Embed Size (px)
Citation preview
Natural Killer/T-Cell LymphomaIntroduction of Anemia
Ting LiuDepartment of Internal Medicine
2017. 3.
Definition of Anemia
The term of Anemia is functionally defined as an
insufficient RBC mass to adequately deliver
oxygen to peripheral tissues
For practical purposes, any of the three
measures ( Hb, Hct, and RBC ) may be used to
establish the presence of anemia, but the
hemoglobin concentration is often preferred
Anemia is not a disease but a manifestation of
many diseases
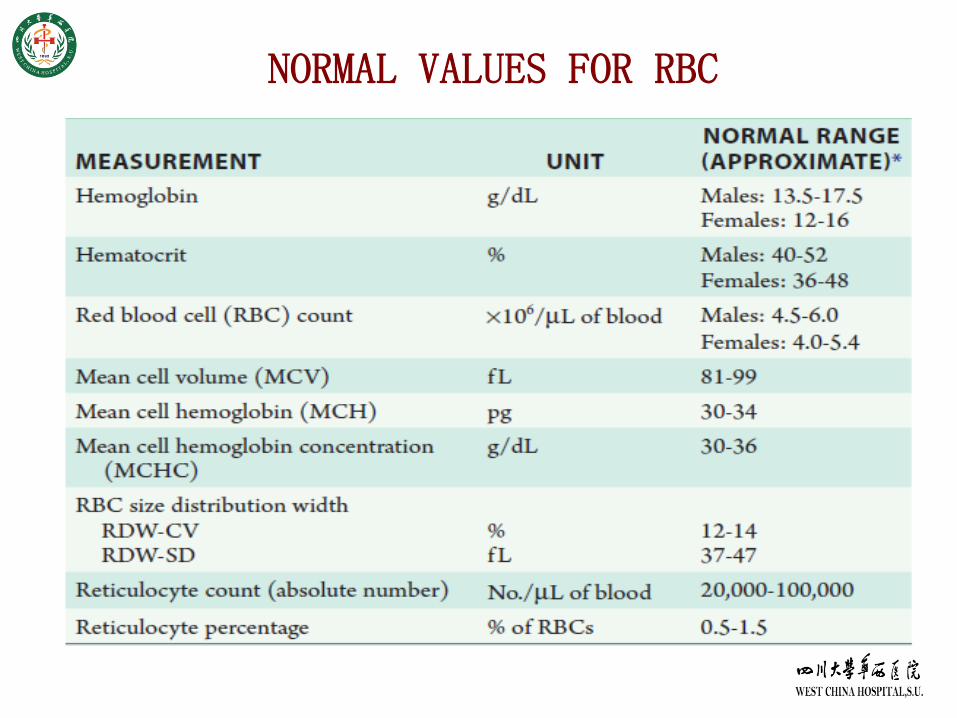
NORMAL VALUES FOR RBC
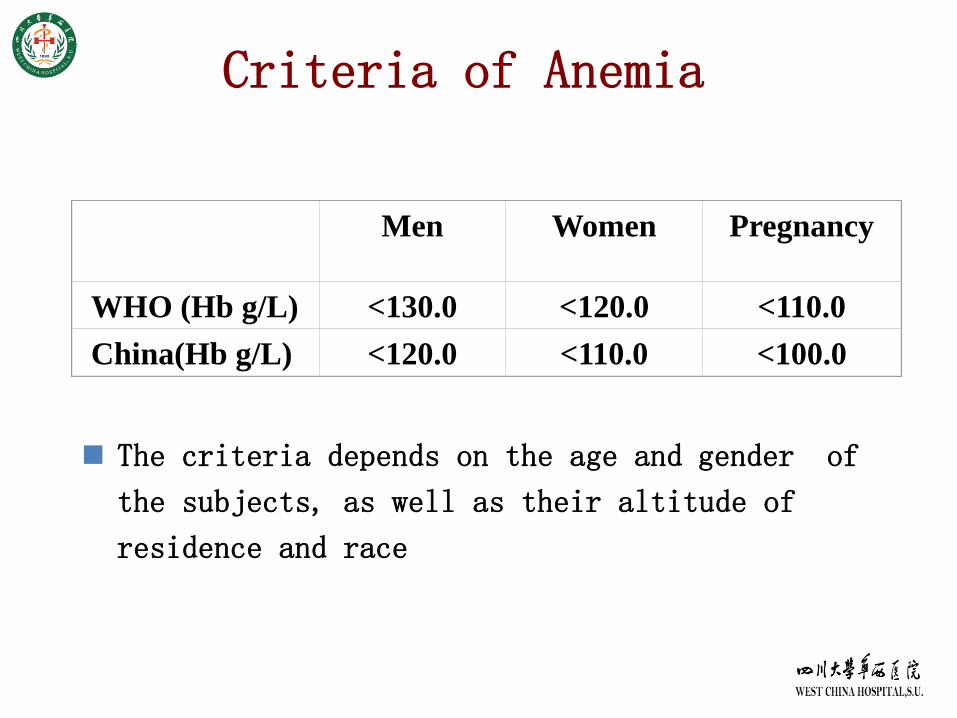
Criteria of Anemia
The criteria depends on the age and gender of
the subjects, as well as their altitude of
residence and race
Men Women Pregnancy
WHO (Hb g/L) <130.0 <120.0 <110.0
China(Hb g/L) <120.0 <110.0 <100.0
