Embed Size (px)
Citation preview
INTRODUCTION TO CLOSTRIDIUM DIFFICILE INFECTIONSLIDE RESOURCE SET
FDX/13/0068/EU | August 2013

Introduction to Clostridium difficile
• C. difficile is a Gram-positive, spore-forming, anaerobic bacillus that was first identified in 19351
• C. difficile is the leading cause of infective nosocomial diarrhoea in industrialised countries2
• C. difficile passes through a life cycle where it exists in two forms; as vegetative cells and as spores3
1. Hall IC, O’Toole E. Am J Dis Child 1935;49:390–402;2. Crobach MJT, et al. Clin Microbiol Infect 2009;15:1053–66;3. Poutanen S, Simor AE. CMAJ 2004;171:51–8.
Vegetative form Spores surrounding a vegetative cell
FDX/12/0076/EUa | MW101

Clinical presentation of C. difficile infection (CDI)
• Asymptomatic colonisation
• Diarrhoea without colitis
– Watery
– Mucus but no blood
• Colitis without pseudomembrane formation
• Pseudomembranous colitis
• Fulminant colitis
Bauer MP, et al. Clin Microbiol Infect 2009;15:1067–79;Bartlett JD, Gerding DN. Clin Infect Dis 2008;46:S12–8.
Increasin
g severity
Normal, healthy colon
Pseudomembranous colitis
FDX/12/0076/EUb | SJ103

Other signs and symptoms of CDI, including severe colitis
• Vomiting
• Abdominal tenderness
• Fever (rigors)
• Dehydration
• Leucocytosis
• Hypoalbuminaemia
• Exhaustion
Bauer MP, et al. Clin Microbiol Infect 2009;15:1067–79.AI/12/0055/EUg | DM104

Risk factors for CDI
1. Cohen SH, et al. Infect Control Hosp Epidemiol 2010;31:431–55;2. Bignardi GE. J Hosp Infect 1998;40:1–15.
There are numerous reported risk factors
for CDI
Broad-spectrum
antibacterials1
Immuno-compromised2
Older age2
Severity of underlying diseases2Prolonged
stay in hospital/
care home2
ICU stay2
Nasogastric tube/
GI surgery2
PPIs2
GI, gastrointestinal;ICU, intensive care unit;
PPI, proton pump inhibitorFDX/12/0076/EUb | SJ108

Key steps in the pathogenesis of CDI
Kelly CP, LaMont JT. Annu Rev Med 1998;49:375–90.
Antibacterial therapy
Alteration of colonic microflora
C. difficile exposure and colonisation
Release of toxins A and B
Colonic mucosal injury and inflammation
FDX/13/0038/EUb | VA002

The infectious cycle of transmission and recurrence of CDI
Adapted from Sunenshine RH, et al. Cleve Clin J Med 2006;73:187–97.
1. Ingestion of spores transmitted from other patients, via hands of healthcare personnel and the environment
2. Germination into growing (vegetative) cells
3. Disruption of normal colonic microflora allows colonisation and overgrowth of C. difficile in the colon
4.Toxin production leads to inflammation and damage to intestinal cells
5. Transmission of spores via the faecal–oral route
C. difficile
Toxins
FDX/12/0076/EUb | SJ101

Cycle of infection with C. difficile
Adapted from Poutanen SM, Simor AE. CMAJ 2004;171:51–8.
C. difficilespores andvegetative cellsare ingested
Most vegetative cells are killed in the stomach,but spores can survivethe acid environment
C. difficile spores germinate in the small bowel uponexposure to bile acids
Flagellae facilitateC. difficile movement
C. difficile multiplies inthe colon
Gut mucosafacilitatesadherenceto thecolonicepithelium
ColonStomach
Small bowel
Spores Vegetative cells
FDX/13/0038/EUb | VA001

CDI is toxin mediated
• Toxin A*1
– Referred to as the ‘enterotoxin’ because of the easily demonstrated
effects of purified toxin in animal intestinal models
– Likely to be intimately involved in CDI pathogenesis
• Toxin B*1
– Potent cytotoxin
– Structurally similar to toxin A but effects in animal intestinal models have
not been easy to demonstrate
– Likely to be intimately involved in CDI pathogenesis
• Binary toxin– Unrelated to toxins A and B1
– Present in the epidemic BI/NAP1/027 strain2
– Role in pathogenesis uncertain21. Rupnik M, et al. Nat Rev Microbiol 2009;7:526–36;2. Warny M, et al. Lancet 2005;366:1079–84.
*Large, single-unit, glucosylating toxins;BI/NAP1, characterised as group BI by restriction
endonuclease analysis and North American pulse-field type 1 by gel electrophoresis
FDX/12/0076/EUb | SJ134

