Embed Size (px)
Citation preview
Introduction of The Strategic Use of ARVs For Treatment & Prevention in
Indonesia:From Policy Development to
Implementation
Dr. Siti Nadia Tarmizi M EpidNational AIDS Program Manager
Ministry of Health Indonesia
Outline
1. Epidemiological situation and Programme Progress
– Prevention outcomes– Treatment outcomes
2. Rational for Policy Formulation3. Policy Implementation 4. Programmatic Questions and Challenges
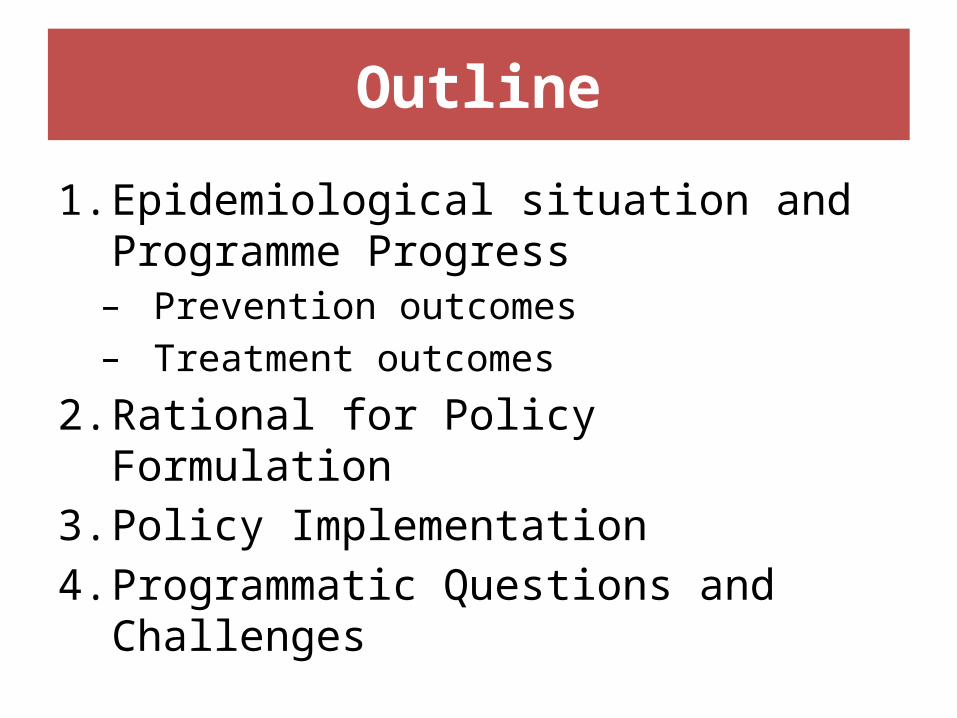
1. Epidemioliogical Background• Concentrated epidemic in most of country, but
low-level generalized epidemic in Papua
Source: Estimates & Projection of HIV/AIDS 2011-2016, MoH 2012

From Driven By Injection To Predominantly Sexual Transmission
Estimated Number of New Infections by Population Sub-Groups
Source: Estimates & Projection of HIV/AIDS 2011-2016, MoH 2012
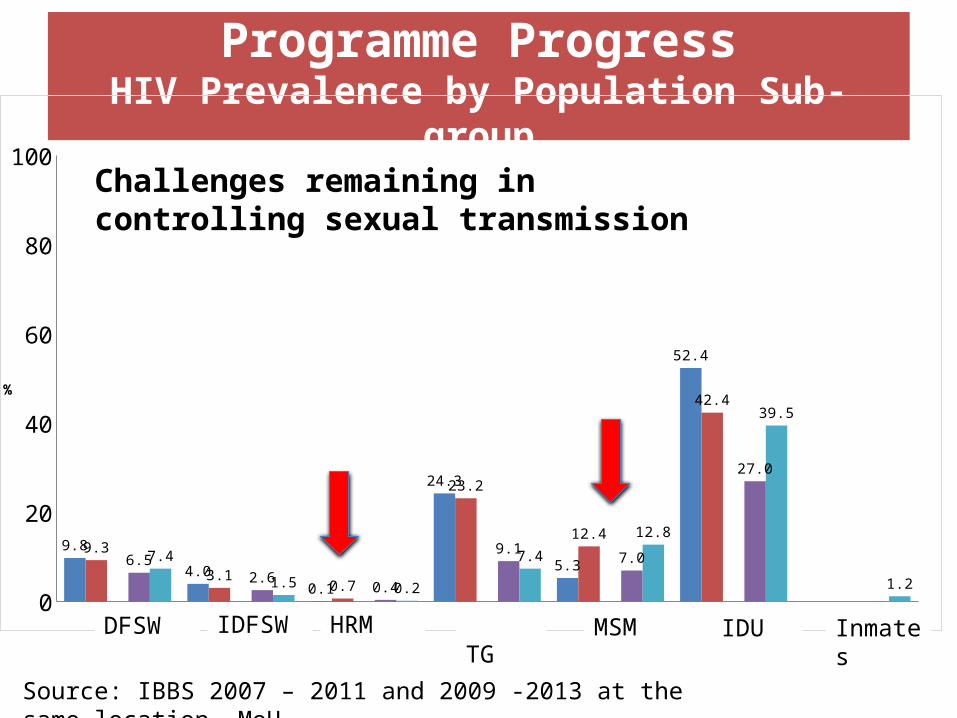
Programme Progress
HIV Prevalence by Population Sub-group
WPSL WPSTL Pria Risti Waria LSL Penasun WBP0
20
40
60
80
100
9.8
4.00.1
24.3
5.3
52.4
9.3
3.10.7
23.2
12.4
42.4
6.52.6
0.4
9.17.0
27.0
7.4
1.5 0.2
7.4
12.8
39.5
1.2
2007 2011 Series3 2009 2013
%
Challenges remaining in controlling sexual transmission
Source: IBBS 2007 – 2011 and 2009 -2013 at the same location, MoH
DFSW IDFSW HRM TG MSM IDU Inmates

Remaining Sexual Risk BehaviorsCondom Use at last sex
DFSW IDFSW IDU MSM Waria0
20406080
100
68 6955
6978
61 6556
68 7064 62
29
54 5868
59 52
74 77
Source: IBBS 2007 & 2011 and IBBS 2009 & 2013, MoH
Always Condom Use
DFSW IDFSW IDU MSM Waria0
20
40
60
80
100
68 6955
6978
61 6556
68 70
4133
9
31 3445
36
13
46 42
2007 2011 2009 2013
TG
TG
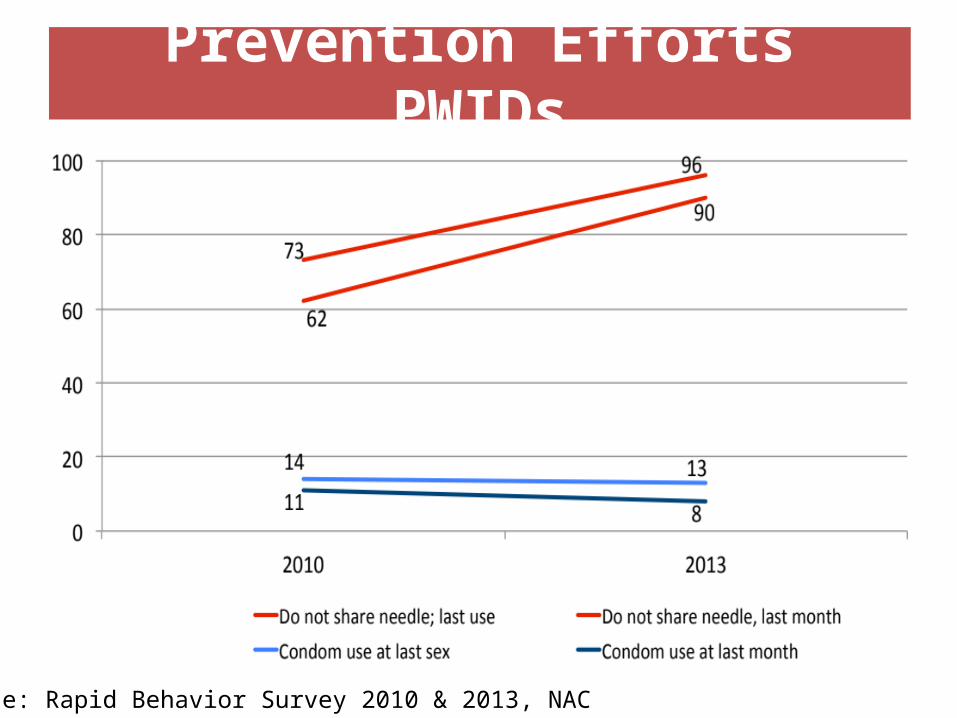
Prevention Efforts PWIDs
• Perilaku penggunaan kondom konsisten masih rendah (STBP 2009: 31%, 2013:46%).
Source: Rapid Behavior Survey 2010 & 2013, NAC
1 July 2014
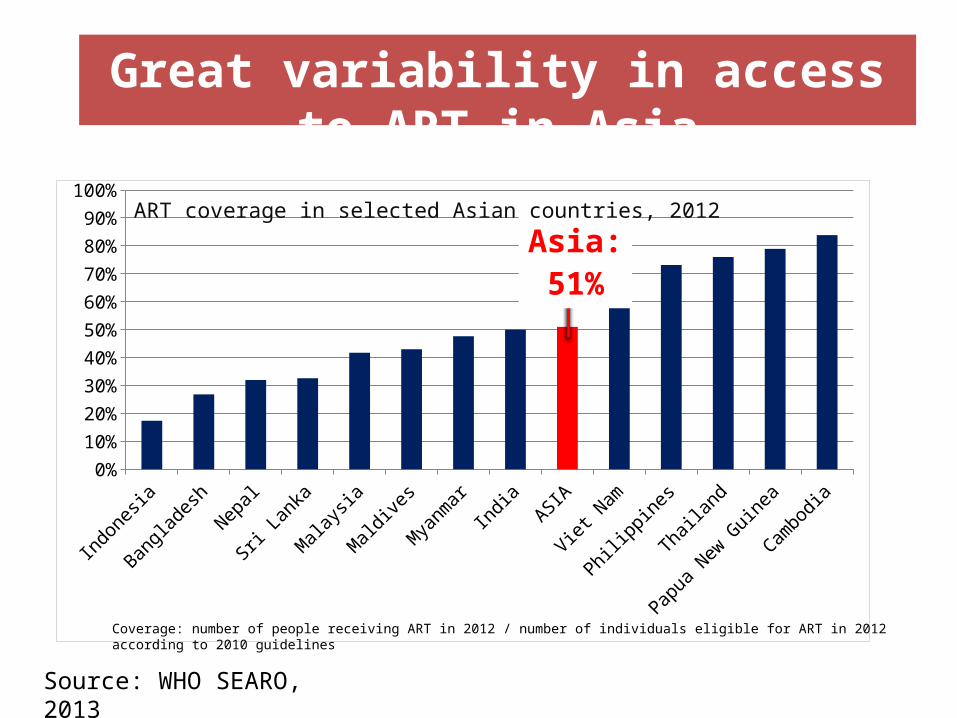
Great variability in access to ART in Asia
Indonesia
BangladeshNepal
Sri Lanka
Malaysia
Maldives
MyanmarIndia
ASIA
Viet Nam
Philippines
Thailand
Papua New Guinea
Cambodia0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Asia:51%
ART coverage in selected Asian countries, 2012
Coverage: number of people receiving ART in 2012 / number of individuals eligible for ART in 2012 according to 2010 guidelines
Source: WHO SEARO, 2013
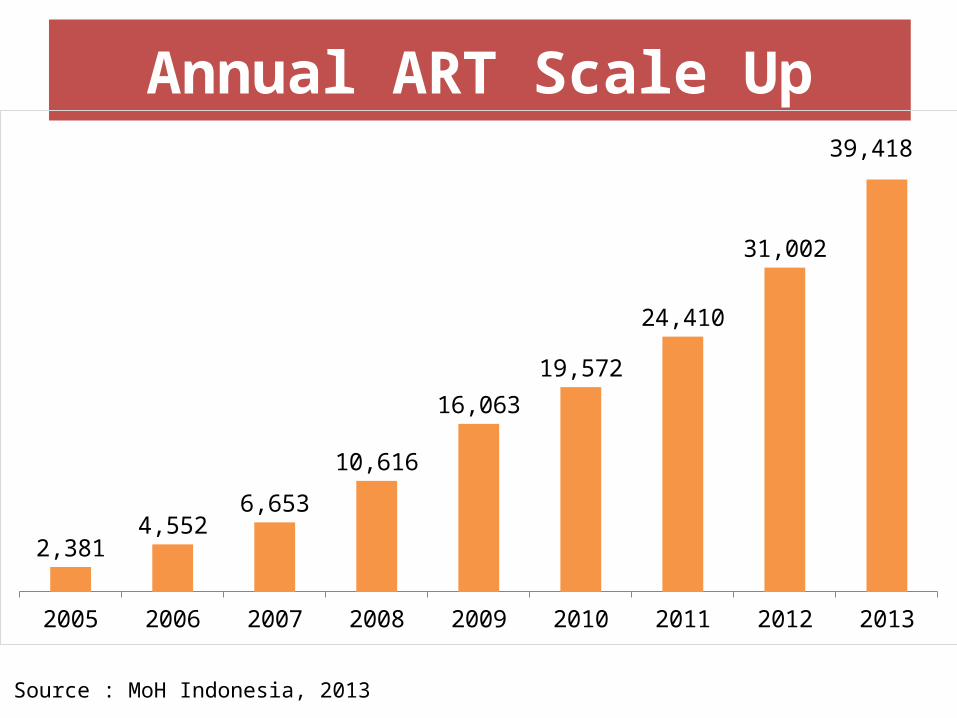
Annual ART Scale Up
2005 2006 2007 2008 2009 2010 2011 2012 2013
2,3814,552
6,653
10,616
16,063
19,572
24,410
31,002
39,418
Source : MoH Indonesia, 2013

1 July 201412 months 24 months 60 months
0
10
20
30
40
50
60
70
80
90
100
84%80%
69%MalaysiaCambodiaChinaPapua New GuineaIndonesiaWeighted av-erage
Still too many people are lost from ART: Retention at 12, 24 and 60 months
%
Source: WHO/UNAIDS
Retention rates for ART at 12, 24 and 60 months in selected countries, 2011
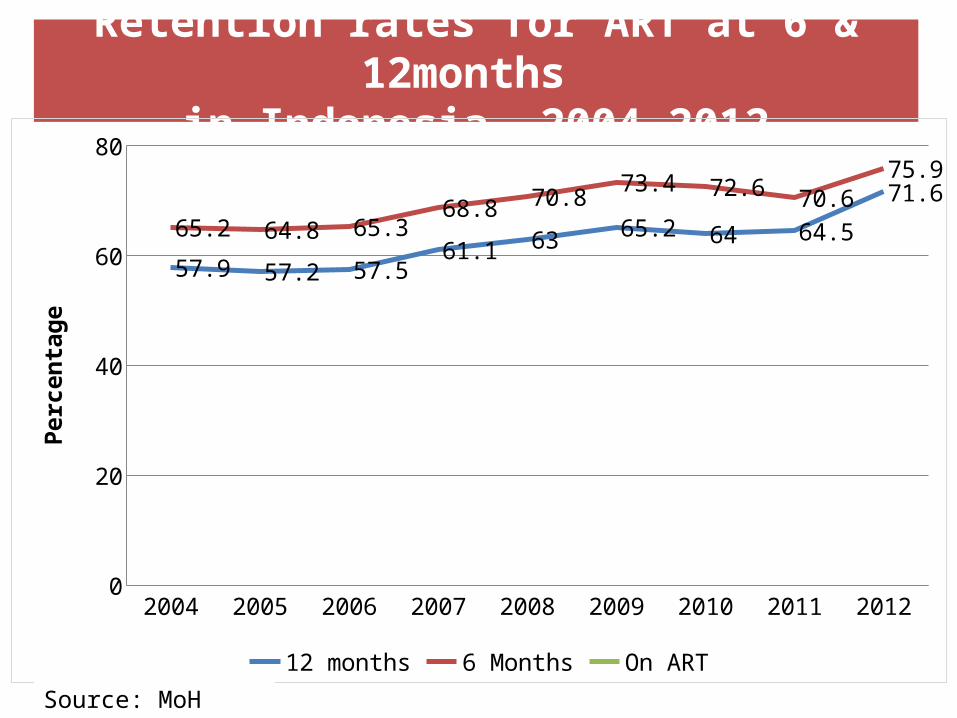
