Introduction to Leukemia
Introduction to LeukemiaThe Acute LeukemiasLeukemias typically
fill up the marrow with abnormal cells, displacing normal
hematopoiesis. The marrow here is essentially 100% cellular, but
composed almost exclusively of leukemic cells. Normal hematopoiesis
is reduced via replacement (a "myelophthisic" process) or by
suppressed stem cell division.
Leukemias - DefinitionLeukemic cells are frequently present in
the:peripheral bloodinvade the reticulendothelial tissuesspleen,
liver, and lymph nodesmay also invade other tissuesuntreated,
eventually causes deathClassificationClassified according to cell
type with regard to both:cell maturity used to distinguish between
acute and chronic leukemiaif malignant cells are immature
acuterapidly aggressiveif predominantly mature - chronicslow or
indolent coursecell lineageMyeloid (granulocytic, monocytic,
megakaryotic, and erythrocytic )LymphoidCategories of
LeukemiasAcute lymphoid leukemia (ALL)Acute myeloid leukemia (AML)
or acute nonlymphoblastic leukemia (ANLL)Chronic lymphocytic
leukemiaAcute lymphocytic leukemiaEtiology/Risk
FactorsHeredityCongenital chromosomal abnormalitieshereditary
immunodeficiency statesChronic marrow dysfunctionDrugs anticancer
drugsIonizing radiationChemicalsVirusesHTLV-1 causative agent of
adult T-cell leukemia/lymphomaComparison of Acute and Chronic
LeukemiaAcuteChronicAgeAll agesAdultsClinical
onsetSuddenInsidiousCourse (untreated)< 6 mo2 6 yearsLeukemic
cellsImmatureMatureAnemiaMild to severeMild ThrombocytopeniaMild to
severeMildWhite cell
countVariableIncreasedOrganomegalyMildProminentAcute
LeukemiaClassification and DifferentiationClinical Features of
Acute LeukemiaPathogenesisClinical ManifestationsBone Marrow
Failure AnemiaFatigue, malaise, pallor ThrombocytopeniaBruising,
bleeding GranulocytopeniaFever, infectionsOrgan Infiltration Marrow
expansionBone or joint pain SpleenSplenomegaly LiverHepatomegaly
Lymph nodesLymphadenopathy Central nervous systemNeurologic
symptoms Gums, mouthGingival hypertrophy,oral lesionsLaboratory
Evaluation of Acute LeukemiaPurpose: Confirm the diagnosis and
distinguish AML from ALLPreliminary evaluation:complete blood count
and peripheral blood examinationbone marrow studiesmorphologic
examinationcytochemical staining immunologic markerscytogenetic
studiesmolecular genetic studieselectron microscopy ?Morphologic
Approach to ClassificationCytologic Features of Blasts in Acute
ANLL and Acute Lymphocytic LeukemiaFeatureAMLALLBlast sizeLarger,
usually uniformVariable, small to medium sizeNuclear
chromatinUsually finely dispersedCoarse to fineNucleoli1-4, often
prominentAbsent or 1-2, often indistinctCytoplasmModerately,
abundant, fine granules often presentUsually scant, coarse granules
sometimes present (~7%)Auer rodsPresent in 60-70% of casesNot
presentOthersOften dysplastic changes in maturing myeloid
cellsMyeloid cells not dysplastic
Copyright 2003 American Society of Hematology. Copyright
restrictions may apply.Maslak, P. ASH Image Bank
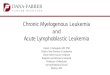
2003;2003:100726Figure 1. A type I myeloblast has a large nuclus
with prominent nucleoli12
Copyright 2003 American Society of Hematology. Copyright
restrictions may apply.Maslak, P. ASH Image Bank
2003;2003:100739Figure 3. Small number of granules are clustered in
the cytoplasm of this myeloblast13
Copyright 2004 American Society of Hematology. Copyright
restrictions may apply.Maslak, P. ASH Image Bank
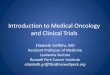
2004;2004:100953Figure 2. Type III blasts have greater than 20
granules but no centrosome14
Copyright 2005 American Society of Hematology. Copyright
restrictions may apply.Maslak, P. ASH Image Bank
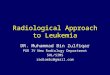
2005;2005:101341Figure 1. Auer rods are distinctive cytoplasmic
inclusion bodies which are found in MDS and AML15
Copyright 2004 American Society of Hematology. Copyright
restrictions may apply.Maslak, P. ASH Image Bank
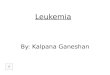
2004;2004:101139Figure 1. This lymphoid blast has a rounded,
"regular" appearance without cytoplasmic granules16Cytochemical
Reactions Useful in the Diagnosis of Acute LeukemiaSpecial
StainSite of ActionCells StainedCommentMyeloperoxidaseMainly
primary granules; Auer rodsLate myeloblasts, granulocytes;
monocytes less intenselySeparates AML (+) from ALL (-)Sudan black
BPhospholipids; sterols, neutral fatsLate myeloblast, granulocytes;
monocytes less intenselyParallels peroxidase, but smears do not
need to freshSpecific esterase (Naphthol AS-D
