Embed Size (px)
Citation preview

1
As a major component of the health caredelivery system, long-term care (LTC) isreceiving increasing attention in both devel-oped and developing countries. LTC is close-ly associated with disabilities emanatingfrom chronic conditions that are mostly re-lated to human aging. Developed countrieshave seen a steep rise in chronic conditions,and the trend will continue. A rise in chron-ic conditions and functional limitations willcreate a growing demand for LTC services inthe developing world as well. Thanks to bet-ter sanitation, nutrition, and medical care,longevity is increasing in developing coun-tries. The social environment in these coun-tries is also changing. Both men and womenare increasingly being drawn into the work-force to improve their standards of living.Their lifestyles are becoming hectic butsedentary.
A broad understanding of long-term careas a distinct segment of the health care de-livery system, LTC clients and services, pol-icy perspectives, and industry perspectives laythe foundation for managing any LTC orga-
nization. The three chapters in this sectionaddress these areas:
• Chapter 1 explains what long-term careis, why it is needed, what type of healthcare and social services constitute LTC,who are the clients served by long-termcare, and how LTC should interface withthe broader health care system.
• Chapter 2 focuses on policy as the dri-ving force behind the evolution of LTCservices. Financing, quality, and access tocommunity-based services have shapedsome of the recent developments. Thefuture remains challenging and requiresa number of policy initiatives to meet thechallenges.
• Chapter 3 furnishes details of the long-term industry, which is necessary for theefficient delivery of services. The chaptercovers community-based and institution-al providers, insurers, LTC professionals,case management agencies, long-termcare pharmacies, and seven categories ofLTC technology.
PART I
Introduction to Long-Term Care
74035_CH01_5368.qxd 8/4/09 9:42 AM Page 1
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION

74035_CH01_5368.qxd 8/4/09 9:42 AM Page 2
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION
3
Chapter 1
Overview of Long-Term Care
What You Will Learn
• Long-term care, as a distinct part of the health care delivery system,is best understood through 10 main dimensions that characterizelong-term care as a set of varied services. The diverse services ful-fill a variety of needs.
• The clients of long-term care are diverse in terms of age and clini-cal needs. The elderly, however, are the major users of long-term careservices.
• Enabling technology reduces the need for long-term care servicesfor many people. But, those who need assistance obtain long-termcare services through three systems of care: informal, communitybased, and institutional.
• Informal care is the largest of the three systems of long-term care.Community-based services have four main objectives and can beclassified into two groups: intramural and extramural. The institu-tional system forms its own continuum of care to accommodateclients whose clinical needs vary from simple to complex.
• Non-long-term care services are often needed by long-term care pa-tients. The long-term care system cannot function without these ser-vices. Hence, the long-term care and non-long-term care systems ofhealth care delivery must be rationally linked.
The Nature of Long-Term CareLong-term care (LTC) is often associatedwith care provided in nursing homes, but thatis a narrow view of LTC. Several types ofnoninstitutional LTC services are providedin a variety of community-based settings.
Family members and surrogates actually pro-vide most of the long-term care that is un-seen to outsiders and often unpaid. Anothercommon misconception is that LTC servicesare meant only for the elderly. Many youngerpeople, and even some children, requireLTC services. The elderly, however, are the
74035_CH01_5368.qxd 8/4/09 9:42 AM Page 3
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION

predominant users of these services, and mostLTC services have been designed with theelderly client in mind.
There is no simple definition that canfully capture the nature of long-term care.This is because a broad range of clients andservices are involved. Yet, certain character-istics are common to all LTC services, re-gardless of whether they are delivered in aninstitution or in a community-based setting.
Long-term care can be defined as a va-riety of individualized and well-coordinatedtotal care services that promote the maxi-mum possible independence for people withfunctional limitations and that are providedover an extended period of time, using ap-propriate current technology and availableevidence-based practices, in accordance witha holistic approach while maximizing boththe quality of clinical care and the individ-ual’s quality of life. This comprehensive de-finition emphasizes 10 essential dimensions,which apply to both institutional and nonin-stitutional long-term care. An ideal LTC sys-tem will incorporate these 10 characteristics.
1. Variety of services.
2. Individualized services.
3. Well-coordinated total care.
4. Promotion of functional indepen-dence.
5. Extended period of care.
6. Use of current technology.
7. Use of evidence-based practices.
8. Holistic approach.
9. Maximizing quality of care.
10. Maximizing quality of life.
Variety of ServicesThe delivery of most types of medical ser-vices is based on what is called the medical
model, according to which health is viewedas the absence of disease. When a patient suf-fers from some disorder, clinical interven-tions that are widely accepted by the medicalprofession are used to relieve the patient’ssymptoms. Prevention of disease and pro-motion of optimum health are relegated to asecondary status. By contrast, in long-termcare, medical interventions are only a part ofan individual’s overall care. Emphasis is alsoplaced on nonmedical factors such as socialsupport and residential services.
Long-term care encompasses a varietyof services for three main reasons: (1) to fitthe needs of different individuals, (2) to ad-dress changing needs over time, and (3) to suitpeople’s personal preferences. Needs varygreatly from one individual to another. Eventhe elderly, who are the predominant usersof LTC services, are not a homogeneousgroup. For example, some people just requiresupportive housing, whereas others requireintensive treatments. The type of services anindividual requires is determined by the na-ture and degree of his or her functional dis-ability and the presence of any other medicalconditions and emotional needs that the in-dividual may have.
Even for the same individual, the needfor the various types of services generallychanges over time. The change is not neces-sarily progressive, from lighter to more in-tensive levels of care. Depending on thechange in condition and functioning, the in-dividual may shift back and forth among thevarious levels and types of LTC services. Forexample, after hip surgery, a patient may re-quire extensive rehabilitation therapy in anursing facility for two or three weeks be-fore returning home, where he or she receivescontinuing care from a home health careagency. After that, the individual may contin-ue to live independently but require a daily
4 CHAPTER 1 • Overview of Long-Term Care
74035_CH01_5368.qxd 8/4/09 9:42 AM Page 4
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION

meal from Meals On Wheels, a home-deliv-ered meals service. Later, this same personmay suffer a stroke and, after hospitalization,have to stay indefinitely in a LTC facility.Hospice care may become necessary at theend of a person’s life.
People’s personal preferences also play arole in the determination of where servicesare received. Experts generally agree that, tothe extent possible, people should be able tolive and receive services where they want. Al-most always, people prefer to live in the com-munity, the first choice being their own home.Home- and community-based services haveincreasingly become available so that peoplecan age in the community. Severe declinesin health, however, may necessitate institu-tional services, particularly for people whoneed care around the clock. Again, a varietyof long-term care facilities are now available.
LTC services are an amalgam of fivedistinct types of services:
• Medical care.
• Mental health services.
• Social support.
• Residential amenities.
• Hospice services.
Understanding the distinctive features ofthese services is important. In actual practice,however, they should be appropriately inte-grated into the total package of care in ac-cordance with individual needs.
Medical CareMedical interventions in long-term care areprimarily governed by the presence of twomain health conditions that are closely relat-ed: chronic illness and comorbidity. First, asopposed to the care for acute conditions, LTC
focuses on chronic ailments, particularlywhen they have already caused some physicalor mental dysfunction. Acute conditions areepisodic; require short-term but intensive med-ical interventions; generally respond to med-ical treatment; and are treated in hospitals,emergency departments, or outpatient clini-cal settings. Chronic conditions, on the oth-er hand, persist over time and are generallyirreversible, but must be kept under control. Ifnot controlled, serious complications can de-velop. In order of their prevalence among theaged population, the most common chronicconditions are hypertension, arthritis, heartdisease, cancers, and diabetes (Federal Inter-agency Forum, 2004). The mere presence ofchronic conditions, however, does not indi-cate a need for long-term care. When chron-ic conditions are compounded by the presenceof comorbidity—coexisting multiple healthproblems—they often become the leadingcause of an individual’s disability and erodethat individual’s ability to live without assis-tance. This is when LTC is needed. The preva-lence of comorbidity and disability risedramatically in aging populations.
Medical care in the LTC environmentgenerally focuses on three main areas:
1. Continuity of care after treatment ofacute episodes in hospitals.
2. Clinical management of chronic con-ditions and prevention of potentialcomplications.
3. Hospitalization when necessary.
Continuity of Care after HospitalizationLong-term care generally involves continuityof care after discharge from a hospital. Pa-tients are hospitalized for acute episodes.Post-acute LTC often consists of skilled nurs-ing care, which is physician-directed care
The Nature of Long-Term Care 5
74035_CH01_5368.qxd 8/4/09 9:42 AM Page 5
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION

provided by licensed nurses and therapists.Post-acute care may be provided in a patient’sown home through home health care, or in aLTC facility. Home health care brings ser-vices such as nursing care and rehabilitationtherapies to patients in their own homes be-cause such patients do not need to be in aninstitution and yet are generally unable toleave their homes safely to get the care theyneed. A long-term care facility is an institu-tion, commonly referred to as a nursing home,that is duly licensed to provide long-termcare services.
Clinical Management and PreventionBecause chronic conditions cannot be cured,they must be managed. Left unmanaged,chronic conditions often lead to severemedical complications over time. For exam-ple, untreated diabetes can lead to heart prob-lems, nerve damage, blindness, and kidneyfailure. The onset of complications arisingfrom chronic conditions can be prevented orpostponed through preventive medicine thatincludes adequate nutrition, therapeutic diets,hydration (fluid intake), ambulation (movingabout), vaccination against pneumonia and in-fluenza, and well-coordinated primary careservices. Ongoing monitoring and timely in-terventions are generally necessary.
Hospitalization when NecessaryOnset of an acute episode requires medicalevaluation and treatment in a hospital. Pa-tients in LTC settings may encounter acuteepisodes, such as pneumonia, bone fracture,or stroke, and require admission to a gener-al hospital. For the same medical conditions,the elderly are more prone to be hospitalizedcompared with people in younger age groupswho may be treated as outpatients.
Mental Health ServicesLong-term care patients frequently sufferfrom mental conditions, most notably depres-sion, anxiety disorders, delirium, and demen-tia. Approximately two-thirds of nursinghome residents suffer from mental disorders(Burns et al., 1993). Mental disorders rangein severity from problematic, to disabling, tofatal. Research shows that depression, al-though common in nursing homes and as-sisted living facilities, often goes undetected(Smalbrugge et al., 2006; Watson et al.,2006). Under-diagnosis and under-treatmentof depression is also a serious problem amongcommunity-dwelling older adults. The risk ofdepression in the elderly increases with oth-er illnesses and when ability to function be-comes limited (NIMH, 2007). Dementia isanother common mental disorder. Character-ized by memory loss, patients with demen-tia find it difficult to do things that they usedto do with ease. Patients with dementia arealso likely to become aggressive and undergomood changes.
It is erroneous to believe that mental dis-orders are normal in older people or that old-er people cannot change or improve theirmental health. But major barriers must beovercome in the delivery of mental healthcare. Efforts to prevent mental disordersamong older adults have been inadequate be-cause present knowledge about effective pre-vention techniques is not as extensive as ourunderstanding of the diagnosis and treatmentof physical disorders. On the other hand,treatment of many elderly people may be in-adequate because assessment and diagnosisof mental disorders in older people can be par-ticularly difficult: the elderly often focus onphysical ailments rather than psychologicalproblems (DHHS, 1999). Another drawbackis that many elder care providers, including
6 CHAPTER 1 • Overview of Long-Term Care
74035_CH01_5368.qxd 8/4/09 9:42 AM Page 6
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION

primary care physicians, are often not ade-quately trained in the diagnosis and treatmentof mental health problems.
Mental health services are generally de-livered by specialized providers in both out-patient and inpatient facilities. Because LTCfacilities are responsible for a patient’s totalcare, nursing home employees must be trainedto recognize the need for mental health care,and the facility must arrange to obtain need-ed services from qualified providers in thecommunity.
Social SupportSocial support refers to a variety of assistiveand counseling services to help people copewith situations that may cause stress, conflict,grief, or other emotional imbalances. Thegoal is to help people make adjustments tochanging life events.
Various stressors commonly accompa-ny the aging process itself and create suchadverse effects as frailty, pain, increasedmedical needs, and the inability to do com-mon things for oneself, such as obtainingneeded information or running errands.Other stressors are event driven. Events thatforce an unexpected change in a person’slifestyle or emotional balance—such asmoving to an institution, loss of a loved one,or experiencing social conflict—requirecoping with stress or grief. Even the thoughtof change brings on anxiety. Many peoplego through a period of “grieving” whencoming to terms with change, which is anormal part of the transition process. Griev-ing may manifest in reactions such as anger,denial, confusion, fear, despondency, anddepression (McLeod, 2002). Social supportis needed to help buffer these adverse ef-fects (Feld & George, 1994; Krause & Bo-rawski-Clark, 1994).
Social support includes both concreteand emotional assistance provided by fam-ilies, friends, neighbors, volunteers, staffmembers within an institution, organiza-tions such as religious establishments andsenior centers, or other private or publicprofessional agencies. Such assistance mayalso include coordination of simple logisti-cal problems that may otherwise become“hassles” of daily life, providing informa-tion, giving reminders, counseling, and of-fering spiritual guidance. Simply remainingconnected with the outside world is an im-portant aspect of social support for manypeople.
Residential AmenitiesSupportive housing is a key component ofLTC because certain functional and safetyfeatures must be carefully planned to com-pensate for people’s disabilities to the maxi-mum extent possible in order to promoteindependence. Some simple examples in-clude access ramps that enable people to gooutdoors, wide doorways and corridors thatallow adequate room to navigate wheel-chairs, railings in hallways to promote inde-pendent mobility, extra-large bathrooms thatfacilitate wheelchair negotiation, grab bars inbathrooms to prevent falls and promoteunassisted toileting, raised toilets to make iteasier to sit down and get up, and pull-cordsin the living quarters to summon help in caseof an emergency.
Congregate housing—multi-unit housingwith support services—is an option for se-niors and disabled adults. Support servicesare basic assistive services. They may includemeals, transportation, housekeeping, buildingsecurity, social activities, and outings. How-ever, not all housing arrangements provideall of these services.
The Nature of Long-Term Care 7
74035_CH01_5368.qxd 8/4/09 9:42 AM Page 7
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION

In LTC institutions, adequate space, pri-vacy, safety, comfort, and cleanliness arebasic residential amenities. In addition, theinstitutional environment must feel home like,it must encourage social activities, it mustpromote recreational pursuits, and the décormust be both pleasing and therapeutic.
Hospice ServicesHospice services, also called end-of-life care,are regarded as a component of long-termcare. The focus of hospice, however, differsconsiderably from other LTC services. Hos-pice incorporates a cluster of special servicesfor the terminally ill with a life expectancy ofsix months or less. It blends medical, spiritu-al, legal, financial, and family support ser-vices. However, the emphasis is on comfort,palliative care, and social support over med-ical treatment. Palliation refers to medicalcare that is focused on relieving unpleasantsymptoms such as pain, discomfort, andnausea.
The hospice philosophy also regards thepatient and family together as one unit ofcare. The option to use hospice means thattemporary measures to prolong life will besuspended. The emphasis is on maintainingthe quality of life and letting the patient diewith dignity. Psychological services focuson relieving mental anguish. Social and le-gal services help with arranging final af-fairs. Counseling and spiritual support areprovided to help the patient deal with his orher death. After the patient’s death, bereave-ment counseling is offered to the family orsurrogates.
The services are generally brought to thepatient, although a patient may choose to goto a freestanding hospice center if one isavailable. Hospice care can be directed from
a hospital, home health agency, nursing home,or freestanding hospice.
Individualized ServicesLong-term care services are tailored to theneeds of the individual patient. Those needsare determined by an assessment of the in-dividual’s current physical, mental, and emo-tional condition. Other factors used for thispurpose include past history of the patient’smedical and psychosocial conditions; a so-cial history of family relationships, formeroccupation, community involvement, andleisure activities; and cultural factors such asracial or ethnic background, language, andreligion. An individualized plan of care is de-veloped so that each type of need can be ap-propriately addressed through customizedinterventions.
Well-Coordinated Total CareLong-term care providers are responsiblefor managing the total health care needs ofan individual client. Total care means thatany health care need is recognized, evaluat-ed, and addressed by appropriate clinical pro-fessionals. Coordination of care with variousmedical providers such as the attending physi-cians, dentists, optometrists, podiatrists, der-matologists, or audiologists is often necessaryto prevent complications or to deal with theonset of impairments at an early stage. Theneed for total care coordination can alsobe triggered by changes in basic needs or oc-currence of episodes. Transfer to an acute carehospital or treatment for mental or behav-ioral disorders may become necessary. Hence,long-term care must interface with non-LTCservices.
8 CHAPTER 1 • Overview of Long-Term Care
74035_CH01_5368.qxd 8/4/09 9:42 AM Page 8
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION

Promotion of Functional IndependenceLTC becomes necessary when there is a re-markable decline in an individual’s ability toindependently perform certain common tasksof daily living. Among children, disabilitiescan result from birth defects, brain damage,or mental retardation. Younger adults maylose functional capacity as a result of an ac-cident or a crippling disease such as multiplesclerosis.
The goal of LTC is to enable the individ-ual to maintain functional independence tothe maximum level practicable. Restorationof function may be possible to some extentthrough appropriate rehabilitation therapy,but, in most cases, a full restoration of nor-mal function is an unrealistic expectation.The individual must be taught to use adap-tive equipment such as wheelchairs, walkers,special eating utensils, or portable oxygendevices. Staff members must render care andassistance whenever the patient is either un-able to do things for him- or herself or ab-solutely refuses to do so.
In keeping with the goal of maximizingfunctional independence for the patient, nurs-ing home staff members should concentrateon maintaining whatever ability to functionthe patient still has and on preventing furtherdecline of that ability. For example, a patientmay be unable to walk independently but maybe able to take a few steps with the help oftrained staff members. Assistance with mo-bility helps maintain residual functioning.Progressive functional decline may be slowedby appropriate assistance and ongoing main-tenance therapy, such as assisted walking,range of motion exercises, bowel and bladdertraining, and cognitive reality orientation.However, in spite of these efforts, it is rea-sonable to expect a gradual decline in an in-
dividual’s functional ability over time. As thishappens, services must be modified in ac-cordance with the changing condition. In oth-er words, LTC must “fill-in” for all functionsthat can no longer be carried out indepen-dently. For instance, a comatose patient whois totally confined to bed presents an extremecase in which full assistance from employeesis required. In most other instances, staffmembers motivate and help the patient do asmuch as possible for him- or herself.
Extended Period of CareFor most LTC patients, the delivery of vari-ous services extends over a relatively longperiod because most recipients of care willat least require ongoing monitoring to noteany deterioration in their health and to ad-dress any emerging needs. Certain types ofservices—such as professional rehabilita-tion therapies, post-acute convalescence, orstabilization—may be needed for a relative-ly short duration, generally less than 90 days.In other instances, LTC may be needed foryears, perhaps indefinitely. In either situa-tion, the period during which care is given ismuch longer than it is for acute care services,which generally last only for a few days. Be-cause patients stay in nursing care facilitiesover an extended time, holistic care and qual-ity of life (discussed later) must be integrat-ed into every aspect of LTC delivery.
Use of Current TechnologyUse of technology varies according to thetype of LTC setting. Certain types of safetytechnologies, such as nonslip footwear andhip protectors that protect the hip from in-jury during a fall, can be used in almost all
The Nature of Long-Term Care 9
74035_CH01_5368.qxd 8/4/09 9:42 AM Page 9
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION

settings. Other technologies, such as call sys-tems to summon assistance, bathing systems,and wander management systems, are de-signed for specific applications. Chapter 3covers LTC technology in greater detail.
Use of Evidence-Based PracticesEvidence-based care relies on the use ofbest practices that have been establishedthrough clinical research. Increasingly, clin-ical processes that have been proven toprovide improved therapies are being stan-dardized into clinical practice guidelines.These guidelines become evidence-basedstandardized protocols that are indicated forthe treatment of specific health conditions.They have been developed to assist practi-tioners in delivering appropriate health carefor specific clinical circumstances. An in-creasing number of standard guidelines havebeen developed for use in nursing homes.Some of these same guidelines can also beused in other LTC settings such as homehealth and assisted living.
Holistic ApproachIn sharp contrast to the medical model, theholistic model of health proposes that healthcare delivery should focus not merely on aperson’s physical and mental needs, butshould also emphasize well-being in everyaspect of what makes a person whole andcomplete. In this integrated model, a patient’smental, social, and spiritual needs and pref-erences should be incorporated into medicalcare delivery and all aspects of daily living.
By its very nature, effective LTC is holis-tic. Once the need for LTC has been estab-lished, a holistic approach must be used inthe delivery of care. The following are brief
descriptions of the four aspects of holisticcaregiving:
1. Physical. This refers to the technicalaspects of care, such as medical ex-amination, nursing care, medications,diet, rehabilitation treatments, etc. Italso includes comfort factors such asappropriate temperature and cozy fur-nishings, cleanliness, and safety inhome and institutional environments.
2. Mental. The emphasis is on the totalmental and emotional well-being ofeach individual. It may include treat-ment of mental and behavioral prob-lems when necessary.
3. Social. Almost everyone enjoys warmfriendships and social relationships.Visits from family, friends, or volun-teers provide numerous opportunitiesfor socializing. The social aspects ofhealth care include housing, trans-portation services, information, coun-seling, and recreation.
4. Spiritual. The spiritual dimensionoperates at an individual level. Itincludes personal beliefs, values, andcommitments in a religious and faithcontext. Spirituality and spiritual pur-suits are very personal matters, but formost people they also require contin-uing interaction with other membersof the faith community.
Maximizing Quality of CareQuality of care is maximized when desirableclinical- and satisfaction-related outcomeshave been achieved. Maximization of quali-ty is an ongoing pursuit, and is never fullyachieved. Hence, maximizing quality requiresa culture of continuous improvement. It re-
10 CHAPTER 1 • Overview of Long-Term Care
74035_CH01_5368.qxd 8/4/09 9:42 AM Page 10
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION
quires a focus on the other nine dimensionsencompassing the nature of LTC discussedin this section. It requires emphasis on bothclinical and interpersonal aspects of care-giving. To improve quality, standards such asregulatory standards and evidence-basedclinical practice guidelines must be imple-mented. Quality must be evaluated or mea-sured to discover areas needing improvement,and processes should be changed as neces-sary. This becomes an ongoing effort.
Maximizing Quality of LifeQuality of life refers to the total living expe-rience, which results in overall satisfactionwith one’s life. Technology that enables peo-ple to live independently generally enhancesthe quality of life. Quality of life is a multi-faceted concept that recognizes at least fivefactors: lifestyle pursuits, living environ-ment, clinical palliation, human factors, andpersonal choices. Quality of life can be en-hanced by integrating these five factors intothe delivery of care.
1. Lifestyle factors are associated withpersonal enrichment and makingone’s life meaningful through activ-ities one enjoys. For example, almosteveryone enjoys warm friendships andsocial relationships. Elderly people’sfaces often light up when they see chil-dren. Many residents in institutionalsettings may still enjoy pursuingtheir former leisure activities, such aswoodworking, crocheting, knitting,gardening, and fishing. Many resi-dents would like to engage in spiritu-al pursuits or spend some time alone.Even patients whose functioning hasdecreased to a vegetative or comatosestate can be creatively engaged in
something that promotes sensoryawakening through visual, auditory,and tactile stimulation.
2. The living environment must be com-fortable, safe, and appealing to thesenses. Cleanliness, décor, furnish-ings, and other aesthetic features arecritical.
3. Palliation should be available for re-lief from unpleasant symptoms suchas pain or nausea.
4. Human factors refer to caregiver atti-tudes and practices that emphasizecaring, compassion, and preservationof human dignity in the delivery ofcare. Institutionalized patients gener-ally find it disconcerting to have losttheir autonomy and independence.Quality of life is enhanced when res-idents have some latitude to governtheir own lives. Residents also desirean environment that promotes privacy.For example, one field study of nurs-ing home residents found that digni-ty and privacy issues were foremostin residents’ minds, overshadowingconcerns for clinical quality (HealthCare Financing Administration, 1996).
5. As pointed out earlier, people over-whelmingly choose to be independent.However, even institutions shouldmake every effort to accommodatepatients’ personal choices. For exam-ple, food is often the primary area ofdiscontentment, which can be ad-dressed by offering a selective menu.Many elderly resent being awakenedearly in the morning when nursinghome staff begin their responsibilitiesto care for patients’ hygiene, bathing,and grooming. Patient privacy is com-promised when a facility can offer
The Nature of Long-Term Care 11
74035_CH01_5368.qxd 8/4/09 9:42 AM Page 11
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION

only semi-private accommodations.But, in that case, the facility can at leastgive the patients some choice in decid-ing who their roommates would be.
Clients of Long-Term CareMore than 10 million Americans are estimat-ed to need LTC services. The majority (58%)are elderly, but a significant proportion (42%)are under the age of 65. Among those whoneed LTC, 14% are in nursing homes and86% reside in the community (Kaiser, 2007).
LTC clients can be classified into fivemain categories:
1. Older adults.
2. Children and adolescents.
3. Young adults.
4. People with HIV/AIDS.
5. People needing subacute or high-techcare.
Older AdultsThe elderly, people 65 years of age or older,are the primary clients of long-term care.Most of the elderly, however, are in goodhealth. According to household interviewsof the elderly civilian noninstitutionalizedpopulation, only 25% described their healthas fair or poor (DHHS, 2008a). It is reason-able to assume that the segment of the elderlypopulation in fair-to-poor overall health islikely to require LTC at some point. Even forthose in good or excellent health, short-termLTC (needed for 90 days or less) may becomenecessary after an accident, surgery, or acuteillness. Also, important differences in healthexist according to population characteristics.Those in fair or poor health are more likely
to be black, Hispanic, or American Indianrather than white or Asian; financially pooror near poor; and rural rather than urbanresidents.
A person’s age, or the presence of chron-ic conditions, by itself does not predict theneed for long-term care. However, as a per-son ages, chronic ailments, comorbidity, dis-ability, and dependency tend to follow eachother. This progression is associated with in-creased probability that a person would needlong-term care (Figure 1–1). In 2007, ap-proximately 7% of civilian, noninstitution-alized elderly in the United States neededhelp with personal care from other individu-als (DHHS, 2008b).
Disability is commonly assessed interms of a person’s ability to perform certainkey everyday activities. Although chronicmental impairments are often assumed toeventually manifest in physical dysfunction,that is not always the case. Individuals withcertain chronic mental illnesses may be ableto perform most everyday activities but mayrequire supervision and monitoring. Severedementias, on the other hand, which aremostly confined to older people, are com-monly accompanied by physical functionallimitations.
Two standard measures are available todetermine a person’s level of dependency. Thefirst, the activities of daily living (ADL) scale,is used to determine whether an individualneeds assistance in performing six basic ac-tivities: eating, bathing, dressing, using thetoilet, maintaining continence, and trans-ferring into or out of a bed or chair. Groom-ing and walking a distance of eight feet aresometimes added to evaluate self-care andmobility. The ADL scale is the most relevantmeasure for determining the need for assis-tance in a long-term care facility. Therefore,ADLs are a key input in determining a facil-
12 CHAPTER 1 • Overview of Long-Term Care
74035_CH01_5368.qxd 8/4/09 9:42 AM Page 12
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION
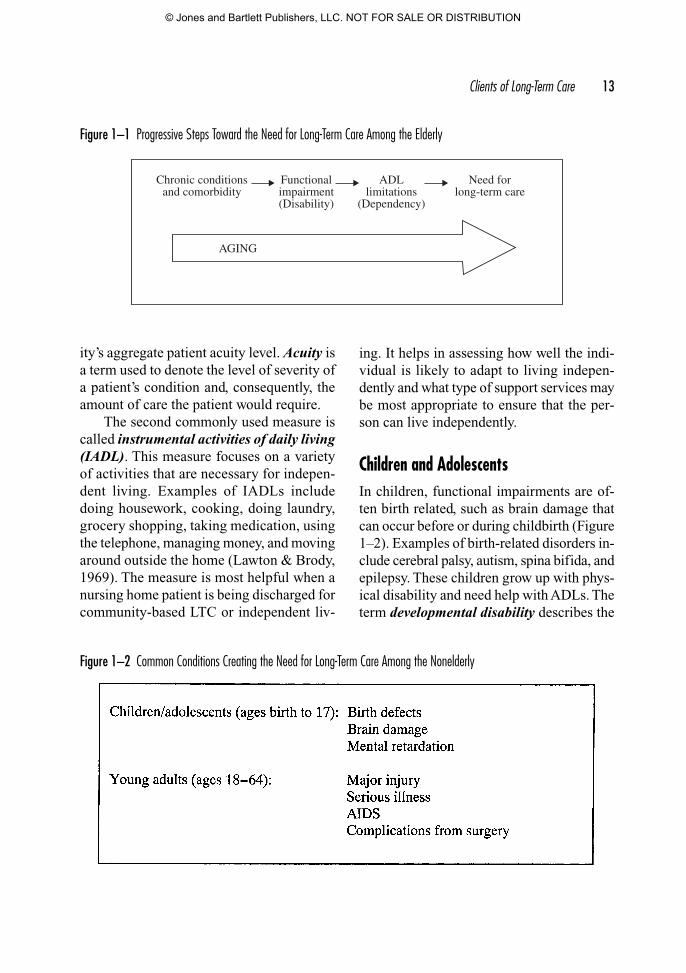
ity’s aggregate patient acuity level. Acuity isa term used to denote the level of severity ofa patient’s condition and, consequently, theamount of care the patient would require.
The second commonly used measure iscalled instrumental activities of daily living(IADL). This measure focuses on a varietyof activities that are necessary for indepen-dent living. Examples of IADLs includedoing housework, cooking, doing laundry,grocery shopping, taking medication, usingthe telephone, managing money, and movingaround outside the home (Lawton & Brody,1969). The measure is most helpful when anursing home patient is being discharged forcommunity-based LTC or independent liv-
ing. It helps in assessing how well the indi-vidual is likely to adapt to living indepen-dently and what type of support services maybe most appropriate to ensure that the per-son can live independently.
Children and AdolescentsIn children, functional impairments are of-ten birth related, such as brain damage thatcan occur before or during childbirth (Figure1–2). Examples of birth-related disorders in-clude cerebral palsy, autism, spina bifida, andepilepsy. These children grow up with phys-ical disability and need help with ADLs. Theterm developmental disability describes the
Clients of Long-Term Care 13
Chronic conditionsand comorbidity
Functionalimpairment(Disability)
Need forlong-term care
ADLlimitations
(Dependency)
AGING
Figure 1–1 Progressive Steps Toward the Need for Long-Term Care Among the Elderly
Figure 1–2 Common Conditions Creating the Need for Long-Term Care Among the Nonelderly
74035_CH01_5368.qxd 8/4/09 9:42 AM Page 13
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION

general physical incapacity such childrenmay face at a very early age. Those who ac-quire such dysfunctions are referred to as de-velopmentally disabled, or DD for short.Mental retardation, that is, below-averageintellectual functioning, also leads to devel-opmental disability in most cases. The closeassociation between the two is reflected inthe term MR/DD, which is short for mental-ly retarded/developmentally disabled. Thus,some children and adolescents can have theneed for LTC services that are generally avail-able in special pediatric long-term care andMR/DD facilities.
Young AdultsPermanent disability among young adultscommonly stems from neurological malfunc-tions, degenerative conditions, traumatic in-jury, or surgical complications. For example,multiple sclerosis is potentially the most com-mon cause of neurological disability in youngadults (Compston & Coles, 2002). Severeinjury to the head, spinal cord, or limbs canoccur in victims of vehicle crashes, sportsmishaps, or industrial accidents. Other seri-ous diseases, injuries, and respiratory or heartproblems following surgery can make it dif-ficult, or even impossible, for a patient tobreathe naturally. Such individuals, who can-not breathe (or ventilate) on their own, requirea ventilator. A ventilator is a small machinethat takes over the breathing function by au-tomatically moving air into and out of the pa-tient’s lungs. Ventilator-dependent patientsalso require total assistance with their ADLs.
Many MR/DD victims are entering adult-hood. The aging process begins earlier inpeople with mental retardation, and the ageof 50 has been suggested to demarcate theelderly segment in this population (Altman,1995). An increasing number of people with
MR/DD are now living beyond the age of 50.Hence, this population will manifest not onlysevere mental and physical impairments butalso the effects of chronic conditions andcomorbidity.
Evidence suggests that MR/DD patientsmay function better in community-based res-idential settings than in traditional nursinghomes. Studies of patients who had movedout of nursing homes to community settingsdemonstrated that these patients had higherlevels of adaptive behavior, lifestyle satisfac-tion, and community integration than resi-dents who remained in nursing homes (Helleret al., 1998; Spreat et al., 1998). Opportunityto make choices, small facility size, attractivephysical environment, and family involve-ment were associated with higher levels ofadaptive behavior and community integration(Heller et al., 1999; Heller et al., 2002).
People with HIV/AIDSWhen it first gained national attention in theearly 1980s, AIDS was a fatal disease thatresulted in a relatively painful death shortlyafter HIV infection. Since then, the intro-duction of protease inhibitors, antiretroviraltherapy, and antibiotics for the treatment ofAIDS-related infections has vastly improvedthe health condition of HIV/AIDS patients.Consequently, AIDS has evolved from anend-stage terminal illness into a chronic con-dition. With reduced mortality, the prevalenceof HIV in the population has actually in-creased, including among the elderly.
Over a period of time, people with AIDSare subject to a number of debilitating con-ditions, which create the need for assistance.Hence, the demand for LTC services is in-creasing, particularly because at least 25%of all known people with HIV/AIDS are age50 and older (New York City Department of
14 CHAPTER 1 • Overview of Long-Term Care
74035_CH01_5368.qxd 8/4/09 9:42 AM Page 14
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION

Health and Mental Hygiene, 2004) and mor-tality rates from HIV/AIDS have decreased.
Care of HIV/AIDS patients presentsspecial challenges, especially because thispopulation has characteristics that are quitedissimilar to the rest of the LTC population.HIV/AIDS patients have a significantly high-er prevalence of depression, other psychi-atric disorders, and dementia associated withAIDS. HIV/AIDS patients also have a sig-nificantly higher prevalence of weight lossand incontinence of bladder and bowel (Shinet al., 2002).
People Requiring Subacute or High-Tech CareA growing number of nursing facilities havedeveloped subacute and technology-intensiveservices. The term subacute care applies topost-acute services for people who requireconvalescence from acute illnesses or surgi-cal episodes. These patients may be recover-ing but are still subject to complications whilein recovery. They require more nursing in-tervention than what is typically included inskilled nursing care. The patients are trans-ferred from the hospital to a nursing homeafter the acute condition has been treated, orafter surgery. Some common orthopedicepisodes include hip and knee replacement.Other subacute and high-tech services areneeded for patients who require ventilatorcare, head trauma victims, comatose patients,and those with progressive Alzheimer’sdisease.
The Long-Term Care Delivery SystemThe LTC system is sometimes referred toas the continuum of long-term care, whichmeans the full range of long-term care ser-
vices that increase in the level of acuity andcomplexity from one end to the other—frominformal and community-based services atone end of the continuum to the institution-al system at the other end.
The long-term care delivery system hasthree major components:
• The informal system.
• The community-based system.
• The institutional system.
The first component, informal care, is thelargest, but it generally goes unrecognized.For the most part, it is not financed by in-surance and public programs, but it includesprivate-duty nursing arrangements betweenprivate individuals. The other two compo-nents have formalized payment mechanismsto pay for services, but payment is not avail-able for every type of community-based andinstitutional service. In many situations, peo-ple receiving these services must pay for themout of their personal resources.
Although institutional management isthe focus of this book, the other two compo-nents, informal care and community-basedservice, also have important implications foradministrators who manage LTC institutions.The community-based services and informalsystems compete with the institutional systemin some ways, but are also complementary.
The three subsystems that form the LTCcontinuum are illustrated in Figure 1–3. Thepatients’ levels of acuity and the complexityof services they need increase from one endof the continuum to the other, for the mostpart. Informal care provided mainly by fam-ily members or friends involves basic assis-tance and is at one extreme of the continuum.Next on the continuum are the variouscommunity-based in-home services and
The Long-Term Care Delivery System 15
74035_CH01_5368.qxd 8/4/09 9:42 AM Page 15
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION

ambulatory services. Finally, there are dif-ferent levels of institutional settings.
Given the complexity of the LTC system,case management (also called care manage-ment) fills in a key role. Case management isa centralized coordinating function in whichthe special needs of older adults are identi-fied and a trained professional determineswhich services would be most appropriate,determines eligibility for those services,makes referrals, arranges for financing, andcoordinates and monitors delivery of care toensure that clients are receiving the prescribedservices. Case management helps link, man-age, and coordinate services to meet the var-ied and changing health care needs of elderlyclients. Case management provides a singleentry point for obtaining information aboutand accessing services. The extent of disabil-ity and personal needs primarily determine
which services on the continuum may be bestsuited for an individual. However, client pref-erences, availability of community-based ser-vices, and ability to pay for services also playa significant role.
In recent years, numerous public andprivate health care organizations haveproliferated—organizations that offer in-formation to consumers on how to care forsomeone at home, how to find and pay forcommunity-based services, and how to findan appropriate institutional setting.
The Informal SystemThe informal long-term care system is verylarge. An accurate estimate of its size is dif-ficult, mainly because the system is not for-mally organized and it cannot even be calleda system in the true sense. However, there
16 CHAPTER 1 • Overview of Long-Term Care
The Community-based System of Long-Term Care
The Institutional System of Long-Term Care
The Informal System In-Home Services Ambulatory Services Inpatient Services
Info
rmal
care
Hom
e-de
liver
ed m
eals
Hom
e hea
lth ca
re
Hom
e hea
lth h
ospi
ce
Hea
lth ed
ucat
ion
and
scre
enin
g
Congr
egat
e mea
ls an
d se
nior
supp
ort
Adu
lt da
y ca
reM
enta
l hea
lth o
utpa
tient
Case m
anag
emen
t
Adu
lt fo
ster c
are
The in
stitu
tiona
l sys
tem
Inde
pend
ent/R
etire
men
t liv
ing
Resid
entia
l/Per
sona
l car
eA
ssist
ed li
ving
Skill
ed n
ursin
gSu
bacu
te ca
reSp
ecia
lized
care
Figure 1–3 The Continuum of Long-Term Care
74035_CH01_5368.qxd 8/4/09 9:42 AM Page 16
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION

are perhaps more than 7 million Americanswho provide care to more than 4 million el-derly persons with functional limitations.The economic value of such care may be ashigh as $96 billion a year (O’Keeffe & Siebe-naler, 2006). For the most part, services ren-dered are believed to be basic, such as generalsupervision and monitoring, running errands,dispensing medications, cooking meals, as-sistance with eating, grooming and dressing,and, to a lesser extent, assistance with mo-bility and transfer.
The extent of informal care that an indi-vidual receives is highly dependent on theextent of the social support network theindividual has. People with close family,friends, neighbors, or surrogates (such asmembers of a religious community) can of-ten continue to live independently muchlonger than those who have little or no socialsupport. For those who do not have an ade-quate informal support network, community-based services can become an importantresource for allowing an individual to con-tinue to live independently.
The Community-Based SystemCommunity-based LTC consists of formalservices provided by various health careagencies. These services can be categorizedas intramural and extramural. Community-based LTC services have a fourfold objective:
1. To deliver LTC in the most economi-cal and least restrictive setting when-ever appropriate for the patient’shealth care needs.
2. To supplement informal caregivingwhen more advanced skills are need-ed than what family members or sur-rogates can provide to address thepatients’ needs.
3. To provide temporary respite to fam-ily members from caregiving stress.
4. To delay or prevent institutional-ization.
Intramural ServicesIntramural services are taken to patientswho live in their own homes, either alone orwith family. The most common intramuralservices include home health care and MealsOn Wheels. Limited support programs thatprovide services such as homemaker, choresand errands, and handyman assistance alsoexist, but the funding to pay for such servicesis not well established and varies from com-munity to community.
Extramural ServicesExtramural services are community-basedservices that are delivered outside a patient’shome. They require that patients come andreceive the services at a community-basedlocation. This category mainly includesambulatory services, such as adult day care,mental health outpatient clinics, and con-gregate meals provided at senior centers.Respite care is another type of service thatcan be classified as extramural.
Adult day care enables a person to livewith family but receive professional servicesin a daytime program in which nursing care,rehabilitation therapies, supervision, and so-cial activities are available. Adult day carecenters generally operate programs duringnormal business hours five days a week.Some programs also offer services in theevenings and on weekends. Senior centers arelocal community centers where seniors cancongregate and socialize. Many centers offera daily meal. Others sponsor wellness pro-grams, health education, counseling services,
The Long-Term Care Delivery System 17
74035_CH01_5368.qxd 8/4/09 9:42 AM Page 17
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION

information and referral, and some limitedhealth care services. Respite care can includeany kind of LTC service (adult day care,home health, or temporary institutionaliza-tion) when it allows family caregivers to taketime off while the patient’s care is taken overby the respite care provider. It allows familymembers to get away for a vacation or dealwith other personal situations without ne-glecting the patient.
The Institutional SystemA variety of LTC institutions form the insti-tutional continuum, with facilities rangingfrom independent living facilities or retire-ment centers at one extreme to subacute careand specialized care facilities at the other ex-treme (see the lower section of Figure 1–3).On the basis of the level of services they pro-vide, institutional LTC facilities may be clas-sified under six distinct categories:
• Independent or retirement living.
• Residential or personal care.
• Assisted living.
• Skilled nursing.
• Subacute care.
• Specialized care.
For most people, the array of facilitiesthat often go by different names can be re-markably confusing. This is particularly truebecause distinctions between some of themcan be blurry. For example, what is definedas board-and-care (i.e., residential and per-sonal care) in one state may be called assist-ed living in another. This is because servicesprovided by these facilities can overlap. Briefdescriptions of these facilities follow. Addi-tional details are found in Chapter 3.
Independent or Retirement HousingIndependent housing units and retirement liv-ing centers are not LTC institutions in the truesense because they are meant for people whocan manage their own care. These residencesdo not deliver clinical care but emphasizeprivacy, security, and independence. Theirspecial features and amenities are designedto create a physically supportive environ-ment to promote an independent lifestyle. Forexample, the living quarters are equipped withemergency call systems. Bathrooms havesafety grab bars. Rooms are furnished withkitchenettes. Congregate housing units havehandrails in the hallways for stability whilewalking. Other housing units offer detachedcottages with individual garages that allowresidents to come and go as they please. Ho-tel services such as meals, housekeeping, andlaundry may or may not be available.
Residential or Personal Care HomesFacilities in this category go by differentnames such as domiciliary care facilities,adult care facilities, board-and-care homes,and foster care homes. In addition to provid-ing a physically supportive environment, thesefacilities generally provide light assistive caresuch as medication use management and as-sistance with bathing and grooming. Otherbasic services such as meals, housekeeping,laundry, and social and recreational activitiesare also generally included. Because person-al care homes are located in residential neigh-borhoods, they are sometimes regarded as acommunity-based rather than an institutionalservice.
Assisted Living FacilitiesAn assisted living facility can be described asa residential setting that provides personal
18 CHAPTER 1 • Overview of Long-Term Care
74035_CH01_5368.qxd 8/4/09 9:42 AM Page 18
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION

care services, 24-hour supervision, sched-uled and unscheduled assistance, socialactivities, and some nursing care services(Citro & Hermanson, 1999). The services arespecially designed for people who cannotfunction without assistance and thereforecannot be accommodated in a retirement liv-ing or residential care facility.
The range of services in assisted livingfacilities is similar to that in personal carehomes, except that the level of frailty amongthe residents is generally higher. Hence, as-sistance with some ADLs is often furnished.Common types of ADL help include assis-tance with eating, bathing, dressing, toileting,and ambulation. Most residents also requirehelp with medications.
Skilled Nursing FacilitiesThese are the typical nursing homes at thehigher end of the institutional continuum.Compared with the types of residences dis-cussed earlier, the environment in skillednursing facilities is more institutionalizedand clinical. Yet, many facilities have imple-mented creative ideas in layout and design tomake their living environments as pleasantand homelike as practicable. Some of theseinnovations are discussed in Chapter 8.
These facilities employ full-time admin-istrators who must understand the varied con-cepts of clinical and social care and have beentrained in management and leadership skills.The facility must be adequately equipped tocare for patients who require a high level ofnursing services and medical oversight, yetthe quality of life must be maximized. A va-riety of disabilities—including problems withambulation, incontinence, and behavioralepisodes—often coexist among a relativelylarge number of patients. Compared with oth-er types of facilities, nursing homes have a
significant number of patients who are cog-nitively impaired, suffer from other mentalailments such as depression, and have phys-ical disabilities and conditions that often re-quire professional intervention. The socialfunctioning of many of these patients has alsoseverely declined. Hence, the nursing homesetting presents quite a challenge to admin-istrators in the integration of the four servicedomains discussed earlier—medical care,mental health services, social support, andresidential amenities.
Subacute Care FacilitiesSubacute care, defined earlier, has becomea substitute for services that were previous-ly provided in acute care hospitals. It hasgrown because it is a cheaper alternative tohospital stay. Early discharge from acutecare hospitals has resulted in a populationthat has greater medical needs than whatskilled care facilities were earlier able toprovide.
Specialized Care FacilitiesBy their very nature, both subacute care andspecialized care place high emphasis onmedical and professional nursing services.Some nursing homes have opened specializedcare units for patients requiring ventilatorcare, treatment of Alzheimer’s disease, inten-sive rehabilitation, or closed head traumacare. Other specialized facilities include in-termediate care facilities for the mentally re-tarded (ICF/MR). The key distinguishingfeature of the latter institutions is specializedprogramming and care modules for patientssuffering from mental retardation and asso-ciated disabilities. Another type of specializedfacility provides pediatric LTC to childrenwith developmental disabilities.
The Long-Term Care Delivery System 19
74035_CH01_5368.qxd 8/4/09 9:42 AM Page 19
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION

The Non-Long-Term Health Care SystemHealth care services described in this sectionare complementary to long-term care. Eventhough these services fall outside the LTCdomain, they are often needed by long-termcare patients. Hence, ideally, the twosystems—long-term care and non–long-termcare—should be rationally linked. The fol-lowing are the main non-LTC services thatare complementary to long-term care:
• Primary care, which is defined as med-ical care that is basic, routine, coordi-nated, and continuous over time. It isdelivered mainly by community-basedphysicians. It can also be rendered bymid-level providers such as physician’sassistants or nurse practitioners. Prima-ry care is brought to the patients who re-side in nursing homes, whereas thoseresiding in less institutionalized settingssuch as retirement living communities orpersonal care homes commonly visit theprimary care physician’s office.
• Mental health care delivered by commu-nity-based mental-health outpatient clin-ics and psychiatric inpatient hospitals.
• Specialty care delivered by community-based physicians in specialty practices,such as cardiology, ophthalmology,dermatology, or oncology. Certain ser-vices are also delivered by freestandingchemotherapy, radiation, and dialysiscenters. Other services are provided bydentists, optometrists, opticians, podia-trists, chiropractors, and audiologists incommunity-based clinics or mobile unitsthat can be brought to a long-term carefacility.
• Acute care delivered by hospitals and out-patient surgery centers. Acute episodes in
a LTC setting require transfer of the pa-tient to a hospital by ambulance.
• Diagnostic and health screening servicesoffered by hospitals, community-basedclinics, or mobile medical services. Somecommon types of services brought toLTC facilities include preventive den-tistry, X-ray, and optometric care.
Rational Integration of Long-Term Careand Complementary ServicesThe LTC delivery system cannot function in-dependently of other health care services.Hence, the LTC system must be rationallylinked to the rest of the health care deliverysystem (Figure 1–4). In a well-integratedsystem, patients should be able to move withrelative ease between needed services. Atleast some streamlining and coordination ofservices can be achieved through informa-tion technology, such as electronic healthrecords.
Types of services comprising the broad-er health care continuum are summarized inTable 1–1. Long-term care patients, regardlessof where they may be residing, frequently re-quire a variety of services along the healthcare continuum, dictated by the changes inthe patient’s condition and episodes that oc-cur over time. As an example, a person livingat home may undergo partial mastectomy forbreast cancer, return home under the care ofa home health agency, require hip surgery af-ter a fall in the home, and subsequently beadmitted to a skilled nursing facility for re-habilitation. This individual will need recu-peration, physical therapy, chemotherapy, andfollow-up visits to the oncologist. Once she isable to walk with assistance and her overallcondition is stabilized, she may wish to be
20 CHAPTER 1 • Overview of Long-Term Care
74035_CH01_5368.qxd 8/4/09 9:42 AM Page 20
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION

moved to an assisted living facility. To ade-quately meet the changing needs of such apatient, the system requires rational integra-tion, but the flow of care is not always assmooth as it should be. Integrated care alsorequires an evaluation of the patient’s needsin accordance with the type and degree of im-
pairment and a reevaluation as conditionschange. Depending on the change in condi-tion and functioning, the patient may movebetween the various levels and types of LTCservices and may also need transferring be-tween LTC and non-LTC services.
Rational Integration of Long-Term Care and Complementary Services 21
Health care delivery system
Promotion of independentfunctioning
Access to appropriateLTC services
Eval
uatio
nan
dre
eval
uatio
n
Individual needs
Type and degreeof impairment
Rational integration
Long-term careservices
Non-long-term careservices
Figure 1–4 Key Characteristics of a Well-Designed LTC System
74035_CH01_5368.qxd 8/4/09 9:42 AM Page 21
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION

For Further Thought1. How does long-term care differ from other types of medical services?
2. How can a nursing home facilitate the delivery of total care?
3. Why is it important that caregivers in long-term care settings not perform every taskof daily living for the patient? How much should caregivers do for patients who havefunctional impairments?
4. For nursing home residents, dignity and privacy issues are often more important thanclinical quality. Identify some staff practices that will promote each individual’s pri-vacy and dignity.
22 CHAPTER 1 • Overview of Long-Term Care
Table 1–1 The Continuum of Health Care Services
Types of Health Services Delivery Settings
Preventive care Public health programsCommunity programsPersonal lifestyles
Primary care Physician’s office or clinicSelf-careAlternative medicine
Specialized care Specialist provider clinicsChronic care Primary care settings
Specialist provider clinicsHome healthLong-term care facilitiesSelf-careAlternative medicine
Long-term care Long-term care facilitiesHome health
Subacute care Special subacute units (hospitals, long-term care facilities)Home healthOutpatient surgical centers
Acute care HospitalsRehabilitative care Rehabilitation departments (hospitals, long-term care facilities)
Home healthOutpatient rehabilitation centers
End-of-life care Hospice services provided in a variety of settings
74035_CH01_5368.qxd 8/4/09 9:42 AM Page 22
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION

For Further LearningAdministration on Aging: A federal agency established under the Older Americans Act.
www.aoa.gov/
Family Caregiver Alliance: A nonprofit organization set up to provide information and resources toaddress the needs of families and friends providing long-term care at home.
http://www.caregiver.org
The George Washington Institute for Spirituality and Health: Affiliated with the George WashingtonUniversity, the Institute is a leading organization on educational and clinical issues related to spiritu-ality and health.
http://www.gwish.org/
The Meals On Wheels Association of America: This organization represents those who provide con-gregate and home-delivered meal services to people in need.
http://www.mowaa.org/index.asp
National Council on Aging: A private, nonprofit organization providing information, training, techni-cal assistance, advocacy, and leadership in all aspects of care for the elderly. It provides informationon training programs and in-home services for older people. Publications are available on topics suchas lifelong learning, senior center services, adult day care, long-term care, financial issues, seniorhousing, rural issues, intergenerational programs, and volunteers serving the aged.
www.ncoa.org
National Mental Health Association: The country’s oldest and largest nonprofit organization that ad-dresses all aspects of mental health and mental illness.
www.nmha.org
REFERENCES
Altman, B.M. 1995, July. Elderly Persons with Developmental Disabilities in Long-Term Care Fa-cilities. AHCPR Pub. No. 95-0084. Rockville, MD: Agency for Health Care Policy and Re-search (now Agency for Healthcare Research and Quality).
Burns, B. et al. 1993. Mental health service use by the elderly in nursing homes. American Journalof Public Health 83: 331–337.
Citro, J., & Hermanson, S. 1999. Fact sheet: Assisted living in the United States. Washington, DC:American Association of Retired Persons.
Compston, A., & Coles, A. 2002. Multiple sclerosis. Lancet 359, no. 9313: 1221–1231.
DHHS. 1999. Mental health: A report of the Surgeon General. Rockville, MD: U.S. Department ofHealth and Human Services.
DHHS. 2008a. Trends in health and aging. Respondent-assessed health by age, sex, and race/ethnicity:United States, 1982–2006. Available at: http://205.207.175.93/aging/TableViewer/tableView.aspx (accessed September 2008).
DHHS. 2008b. Early release of selected estimates based on data from the 2007 National Health In-terview Survey. Available at: http://www.cdc.gov/nchs/data/nhis/earlyrelease/earlyrelease200806.pdf (accessed September 2008).
References 23
74035_CH01_5368.qxd 8/4/09 9:42 AM Page 23
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION

Federal Interagency Forum on Aging-Related Statistics. 2004. Older Americans 2004: Key Indica-tors of Well-Being. Washington, DC: U.S. Government Printing Office.
Feld, S., & George, L.K. 1994. Moderating effects of prior social resources on the hospitalizationsof elders who become widowed. Journal of Aging and Health 6: 275–295.
Health Care Financing Administration. 1996. Nursing home quality of life study spotlights resi-dents’ concerns. Health Care Financing Review 17, no. 3: 324.
Heller, T., et al. 1998. Impact of age and transitions out of nursing homes for adults with develop-mental disabilities. American Journal of Mental Retardation 103, no. 3: 236–248.
Heller, T., et al. 1999. Autonomy in residential facilities and community functioning of adults withmental retardation. Mental Retardation 37, no. 6: 449–457.
Heller, T., et al. 2002. Eight-year follow-up of the impact of environmental characteristics on well-being of adults with developmental disabilities. Mental Retardation 40, no. 5: 366–378.
Kaiser (Kaiser Commission on Medicaid and the Uninsured). 2007. Medicaid Facts. The Henry J.Kaiser Family Foundation. Available at: http://www.kff.org/medicaid/upload/2186_05.pdf (ac-cessed September 2008).
Krause, N., & Borawski-Clark, E. 1994. Clarifying the functions of social support in later life. Re-search on Aging 16: 251–279.
Lawton, M.P., & Brody, E.M. 1969. Assessment of older people: Self-maintaining and instrumentalactivities of daily living. Gerontology 9: 179–186.
McLeod, B.W. 2002. And Thou Shalt Honor: A Caregiver’s Companion. Wiland-Bell Productions,distributed by Rodale at www.rodalestore.com.
New York City Department of Health and Mental Hygiene. 2004. HIV Surveillance and Epidemiolo-gy Program Quarterly Report, 2, no. 1. New York: New York City Department of Health andMental Hygiene.
NIMH (National Institute of Mental Health). 2007. Older Adults: Depression and Suicide Facts.Available at: http://www.nimh.nih.gov/health/publications/older-adults-depression-and-suicide-facts.shtml (accessed September 2008).
O’Keeffe, J. & Siebenaler, K. 2006. Adult Day Services: A Key Community Service for Older Adults.Washington, DC: U.S. Department of Health and Human Services.
Shin, J.K. et al. 2002. Quality of care measurement in nursing home AIDS care: A pilot study. Jour-nal of the Association of Nurses in AIDS Care 13, no. 2: 70–76.
Smalbrugge, M., et al. 2006. The impact of depression and anxiety on well-being, disability and useof health care services in nursing home patients. International Journal of Geriatric Psychiatry21, no. 4: 325–332.
Spreat, S., et al. 1998. Improve quality in nursing homes or institute community placement? Imple-mentation of OBRA for individuals with mental retardation. Research in Developmental Dis-abilities 19, no. 6: 507–518.
Watson, L.C., et al. 2006. Depression in assisted living is common and related to physical burden.American Journal of Geriatric Psychiatry 14, no. 10: 876–883.
24 CHAPTER 1 • Overview of Long-Term Care
74035_CH01_5368.qxd 8/4/09 9:42 AM Page 24
© Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION