
8/13/2019 Introduction to Mol Epidemiology
42/60
2. Biomarker characterization studies
Evaluate the distribution and determinants of biomarkers in
populations
Help investigators sift through available markers to select
those that are most promising for use in etiologic studies
From information on behavior and determinants of the
marker, these studies help clarify which etiologic study
designs are optimal for biomarker use
By demonstrating that a xenobiotic compound is absorbed, or
causes an early toxic effect, these investigations may
provide
biologic plausibility for a suspected exposure-disease
association Biomarker characterization studies can be grouped
into cross-
sectional and longitudinal studies
-
8/13/2019 Introduction to Mol Epidemiology
43/60
Cross-sectional studies
A CS examines the relationship between a biomarker and
other variables of interest as they exist in a defined
population at one particular time
The temporal sequence of cause and effect cannot be
determined
They are useful for characterizing the determinants of a
biomarker in a specific population
They can be used to evaluate the correlation between
genotype and phenotypic expression of potential genetic
susceptibility markers
Cross-sectional studies provide limited information onbiomarker
kinetics
-
8/13/2019 Introduction to Mol Epidemiology
44/60
Longitudinal studies
Subsets of a defined population are identified that are,
have
been, or in the future may be exposed, not exposed, or
exposed in different degrees to a factor or factorshypothesized
to influence the biomarker(s) under study
Subjects are evaluated 2 or more times to assess changes in
a
biomarker level due to internal or external perturbations in
the determinants of the biomarker These studies are often
performed when the main exposure
reflected in a biomarker varies over the duration of the
study
period e.g. worker response to occupational exposures
Depending on the kinetics of the biomarker, workers areevaluated
at the beginning and end of work shift, work week,
or vacation period (benzene exposure and peripheral blood
counts)
-
8/13/2019 Introduction to Mol Epidemiology
45/60
Exposure patterns will vary e.g. smoking cessation programs
and decline in 4-aminobiphenyl hemoglobin adduct formation
Longitudinal studies compare individuals to themselves, thus
controlling for genetic differences in effect modification of
theexposure-biomarker response
In short transitional studies lay the foundation for future
etiologic studies
-
8/13/2019 Introduction to Mol Epidemiology
46/60
B. Disease etiology and intervention studies
Use biomarkers to study the determinants of disease in
specific populations and apply this information to the
control
of health problems
Subjects either are healthy at entry into the study and are
followed forward to disease or are diseased at the time of
the
study
They can be used to calculate the biomarker
attributableproportion (AP or etiologic fraction), defined as
the
proportion of diseased cases that is attributable to an
intermediate biomarker
If a marker is causally associated with the disease under
study,this measure provides an assessment of what proportion a
disease would be eliminated if the biomarker determinants
were altered in a way that reduced the marker prevalence in
a
given population
-
8/13/2019 Introduction to Mol Epidemiology
47/60
AP can be determined directly from the sensitivity (s) and
the
relative risk (R)Calculation of attributable proportion
disease
marker yes no
+ A B
- C D
Sensitivity (S) = A/A + c; Relative Risk (R) = [A/(A+B)] /
[C/(C+D]
AP = S(11/R)
-
8/13/2019 Introduction to Mol Epidemiology
48/60
Observational studies
Observational studies using markers include descriptive,
cross-sectional, case-control, and prospective longitudinal
studies
The latter two have the greatest ability to assess etiologic
relationships
1. Case-control CC study starts with the disease (or other
outcome variable)
of interest and a suitable control (comparison, reference)
group of persons without the disease (or outcome variable)
The relationship of an attribute to the disease is examined
bycomparing the diseased and non-diseased with respect to
how frequently the attribute is present or, if the study is
quantitative, the levels of the attribute in each of the
groups
-
8/13/2019 Introduction to Mol Epidemiology
49/60
-
8/13/2019 Introduction to Mol Epidemiology
50/60
2. Longitudinal studies(prospective cohort)
Have potential to use the full range of biomarkers in the
continuum from exposure to disease
They are expensive and time consuming
For any given disease, a study population can be selected
that
is representative of the general population, thus maximizing
the generalizability of the study findings
Alternatively, the study population may be selected to be
initially at high risk for developing the disease (e.g. high
risk
middle-aged men followed for development of coronary
artery disease)
In longitudinal studies repeat sampling and periodic
evaluation is possible over time
I t ti t i l t di
-
8/13/2019 Introduction to Mol Epidemiology
51/60
Intervention trial studies
One of the proposed uses of biomarkers is to assess the
impact of intervention in cohorts at increased risk of
cancer
and heart disease
E.g. in cancer intervention trials, the assumptions are that
the
marker-indicated cancer is likely to occur and that
reduction
of the marker was synonymous with control (reduction) of the
disease Another type of intervention study involves the use of
