Embed Size (px)
DESCRIPTION
INTRODUCTION OF ART IN COMPREHENSIVE HIV/AIDS CARE AND SUPPORT: MONITORING AND EVALUATION. John A. Adungosi, MB Chb, MSc, MRIT. ACKNOWLEDGEMENTS. Dr. S.K. Sharif, PMO—Coast Province Dr. H. Shikely, Chief Administrator, Coast General Provincial General Hospital - PowerPoint PPT Presentation
Citation preview

INTRODUCTION OF ART IN INTRODUCTION OF ART IN COMPREHENSIVE HIV/AIDS COMPREHENSIVE HIV/AIDS
CARE AND SUPPORT:CARE AND SUPPORT:MONITORING AND MONITORING AND
EVALUATIONEVALUATIONJohn A. Adungosi, John A. Adungosi, MB Chb, MB Chb,
MSc, MRITMSc, MRIT

ACKNOWLEDGEMENTSACKNOWLEDGEMENTS• Dr. S.K. Sharif, PMO—Coast ProvinceDr. S.K. Sharif, PMO—Coast Province• Dr. H. Shikely, Chief Administrator, Coast General Dr. H. Shikely, Chief Administrator, Coast General
Provincial General HospitalProvincial General Hospital• Staff of CPGH, Port Reitz District Hospital, Mkomani-Staff of CPGH, Port Reitz District Hospital, Mkomani-
Bomu Medical Centre and Magongo Health CentreBomu Medical Centre and Magongo Health Centre• USAIDUSAID• Technical Advisory Partners:Technical Advisory Partners:
– Family Health InternationalFamily Health International– MSH/RPM PlusMSH/RPM Plus– Population Council/HORIZONSPopulation Council/HORIZONS

Purpose of HIV/AIDS care treatment Purpose of HIV/AIDS care treatment and support programmes:and support programmes:
• To reduce morbidity and mortality from HIV/AIDS and related To reduce morbidity and mortality from HIV/AIDS and related complications.complications.
• To improve the quality of life of adults and children living with To improve the quality of life of adults and children living with HIV/AIDS and their families.HIV/AIDS and their families.
• To assure equitable access to diagnosis, medical care, To assure equitable access to diagnosis, medical care, pharmaceuticals, and supportive care.pharmaceuticals, and supportive care.
• To promote prevention opportunities within care and support To promote prevention opportunities within care and support service delivery.service delivery.

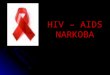
PEOPLE AND FAMILIES
AFFECTED BY HIV/AIDS
Human Rights and Legal Supporte.g.: •PLHA participation•Stigma & discrimination reduction•Succession planning
Socioeconomic Supporte.g.:•Material support•Economic security•Food support
Medical & NursingCaree.g.:•VCT, Family Planning•Preventive therapy•OI treatment and HAART•Palliative care
Psychosocial Supporte.g.:•Counseling•Spiritual support•Follow-up counseling•Community support
Elements of Comprehensive Care and Support

BackgroundBackgroundWhy did the ART program start?Why did the ART program start?
1.1. Availability of HAART in Kenya: from mid-Availability of HAART in Kenya: from mid-90s in private hospitals90s in private hospitals
2.2. Prohibitive cost of treatment amidst Prohibitive cost of treatment amidst intense public interestintense public interest
3.3. Government responses to improve accessGovernment responses to improve access4.4. Increasing availability of ARV drugs due to Increasing availability of ARV drugs due to
progressive reduction in prices and progressive reduction in prices and initiatives to improve accessinitiatives to improve access

Background (2)Background (2)5.5. National consultative meeting on ARTNational consultative meeting on ART
– Convened by IMPACT in Sept. 2001Convened by IMPACT in Sept. 2001– Involved local and international Involved local and international
stakeholders, donors, researchers, PLHA and stakeholders, donors, researchers, PLHA and community groups community groups
– The purpose was to review the ART situation The purpose was to review the ART situation in Kenya and chart the way forwardin Kenya and chart the way forward
– The result was the setting up of a National The result was the setting up of a National ART Task ForceART Task Force

Background (3)Background (3)• National ART task forceNational ART task force
– Composed of local and international stakeholders, Composed of local and international stakeholders, community groups, PLHA, professional community groups, PLHA, professional associations,donors and development agencies associations,donors and development agencies
– Acts as an advisory board to the NASCOP and Director of Acts as an advisory board to the NASCOP and Director of Medical ServicesMedical Services
– Has many sub committees (Drugs, training, Systems Has many sub committees (Drugs, training, Systems developmentdevelopment
– Provides platform for sharing experiences on ART Provides platform for sharing experiences on ART implementationimplementation