Role of host antibody-mediated responses in CDI pathogenesis
Adapted from Rupnik M, et al. Nat Rev Microbiol 2009;7:526–36.
Patients with risk factors for CDI,
including antibacterialuse in hospital setting
Exposure to toxigenicC. difficile accompanied by
IgG response to toxin A
C. difficile negative
Asymptomatically colonised
Asymptomatically colonised
Symptomatic CDI
Exposure to toxigenicC. difficile without an IgG response
to toxin A
Exposure to non-toxigenic C. difficile
IgG, Immunoglobulin G antibodyFDX/12/0076/EUb | SJ102

Impact of CDI on short- and long-term patient management
• CDI may necessitate treatments for underlying diseases to be reduced in intensity or suspended
– Alterations to treatment plans may irreversibly affect long-term outcomes1
• Episodes of CDI arising in the ICU may prolong ICU stay and overall hospitalisation2
– Excess ICU length of stay: 2.2 days (p=0.069)
– Excess hospital length of stay: 4.5 days (p=0.030)
1. Hautmann MG, et al. Radiat Oncol 2011;6:89; 2. Kenneally C, et al. Chest 2007;132:418–24.
FDX/12/0076/EUb | SJ119

Length of hospital stay among patients with CDI by country
Wiegand PN, et al. J Hosp Infect 2012;81:1–14.FDX/12/0076/EUd | DN139
EU, European Union
45
40
35
20
10
0
Leng
th o
f sta
y (d
ays)
Belgium
25
30
15
5
France
Germany
Ireland
Spain
Switzerland
Netherlands UK
16 17 17
1215
50
EU
27
2118
37

Association of CDI with hospital readmissions
Dubberke ER, et al. Emerg Infect Dis 2008;14:1031–8.
• In this study, CDI patients were significantly more likely to be readmitted to hospital than controls; the readmission rate attributable to CDI was 19.3%
Kaplan–Meier estimates of time until hospital readmission for matched pairs (N=580) in patients with and without CDI
1.0
0.8
0.6
0.4
0.2
0.00 30 60 90 120 150 180
Time since hospital discharge (days)
Pro
por
tion
with
out
read
mis
sion
No CDI
CDI
Log-rank p<0.001
FDX/12/0076/EUd | DN149

Association of CDI with mortality
Dubberke ER, et al. Emerg Infect Dis 2008;14:1031–8.
• 38% of patients with CDI died within 180 days after hospital admission vs 12% of patients without CDI
Kaplan–Meier survival estimates for cohort (N=18,050) in patients with and without CDI
1.0
0.8
0.6
0.4
0.2
0.0
Time since hospital discharge (days)
Cum
ula
tive
sur
viva
l No CDI
CDI
Log-rank p<0.001
0 30 60 90 120 150 180
FDX/12/0076/EUd | DN150

Mortality rates in studies of CDI
• In a recent pan-European hospital-based survey:1
– ~2% of patients with CDI died as a result of the infection
– CDI contributed to mortality in a further 7% of cases
• In a case-control study in Canada:2
– ~7% of patients with CDI died as a result of the infection
– CDI contributed to mortality in a further 8% of cases
1. Bauer MP, et al. Lancet 2011;377:63–73;2. Loo VG, et al. N Engl J Med 2005;353:2442–9.
FDX/12/0087/EUu | slide 013

Mortality rates associated with CDI across Europe
Wiegand PN, et al. J Hosp Infect 2012;81:1–14.
• Data from a systematic review found the weighted average 30-day mortality from CDI ranged from 3–30%
Weighted average 30-day mortality in patients with healthcare facility-acquired CDI by country
45
40
35
20
10
0
30-d
ay m
orta
lity
(%)
Austria
25
30
15
5
DenmarkFinland
France
Germany
Ireland
LuxembourgSpain
Switzerland
The Netherlands UK
14%16% 14%
3%
16%
7%
15%
22%
9%
20%
30%
FDX/12/0076/EUd | DN108

Age-specific incidence of CDI and attributable mortality
Loo VG, et al. N Engl J Med 2005;353:442–9.
<40 41–50 51–60 61–70 71–80 81–90 >900
10
20
30
40
50
60
70
80
CDI rate per 1,000 ad-missions
Attributable 30-day mortal-ity rate
Age (years)
Rat
e (%
)
FDX/12/0076/EUb | SJ113