biologic
markers in the early detection of disease in high risk
groups
The groups can be screened thus providing prevention
modalities in a cost-effective manner
I t t ti f id i l i l
-
8/13/2019 Introduction to Mol Epidemiology
52/60
Interpretation of epidemiological
studies An observed association between an exposure and a
disease
may arise as a consequence of one of four circumstances:
A causal association
Chance
Bias
Confounding
Cause
Criteria for causation: strength of association,
temporality,plausibility, coherence etc
-
8/13/2019 Introduction to Mol Epidemiology
53/60
Chance
All biological features are subject to variation, so an
association may also arise by chance
When we study a random sample from a population, we wish
to infer something about that population
Therefore, we want to know how good an estimate the study
provides of the of the population parameter. The larger the
random sample, the more confident we will be about the
accuracy of the estimate
Hypothesis tests are used to determine the probability that
the result may have arisen by chance. Examples are the
z-test
or t-test for continuous variables and the chi-square test
forcategorical variables
Ch
-
8/13/2019 Introduction to Mol Epidemiology
54/60
Chance
Unless there is overwhelming evidence for an effect in only
one direction, two-tail tests should be used
The tests give a p-value and conventionally, results are
described as statistically significant if the p-value is 0.05
or
less
It is better to quote the p-value for a significance rather
than
simply state that it is significant or not
This value is arbitrary and should not be blindly accepted
would we reject a study result if the p-value were 0.06,
knowing that a slight increase in sample size might have
tipped the result to significance? In a study of 20 risk
factors, one statistically significant result
might arise by chance, so we should ask if the result is
biologically reasonable
-
8/13/2019 Introduction to Mol Epidemiology
55/60
Chance
NB:
The width of a confidence interval is determined by
variation
within the sample and indicates the range within which the
true population value is expected to lie
For measures of association (risk ratio, rate ratio or odds
ratio), if this confidence interval includes 1.0, then the
association is not statistically significant
An association that is statistically significant need not be
biologically or clinically important
The role of chance can be reduced by increasing sample size
Bias
-
8/13/2019 Introduction to Mol Epidemiology
56/60
Bias
Defined as any form of systematic error
In a study, bias may arise as a result of selectionor
observation
Selection bias is particularly important in case:control
studies
Consider how the following sources of data may be biased
with respect to a more general population;
Abattoir
Hospital
Private physician practice
A further source of selection bias may be the proportion
ofpotential participants who do not wish to join a studythe
non-response rate. The impact of a high non-response rate
will be especially marked if it differs between cases and
controls or exposed and unexposed groups
-
8/13/2019 Introduction to Mol Epidemiology
57/60
Confounding
-
8/13/2019 Introduction to Mol Epidemiology
58/60
Confounding
Whilst the role of chance can be controlled by the size of a
random sample and bias by study design, confounding is a
consequence of the complex inter-relationships betweenmultiple
exposures and disease that are found in the real
world
After eliminating the possible roles of bias and chance in
an
observed association, another alternative explanation is thatthe
exposure being studied is actually associated with another
variable, which is directly associated with disease
This other variable would be said to confound the
relationship
between exposure and disease and is often termed aconfounding
variable or a confounder
Common confounding variables include age, sex and breed
Confounding
-
8/13/2019 Introduction to Mol Epidemiology
59/60
Confounding
The confounding variable must be associated with the disease
independently of the exposure of interestif the association
is not independent , then both may lie on the same
causalpathway
Confounding can be controlled by
Random sampling (randomizing subjects)should ensure
that potential confounders are equally distributed in
studygroups
Restriction (restricting subject groups to a narrow range of
potential confoundersonly certain breeds, sex, age of
subjects recruitedbut, if criteria for selection are too
severe,the results may only be applicable to a very limited
population
Matchingcontrols are selected to have the same status with
regard to
confounderse.g. age, sex, breed, parity etc. However,
over-matching can
also result in a reduced ability to generalize in a larger
population
Confounding
-
8/13/2019 Introduction to Mol Epidemiology
60/60
Confounding
Finally, confounding can be controlled in analysis
This may be done either by stratification, in which the
exposure effects are assessed for each level of the
confounding variable, or multivariate analysis
The accessibility of powerful multivariate models such as
logistic regression has facilitated this approach
It requires that information on confounding variables is
collected and then entered into the model
This approach has the advantage over stratification that
many
potential confounders can be controlled simultaneously and
has the advantage over a matched design that the effects ofthese
confounders can be evaluated