National Adult HIV Prevalence: 10.2%
Project Site: Coastal city of Mombasa
Health Facilities1. Coast General Provincial Hospital: 700-bed
tertiary referral hospital with >70% of beds occupied by HIV/AIDS patients.
2. Port Reitz District Hospital: Government referral hospital.
3. Mkomani Bomu Clinic: Semi-private primary health care clinic.
4. Magongo Health Center: Local government primary health care clinic.
Site Information: KenyaSite Information: Kenya

Where is the program Where is the program implemented?implemented?
Mombasa: Rationale for Site Selection (1)Mombasa: Rationale for Site Selection (1)High HIV prevalence and disease burdenHigh HIV prevalence and disease burdenSites provide the opportunity to introduce ART at Sites provide the opportunity to introduce ART at
different levels of health care services as well as different levels of health care services as well as multiple entry points to ART services within the multiple entry points to ART services within the same catchment areasame catchment area
Sites are linked through a referral network Sites are linked through a referral network system and to some services that provide system and to some services that provide elements of comprehensive care and supportelements of comprehensive care and support

• Rationale for Site Selection (2):Rationale for Site Selection (2):– USAID supported programs in Mombasa provide USAID supported programs in Mombasa provide
elements of comprehensive care and supportelements of comprehensive care and support• IMPACT: Prevention activities (BCC, STI IMPACT: Prevention activities (BCC, STI
management) & care activities (VCT, management management) & care activities (VCT, management of OI, psychological support to PLHA)of OI, psychological support to PLHA)
•COPHIA: Home-based care activitiesCOPHIA: Home-based care activities•PSI: Condom promotionPSI: Condom promotion•Strong political commitmentStrong political commitment
Where is the program Where is the program implemented?implemented?

How is the program How is the program implemented?implemented?
1.1. Establish the Technical Advisory Partners Establish the Technical Advisory Partners and define the role of each partner:and define the role of each partner:– Partners’ rolesPartners’ roles
• FHI/IMPACT: overall implementation and M&E FHI/IMPACT: overall implementation and M&E
• MSH/RPM Plus: strengthening drug and commodity MSH/RPM Plus: strengthening drug and commodity managementmanagement
• Population Council/Horizons: conducting operational Population Council/Horizons: conducting operational research related to the introduction of ART programresearch related to the introduction of ART program

How is the program How is the program implemented?implemented?2.2. Develop a concept paper describing the Develop a concept paper describing the
implementation of the programimplementation of the program3.3. Convene a workshop with local Convene a workshop with local
stakeholders to discuss the concept paperstakeholders to discuss the concept paper• The TAP described the ART ProgramThe TAP described the ART Program• Local stakeholders provided Local stakeholders provided
recommendations on key programmatic recommendations on key programmatic issues and the framework for the programissues and the framework for the program
• Local stakeholders provided their Local stakeholders provided their commitment to support and promote the commitment to support and promote the programprogram

How is the program How is the program implemented?implemented?4.4. Establish the ART program management Establish the ART program management
structurestructure• Steering Committee:Steering Committee:
o Composition:Composition: LLocal stakeholdersocal stakeholderso Responsibility:Responsibility: Overseeing program implementation Overseeing program implementation
• Scientific Committee: Scientific Committee: o Composition:Composition: Local and international Local and international
researchers and researchers and scientistsscientistso Responsibility:Responsibility: Developing realistic minimum Developing realistic minimum
package package of activities (e.g eligibility criteria, of activities (e.g eligibility criteria, Rx Rx treatment monitoring schedules)treatment monitoring schedules)

How is the program How is the program implemented?implemented?4.4. Establish the ART program management structureEstablish the ART program management structure
• Operational Management teamOperational Management team::o Composition: Composition: Program coordinator, ART site team Program coordinator, ART site team
leader, partners’ field officersleader, partners’ field officerso Responsibility: DResponsibility: Daily management of the programaily management of the program
• Technical Advisory PartnerTechnical Advisory Partner: : o Composition:Composition: RPM Plus, Horizons, IMPACT, USAIDRPM Plus, Horizons, IMPACT, USAIDo Responsibility:Responsibility: Providing technical support to the Providing technical support to the
program and the different committeesprogram and the different committees