Retention rates for ART at 6 & 12months in Indonesia, 2004-2012
2004 2005 2006 2007 2008 2009 2010 2011 20120
20
40
60
80
57.9 57.2 57.561.1 63 65.2 64 64.5
71.6
65.2 64.8 65.368.8 70.8
73.4 72.6 70.675.9
12 months 6 Months On ART
Perc
enta
ge
Source: MoH 2013

1 July 2014
HIV Treatment Cascade
0
100000
200000
300000
400000
500000
600000 590000
188284141360
42411
NA NA
Source: MoH 2014

2. Rationale for Policy Formulation• Evidence of further reducing new HIV infections through “Test and Treat”
or SUFA and global move towards earlier treatment• Implementing SUFA will help accelerating coverage of ART for those most
in need• Joint rapid assessment early 2013 in collaboration among MoH, NAC,
WHO, UNAIDS and UNICEF – to obtain information for developing a roadmap to accelerate
expansion of ARVs for HIV treatment and prevention in Indonesia – To assess barriers to diagnosis and treatment– to review and learn current existing good practices – to find opportunities to further accelerate expansion and coverage of
ART • Mathematical modelling to look at the impact and effectiveness of
program that is expected from rapidly scaling-up ART in Indonesia• Followed by national consultation meeting in March 2013
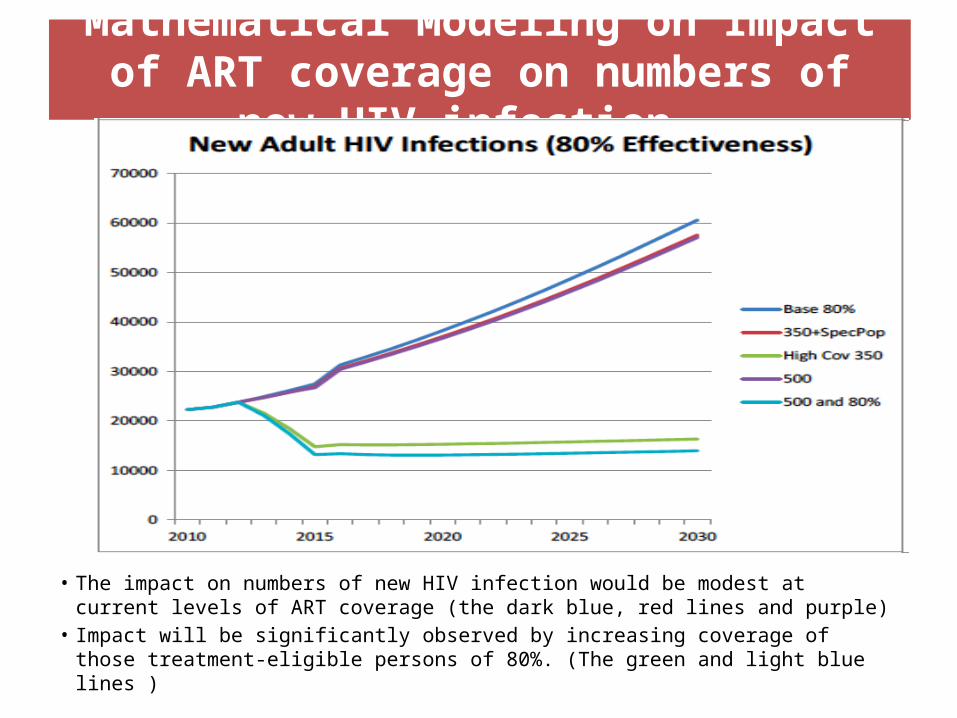
Mathematical Modeling on Impact of ART coverage on numbers of new HIV infection
• The impact on numbers of new HIV infection would be modest at current levels of ART coverage (the dark blue, red lines and purple)
• Impact will be significantly observed by increasing coverage of those treatment-eligible persons of 80%. (The green and light blue lines )

3. Policy ImplementationContinuum of Comprehensive HIV Services Framework (LKB)
• Indonesia is intensifying the response by strengthening the continuum of HIV-STI comprehensive care, a service delivery model was on going
• Addressing the prevention, care and treatment comprehensively by increased participation of all related stakeholders especially the community members at district level & HIV service available at PHC

Introduction of Strategic Use of ARVs (SUFA) through “LKB”
• Objectives:– To significantly increase HIV testing and ART coverage – To optimize the prevention impact of ARVs by offering ART
regardless of CD4 level to key affected populations and sero-discordant couples
– To strengthen the involvement and ownership by CSO groups.• Strategies
– 1. Expanding HIV diagnosis– 2. Effective enrollment and retention in HIV care– 3. Build on effective efforts that already exist, including the
LKB (CoC)
Phased Approach• Roadmap of “Rapid Scale Up of ART and Strategic Use
of ARVs (SUFA) through LKB” – 75 priority districts– phased implementation and scale-up approach
• started in 13 districts (3 from Tanah Papua and 8 from the remainder of Indonesia) in October 2013.
• rolled-out in 63 additional districts during April till December 2014.
• Minister of Health Regulation No. 21/2013– PITC approach to increase HIV test and counseling– ART regardless CD4 count to KAPs (CSW, MSM,
transgender IDUs), TB-HIV patients, Hep-HIV patients, and HIV infected pregnant women
Initiate ART when the CD4 under 350
Start ART regardless of the
CD4
Key Affected Populations: IDU, MSM, TG, SW Prisoners
Accelerating getting to Zero New Infections (and reduce mortality)

Population PN ART 2012 WHO Consolidated
ARV Guidelines 2013
SUFA
HIV+ ARV-Naïve AZT/TDF + 3TC (FTC) + EFV/NVP
TDF + 3TC (or FTC) + EFV
Priority for new patients TDF + 3TC (or FTC) +
EFV
HIV+ ARV-Naïve Pregnant Women
AZT/TDF + 3TC (FTC) + NVP/EFV
HIV/TB Co-infectionAZT/TDF + 3TC (FTC) + EFV
HIV/HBV Co-infection
TDF + 3TC (FTC) + EFV
Serodiscordant
KAPs (FSW, PWID, MSM, Transgender)
20
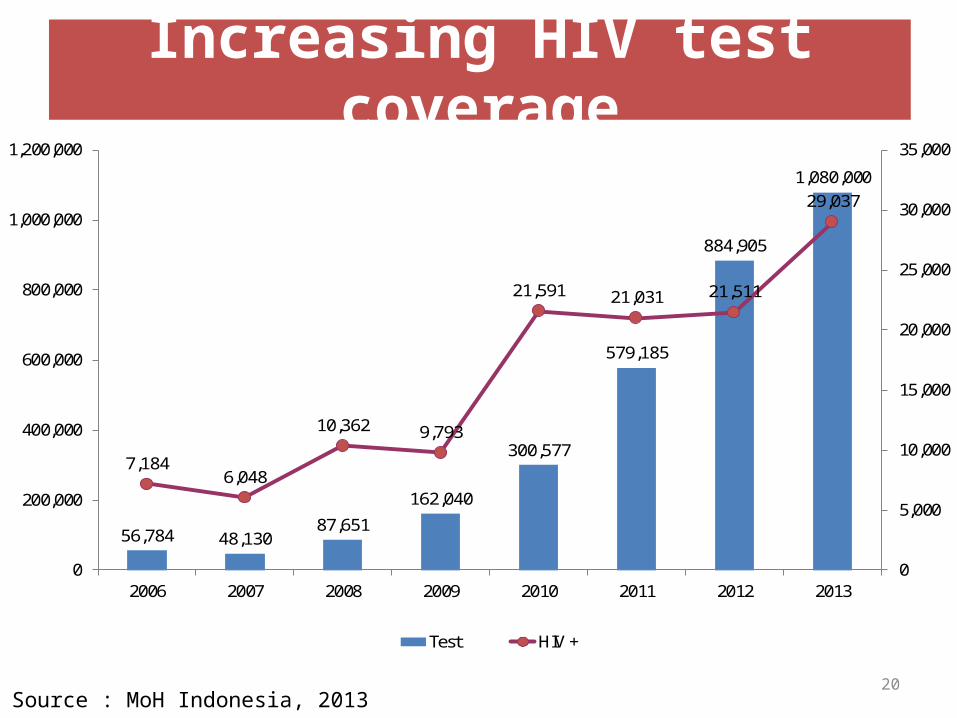
Increasing HIV test coverage
56,784 48,13087,651
162,040
300,577
579,185
884,905
1,080,000
7,1846,048
10,362 9,793
21,591 21,031 21,511
29,037
0
5,000
10,000
15,000
20,000
25,000
30,000
35,000
0
200,000
400,000
600,000
800,000
1,000,000
1,200,000
2006 2007 2008 2009 2010 2011 2012 2013
Test HIV +
Source : MoH Indonesia, 2013

4. Programmatic Questions - Challenges• For T&T as part of LKB/SUFA to have an impact in Indonesia it would
need to be accessible/acceptable and reach all key affected groups.• T&T/SUFA as in the Permenkes 21 raises programmatic questions
specially about how to improve the HIV treatment cascade:– How best to control STI ?– How best to expand HIV testing and reach those KAPs?– How bes decentralization of HIV services implemented– How best to retain them on treatment– How SUFA will affect adherence and risk behaviors?
• Effective community-based interventions involving KAPs are fundamental in the success of LKB/SUFA
• In a decentralized context local ownership by policy/decision makers is key for adoption of policy and financial sustainability

Acknowledgments
• Ms Wenita I – NAC Indonesia• Dr Oscar Barreneche – WHO Indonesia• Mr Cho Kah Sin – UNAIDS Indonesia• Dr Sri Pandam – WHO Indonesia• Dr Janto Lingga –WHO Indonesia • Ms Fetty Wijayanti –WHO Indonesia• Mr Daniel – Spiritia Foundation• USAID, DFAT, FHI 360, CHAI

TERIMA KASIH
THANK YOU