chloroacetateCytoplasmNeutrophilic granulocytes; mast
cellsParallels peroxidase, but less sensitive; Non-specific
esterase (alpha-napththyl acetate and butyrate)CytoplasmMonocytes;
focal staining in T cellsUseful for determining degree of monocytic
differentiation; separates mono (+) from myelo (-) blastsPeriodic
acid-SchiffGlycogen and related substancesLymphocytes,
granulocytes, megakaryocytesHelpful in supporting diagnosis of
erythroleukemiaImmunologic Markers Used in the Classification of
Acute LeukemiaLineageAntigenB cellCD19, CD20, CD21, CD22, CD23,
D24T cellCD1, CD2, CD3, CD4, CD5, CD7, CD8LymphoidTdTMyeloid
(granulocytic)CD13, CD33, CD11b, CD15MonocyticCD14,
CD11bErythroidGlycophorin AMegakaryocyticCD41, CD42b, CD61Lineage
Independent AntigensHLA-DRHLA class IICD45Leukocyte common
antigenCD34Stem cell antigenCD10Common ALL antigen (CALLA)Acute
Myeloid Leukemia(AML)Acute Nonlymphoid Leukemia(ANLL)DefinitionAML
are clonal malignancies that are characterized by the appearance of
increased numbers of immature myeloid cells in the marrow and
blood.DefinitionAML is a clonal, malignant disease of the
hematopoietic tissue that is characterized byaccumulation of
abnormal (leukemic) blast cells, principally in the marrowimpaired
production of normal blood cells.EtiopathogenesisRisk
factorsEnvironmentalradiationbenzenesalkylating agents and other
cytotoxic drugs therapy-related AMLEvolution from a chronic clonal
hemopathyInherited syndromesEpidemiologyAML is the predominant form
of leukemia during the neonatal period and accounts for 15 to 20
percent of acute leukemia in children and80 percent of acute
leukemia in adults.
Revised Criteria for the Classification of AML (FAB)M0 with
minimal differentiationLarge, agranular blasts (resemble ALL L2,
rarely L1). Myeloperoxidase negative or90 percent of non erythroid
cells. At least 3 percent of these are myeloperoxidase or Sudan
black positive.Remaining 10 percent (or less) of cells are maturing
granulocytes or monocytesRevised Criteria for the Classification of
AML (FAB)M2 with maturationSum of agranular and granular blasts
(types I and II) is from 30 to 89 percent of non-erythroid
cells.Monocytic cells, 10 percent.M3 PromyelocyticMajority of cells
are abnormal promyelocytes with heavy granulation.Characteristic
cells containing bundles of Auer rods (faggots) invariably present.
Note: Microgranular variant (M3v) also occurs. Promyelocytes have
marked nuclear irregularity that includes reniform, lobulated and
monocyte-like indented nuclei. The cytoplasm contains fine or
indistinct granules in contrast to the coarse azurophilic granules
in typical M3.Revised Criteria for the Classification of AML
(FAB)M4 MyelomonocyticIn the marrow, blasts >30 percent of
non-erythroid cells.Sum of myeloblasts, promyelocytes, myelocytes
and later granulocytes is between 30 and 80 percent of
non-erythroid cells.> 20 percent of non-erythroid cells are
monocyte lineage.If monocytic cells exceed 80 percent, diagnosis is
M5 Note: (a) If marrow findings as above and peripheral blood
monocytes (all types) are > 5.0 x 109/L, diagnosis is M4 (b) If
monocyte count < 5 x 109/L, M4 can be confirmed on basis of
serum lysozyme, combined esterase, etc. (c) Diagnosis of M4
confirmed if > 20 percent of marrow precursors are monocytes
(confirmed by special stains).Revised Criteria for the
Classification of AML (FAB)M4 with eosinophiliaEosinophils > 5
percent of non-erythroid cells in marrow.Eosinophils are
abnormal.Eosinophilis are chloroacetate and PAS positive.M5
Monocytic80 percent of marrow non-erythroid cells are monoblasts,
promonocytes or monocytes.M5a, 80 percent of monocytic cells are
monoblasts.M5b, < 80 percent of monocytic cells are monoblasts,
remainder are predominantly promonocytes and monocytes.Revised
Criteria for the Classification of AML (FAB)M6 ErythroleukemiaThe
erythroid component of the marrow exceeds 50 percent of all
nucleated cells.30 of the remaining non-erythroid cells are
agranular or granular blasts ( types I and II). Note: If > 50
percent erythroid cells but < 30 percent blasts, diagnosis
becomes myelodysplastic syndromes. A rare form of erythoird
neoplasia, erythremic myelosis, involves only the red blood cell
precursors. The erythroblasts, primarily pronormoblasts and
basophilic normoblasts, constitute 90% or more of the marrow
cells.M7 Megakaryocytic30 percent at least of nucleated cells are
blasts.Blasts identified by platelet peroxidase on electron
microscopy, or by monoclonal antibodies.Increased reticulin is
common.
Copyright 2003 American Society of Hematology. Copyright
restrictions may apply.Maslak, P. ASH Image Bank
2003;2003:100838Figure 1. Blasts are the predominant population in
the bone marrowAML (M1)29
Copyright 2003 American Society of Hematology. Copyright
restrictions may apply.Maslak, P. ASH Image Bank
2003;2003:100722Figure 2. Aspirate has a large number of blastsAML
(M2)30
Copyright 2002 American Society of Hematology. Copyright
restrictions may apply.Maslak, P. et al. ASH Image Bank
2002;2002:100532Figure 1. The most common form of APL is easily
recognized by the heavy granulation of the abnormal promyelocytes
(AML M3)31
Copyright 2002 American Society of Hematology. Copyright
restrictions may apply.Maslak, P. et al. ASH Image Bank
2002;2002:100598Figure 1. The granules in this morphologic variant
of APL are less prominent than those seen in the most common form
of this disease32
Copyright 2004 American Society of Hematology. Copyright
restrictions may apply.Lazarchick, J. ASH Image Bank
2004;2004:101148Figure 4. The increased number of blasts are noted
with a prominent background of eosinophils and abnormal
eosinophilic myelocytes33
Copyright 2002 American Society of Hematology. Copyright
restrictions may apply.Maslak, P. et al. ASH Image Bank
2002;2002:100537Figure 1. Monoblasts are large cells with ample
cytoplasm34
Copyright 2003 American Society of Hematology. Copyright
restrictions may apply.Maslak, P. ASH Image Bank
2003;2003:100635Figure 3. Erythroid elements comprise greater than
or equal to 50% of the nucleated cellular elements while the
myeloblasts make up greater than or equal to 20% of the
nonerythroid population35
Copyright 2002 American Society of Hematology. Copyright
restrictions may apply.Maslak, P. ASH Image Bank
2002;2002:100478Figure 1. Blasts in acute megakaryoblastic leukemia
may show cytoplasmic budding reminiscent of the process where
platelets are shed from normal megakaryocytes (MacNeal Tetrachrome
400x)36Common Cytogenetic Abnormalities Associated with
AMLChromosomeAbnormalityAssociated Disordert(8;21)AML
(M2)t(15;17)Unique to APL (M3)16q abnormalities:inv (16) and del
(16)AML with abnormal eosinophilia (M4E)t9;22)
t(9;11)TreatmentRemission-induction therapyPost-remission
maintenance therapyStem cell transplantAcute Lymphoid Leukemiaacute
lymphoblastic leukemiaacute lymphocytic leukemiaDefinitionALL is a
neoplastic disease that results from multistep somatic mutations in
a single lymphoid progenitor at one of several discrete stages of
development.The immunophenotype of leukemic cells at diagnosis
reflects the level of differentiation achieved by the dominant
clones.
EtiopathogenesisRisk FactorsGenetic syndromesEnvironmental
factorsHost pharmocogeneticsIn utero development of ALLEvent-free
and Overall Survival in ALL
FAB Classification of ALLMorphologicFeaturesL1L2L3Cell
sizeSmallLargeLargeNuclear chromatinFine or clumpedFineFineNuclear
shapeRegular, may have cleft of indentationIrregular, may have
cleft or indentationRegular, oval to roundNucleoliIndistinct or not
visible1 or more per cell; large prominent1 or more per cell; large
prominentAmount of cytoplasmScantyModerately abundantModerately
abundandCytoplasmic basophiliaSlightSlightProminentCytoplasmic
vacuolesVariableVariablevariableALL (L1)
ALL (L2)
ALL (L3)
Acute LeukemiaA heterogeneous group of neoplasms affecting
uncommitted or partially committed hematopoietic stem cells.The
retained capacity of some differentiation is the basis for the
phenotypic classification.Broadly divided into (based on cell
origin)Non-lymphoid (Myeloid) leukemiaLymphoid leukemia
Classification of LeukemiaAcute Myeloid (FAB classification)Acute
myeloblastic leukemiawithout differentiation (M0)without maturation
(M1)with maturation (M2)Acute promyelocytic leukemia (M3) APLAcute
myelomonocytic leukemia (M4) AMMLAcute monocytic leukemia (M5)
AMoLErythroleukemia (M6) Di Guglielmos syndromeAcute
megakaryoblastic leukemia (M7)Classification of LeukemiaAcute
LymphoblasticPrecursor B-cell ALLEarly-Pre-B-cell ALLPre-B-cell
ALLB-cell ALLT-cell ALLChronic MyeloidChronic myelogenous leukemia
(CML)Chronic eosinophilic leukemia (CEL)Chronic basophilic leukemia
(CBL)Classification of LeukemiaChronic LymphoidChronic lymphocytic
leukemia (CLL)B-cell CLLT-cell CLLProlymphocytic leukemiaHairy cell
leukemiaPlasma cell leukemiaSzary syndromeEtiology and Risk
FactorsHost FactorsHeredityCongenital chromosomal
abnormalitiesImmunodeficiencyChronic marrow
dysfunctionEnvironmental FactorsIonizing radiationChemicals and
drugsViruses