How is the programHow is the program implementedimplemented??
5.5. Conduct assessment of existing Conduct assessment of existing capacity for implementing HIV care capacity for implementing HIV care program including ART program including ART
6.6. Strengthen the capacity based on the Strengthen the capacity based on the findings from the assessmentfindings from the assessment
7.7. Develop implementation plansDevelop implementation plans8.8. Execute, monitor and evaluate the Execute, monitor and evaluate the
implementationimplementation

What have we done so far?What have we done so far?
1.1. All committees have been establishedAll committees have been established– Scientific Committee has defined eligibility criteria Scientific Committee has defined eligibility criteria
and treatment monitoring schedule, Steering and treatment monitoring schedule, Steering Committee approvedCommittee approved
2.2. Assessment of existing capacity was conductedAssessment of existing capacity was conducted
3.3. Based on findings from the assessment, an Based on findings from the assessment, an implementation plan was developed with each implementation plan was developed with each facilityfacility

What have we done so far? (2)What have we done so far? (2)• The capacity of the CPGH has been The capacity of the CPGH has been
strengthened:strengthened: – Training of 37 clinicians, pharmacists and Training of 37 clinicians, pharmacists and
laboratory staff was completed in April, 2003;laboratory staff was completed in April, 2003;– Standard Operating Procedures and clinical data Standard Operating Procedures and clinical data
collection tools are in place; collection tools are in place; – Procurement of laboratory equipment is underway Procurement of laboratory equipment is underway
(CD4 instrument); (CD4 instrument); – Drug storage and security at pharmacy have been Drug storage and security at pharmacy have been
developed;developed;– Nurse adherence counselors were trained in Nurse adherence counselors were trained in
adherence monitoringadherence monitoring..

What have we done so far? (3)What have we done so far? (3)• The CPGH Comprehensive HIV Care The CPGH Comprehensive HIV Care
Center is operational, providing HIV Center is operational, providing HIV clinical services, ART, nutritional clinical services, ART, nutritional counseling, TB, STI, and referral to counseling, TB, STI, and referral to home care, inpatient services, MCH/ANC, home care, inpatient services, MCH/ANC, PMTCT, and the Pediatric Clinic.PMTCT, and the Pediatric Clinic.
• On May 23, 2003, patients started ART On May 23, 2003, patients started ART in accordance with eligibility criteria.in accordance with eligibility criteria.

PATIENT DATAPATIENT DATA
• The Comprehensive HIV Care Centre:The Comprehensive HIV Care Centre:– Began clinical care on April 17, 2003Began clinical care on April 17, 2003– number of HIV infected patients number of HIV infected patients
followed:followed:• FemaleFemale• MaleMaleWHO Clinical Staging:WHO Clinical Staging:
– IIII– IIIIII– IVIV

PATIENT DATA (2)PATIENT DATA (2)
• The First Month of ART at CPGH:The First Month of ART at CPGH:– Total: HIV Care- 123; ART 11Total: HIV Care- 123; ART 11– Gender-- =Female/ MaleGender-- =Female/ Male– Range of CD4 counts—03-201Range of CD4 counts—03-201– Adherence counseling—all patients participated Adherence counseling—all patients participated
in a minimum of 3 mandatory adherence in a minimum of 3 mandatory adherence counseling sessions prior to starting ARVscounseling sessions prior to starting ARVs
– Response to ARVs:Response to ARVs: • Incidence of adverse symptoms—Incidence of adverse symptoms—

MONITORING AND EVALUATIONMONITORING AND EVALUATION• Objectives:Objectives:1.1. To improve the capacity of HIV/AIDS clinics, To improve the capacity of HIV/AIDS clinics,
laboratory and pharmacy services in selected public laboratory and pharmacy services in selected public health facilities in Mombasa to support the health facilities in Mombasa to support the introduction of comprehensive care including ARTintroduction of comprehensive care including ART
2.2. To provide ART to 300 patients over a period of five To provide ART to 300 patients over a period of five years in accordance with eligibility criteriayears in accordance with eligibility criteria
3.3. To sensitize and strengthen communities and PLHA To sensitize and strengthen communities and PLHA support groups in HIV/AIDS comprehensive care, support groups in HIV/AIDS comprehensive care, including ARTincluding ART
4.4. To explore Operations Research Questions (e.g., To explore Operations Research Questions (e.g., What is the effect of DAART upon ARV adherence?)What is the effect of DAART upon ARV adherence?)