Factors contributing to risk of mortality from CDI
• Advancing age1,2
• Older age and severity associated with the epidemic 027/NAP1 strain3
• Use of metronidazole for severe disease4
• Haematological malignancy and severe disease5
• Comorbidity– Renal disease4
– Ischaemic heart disease4
– Inflammatory bowel disease6
– Liver disease (cirrhosis)7
1. Loo VG, et al. N Engl J Med 2005;353:2442–9;2. Bauer MP, et al. Lancet 2011;377:63–73;3. Miller M, et al. Clin Infect Dis 2010;50:194–201;4. Wilson V, et al. Clin Infect Dis 2010;50:e77–81;
5. Dubberke ER, et al. Infect Con Hosp Epidemiol 2007;28:208–11;6. Ananthakrishnan AN, et al. Gut 2008;57:205–10;7. Bajaj JS, et al. Am J Gastroenterol 2010;105:106–13.
FDX/12/0076/EUb | SJ110
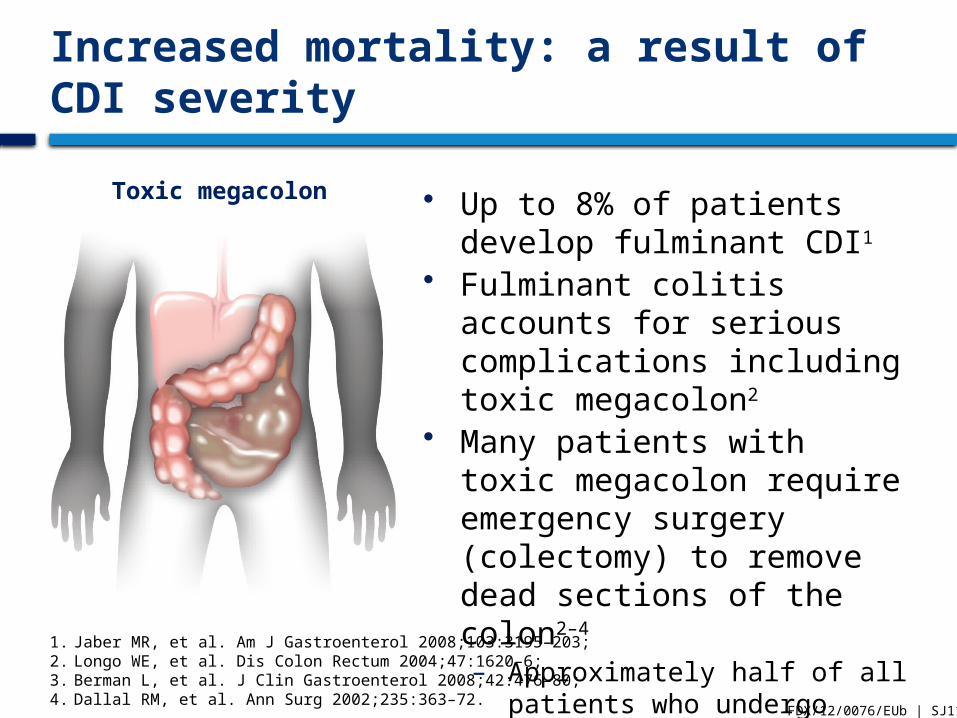
Toxic megacolon
Increased mortality: a result ofCDI severity
1. Jaber MR, et al. Am J Gastroenterol 2008;103:3195–203;2. Longo WE, et al. Dis Colon Rectum 2004;47:1620–6;3. Berman L, et al. J Clin Gastroenterol 2008;42:476–80;4. Dallal RM, et al. Ann Surg 2002;235:363–72.
• Up to 8% of patients develop fulminant CDI1
• Fulminant colitis accounts for serious complications including toxic megacolon2
• Many patients with toxic megacolon require emergency surgery (colectomy) to remove dead sections of the colon2–4
– Approximately half of all patients who undergo colectomy die3,4
FDX/12/0076/EUb | SJ111

Recurrence of CDI
• Recurrence of CDI has been identified by the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) as the most important problem in the treatment of CDI1
• CDI recurrence is common, occurring in up to 25% of cases within 30 days following treatment2–4
• Recurrence appears to be related to a combination of:5
– A failure to re-establish the colonic microflora
– The presence in the intestines of spores of C. difficile
– A sub-optimal host immune response to the infecting organism and its toxins
1. Bauer MP, et al. Clin Microbiol Infect 2009;15:1067–79;2. Louie TJ, et al. N Engl J Med 2011;364:422–31;3. Lowy I, et al. N Engl J Med 2010;362:197–205;4. Bouza E, et al. Clin Microbiol Infect 2008;14(Suppl 7):S103–4;5. DuPont HL. N Engl J Med 2011;364:473–4.
FDX/12/0076/EUb | SJ121

The incidence of recurrent CDI
1. Louie TJ, et al. N Engl J Med 2011;364:422–31;2. Lowy I, et al. N Engl J Med 2010;362:197–205;3. Bouza E, et al. Clin Microbiol Infect 2008;4(Suppl 7):S103–4;4. McFarland LV, et al. Am J Gastroenterol 2002;97:1969–75;5. McFarland LV, et al. JAMA 1994;271:1913–8.
1st recurrence of CDI
Recurrence(s) of CDI
~45–65% of patients have further
recurrences4,5
Up to 25% of patients have recurrent CDI1–3
Initial episode of CDI
FDX/12/0076/EUb | SJ122