FORMATIVE ASSESSMENT DATA FORMATIVE ASSESSMENT DATA COLLECTION TOOLSCOLLECTION TOOLS
• Needs Assessment Tool:Needs Assessment Tool:--National Clinical Guidelines--National Clinical Guidelines--Physical infrastructure--Physical infrastructure
•Laboratory servicesLaboratory services•PharmacyPharmacy--Human resources and staff capacity--Human resources and staff capacity
--Clinical services and referral mechanism--Clinical services and referral mechanism--HIV diagnosis--HIV diagnosis--ARV management--ARV management--Management Information Systems--Management Information Systems--Cost Issues--Cost Issues

STANDARD OPERATING STANDARD OPERATING PROCEDURESPROCEDURES
• Clinical Care and Patient FlowClinical Care and Patient Flow– Adult and PaediatricAdult and Paediatric
• Post-exposure prophylaxisPost-exposure prophylaxis• Drug and Commodity ManagementDrug and Commodity Management• Laboratory and Other InvestigationsLaboratory and Other Investigations

DATA COLLECTION TOOLS (2)DATA COLLECTION TOOLS (2)
• Patient Clinical Monitoring Forms:Patient Clinical Monitoring Forms:--Comprehensive Care Centre Registration Form--Comprehensive Care Centre Registration Form--Nursing Assessment for Triage Form--Nursing Assessment for Triage Form--Clinical Management of HIV Patients: First Visit--Clinical Management of HIV Patients: First Visit--Follow-Up Review of HIV Patients--Follow-Up Review of HIV Patients--Enrollment Form for Adult ARV Treatment--Enrollment Form for Adult ARV Treatment--Medical Follow-up of Adult Patients on ART--Medical Follow-up of Adult Patients on ART--Referral System Form--Referral System Form--Clinic Attendance and Treatment Follow-Up --Clinic Attendance and Treatment Follow-Up RegisterRegister

MONITORING AND MONITORING AND EVALUATION (3)EVALUATION (3) Indicator Categories:Indicator Categories:
Clinical/biological outcomesClinical/biological outcomesARV treatment adherenceARV treatment adherenceOccurrence of adverse drug effectsOccurrence of adverse drug effectsOccurrence of OIs, including TBOccurrence of OIs, including TBDrug management and inventory controlDrug management and inventory controlLaboratory monitoring and equipment utilizationLaboratory monitoring and equipment utilizationReferral for community based services, including home Referral for community based services, including home care and psychosocial supportcare and psychosocial supportTraining and refresher coursesTraining and refresher coursesImpact of community outreach on stigma and treatment Impact of community outreach on stigma and treatment seekingseeking

MOMBASA PROJECT: M&E PLAN MOMBASA PROJECT: M&E PLAN SAMPLESAMPLE
Specific Objective 2: To provide ART to 300 patients over a period of five years in accordance with eligibility criteria
Indicators Activities/resources
Outputs
Long term outcomes (impact)
Definition (key indicators)
Sources of data and methods
Periodicity of collection
Responsible
Sub-Objective 2.1: Develop and implement client monitoring system including development of adherence system Develop clients monitoring system including development of adherence system
Client monitoring and adherence system developed
Forms for clients monitoring
FHI and MOH staff
# and % of clients referred eligible for ART
Numerator: # of HIV + clients who attended the sites and who are eligible according to criteria upon agreed by the steering committee/local guidance Denominator: total # of HIV+ clients who attending the sites in a given period
Clinic records Sites monitoring reports
Regular basis Quarterly reports Annual reports
Clinic staff M&E officer
Implement client Monitoring system including adherence
# of clients who started ART and adhere to treatment
% of clients who demonstrate 95% adherence to treatment
Numerator: # of clients who show 95% adherence to ARV therapy during the life of the project Denominator: total # of clients enrolled at the start of the project
Clients records Sites reports
Regular-basis but to be compiled every quarter

NEXT STEPSNEXT STEPS• Scale-up project at 3 satellite sites in MombasaScale-up project at 3 satellite sites in Mombasa• Progressively develop computer-based data Progressively develop computer-based data
entry system at each siteentry system at each site• November 2003: completion of 6 months of November 2003: completion of 6 months of
ART at CPGHART at CPGH– Collect, analyze and report on key findingsCollect, analyze and report on key findings– Document lessons learned from start-up of Document lessons learned from start-up of
ART projectART project– Disseminate data and conclusions to key Disseminate data and conclusions to key
stakeholders and service providers stakeholders and service providers