Risk factors for a recurrence of CDI
• Immunocompromised state1
• Exposure to other antibacterial agents that disrupt the normal colonic microflora2–5
• Renal impairment6,7
• Aged 65 years or over2,4,8
• Impaired immune response to C. difficile toxin A2
• Severe underlying disease2
• Prolonged hospitalisation8
• ICU stay5
1. Cohen MB. J Pediatr Gastroenterol Nutr 2009;48(Suppl 2):S63–5;
2. Kyne L, et al. Lancet 2001;357:189–93;3. Bauer MP, et al. Clin Microbiol Infect 2009;15:1067–79;4. Bauer MP, et al. Lancet 2011;377:63–73;
5. Hu MY, et al. Gastroenterology 2009;136:1206–14;6. Do AN, et al. Clin Infect Dis 1998;26:954–9;7. Bauer MP, et al. Clin Microbiol Infect 2011;17(Suppl 4):A1–4;8. Pépin J, et al. Clin Infect Dis 2005;40:1591–7.
FDX/12/0076/EUr | SJ204

Laboratory detection of CDI
The recommended approach is to demonstrate:1,2
• Organism in stool– GDH or culture: do not distinguish toxigenic vs non-toxigenic
– Need confirmatory test for toxigenicity
• Toxin in stool– Cell culture toxin cytotoxicity
– EIA to detect toxins A and/or B
• Toxin from organism– Culture cytotoxicity
• Toxin genes in organism – PCR for toxin B gene1. Crobach MJT, et al. Clin Microbiol Infect 2009;15:1053–66;
2. Kelly CP, LaMont JT. Annu Rev Med 1998;49:375–90.FDX/12/0087/EUu | slide 018
EIA, enzyme immunoassay; GDH, glutamate dehydrogenase;PCR, polymerase chain reaction

−+ − +
ESCMID recommended diagnostic algorithm for CDI
Adapted from Crobach MJT, et al. Clin Microbiol Infect 2009;15:1053–66.
EIA to detectTcdA and TcdB
EIA to detect GDH, or real-time PCR to detect TcdB
EIA to detect GDH,or real-time PCR to detect TcdB, or
cytotoxicity assay
High clinical suspicion:
toxigenic culture
No CDI
CDI isdiagnosed
No CDICDI is
diagnosed
C. difficile toxins are not detectable in faeces
but C. difficile is present; CDI cannot be excluded
+ − − +
Toxin detection or bacterial detection
EIA, enzyme immunoassay; GDH, glutamate dehydrogenase;PCR, polymerase chain reaction
EIA to detect TcdA,and TcdB,
or cytotoxicity assay
FDX/12/0076/EUo | CS209

CDI imposes a significant burden on hospitals
• Infection control and environmental decontamination1
• Patient isolation and ward closures1
• Monitoring and surveillance2
• Laboratory tests3
• Surgical costs1,3
• ICU length of stay4
• Hospital length of stay2,4,5
1. Kuijper EJ, et al. Clin Microbiol Infect 2006;12:2–18;2. Wiegand PN, et al. J Hosp Infect 2012;81:1–14;3. Ghantoji SS, et al. J Hosp Infect 2010;74:309–18;4. Kenneally C, et al. Chest 2007;132:418–24;5. Vonberg RP, et al. J Hosp Infect 2008;70:15–20.
FDX/12/0076/EUb | SJ120

CDI: a public health challenge
• The recorded incidence and severity of CDI have increased in many settings in recent years, including in people previously thought to be at lower risk1–6
• Clusters/outbreaks of CDI cause ward closures and disruption of hospital activity7
• There is a considerable burden of morbidity and mortality due to CDI7
• The resultant effect is an erosion of public confidence concerning the risk of healthcare-associated infection
• Also, the financial burden of disease is high8
1. Bauer MP, et al. Lancet 2011;377:63–73; 2. Vonberg RP, et al. Emerg Infect Dis 2007;13:179–80;3. Soler P, et al. Infect Control Hosp Epidemiol 2008;29:887–9;4. Lyytikäinen O, et al. Emerg Infect Dis 2009;15:761–5;
5. Søes L, et al. Euro Surveill 2009;14:1–4;6. CDC. MMWR Morb Mortal Wkly Rep 2005;54:1201–5;7. Kuijper EJ, et al. Clin Microbiol Infect 2006;12:2–18;8. Wilcox M, et al. J Hosp Infect 1996;34:23–30.
FDX/12/0076/EUa | MW103





