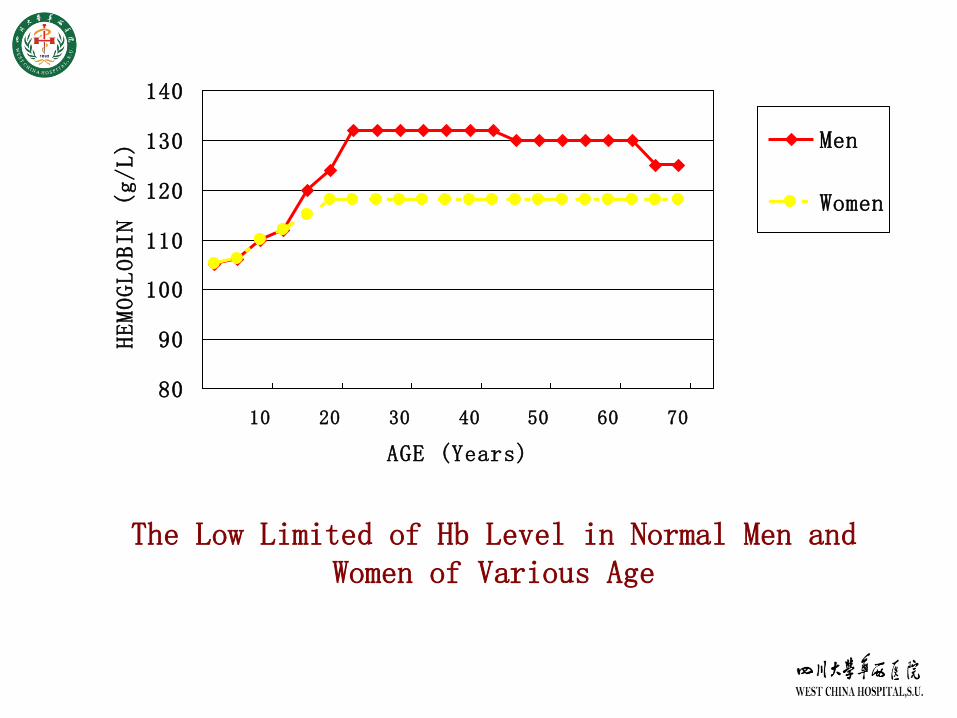
The Low Limited of Hb Level in Normal Men and Women of Various Age
80
90
100
110
120
130
140
10 20 30 40 50 60 70
AGE (Years)
HEMOGLOBIN (g/L) Men
Women
The injury of progenitor of erythrocyte:
physical, chemical, biological factors
The lack of hematopoietic factors:
ferritin,vitB12, folic acid,vitB6
The damage of bone marrow tissues:
leukemia, lymphoma,solid tumor infiltrate
Increase of red blood cell destruction & loss:
hereditary and acquied hemolytic anemia
bleeding
Causes and Mechanisms of Anemia
Classification of Anemia
According to the causes and mechanisms of anemia
types:
Decrease of red blood cell production:
AA, IDA, leukemia
Increase of red blood cell destruction:
hemolytic anemia
Acute or chronic blood loss, GI tumor, ulcer,
hypermenorrhea, hemorrhoea
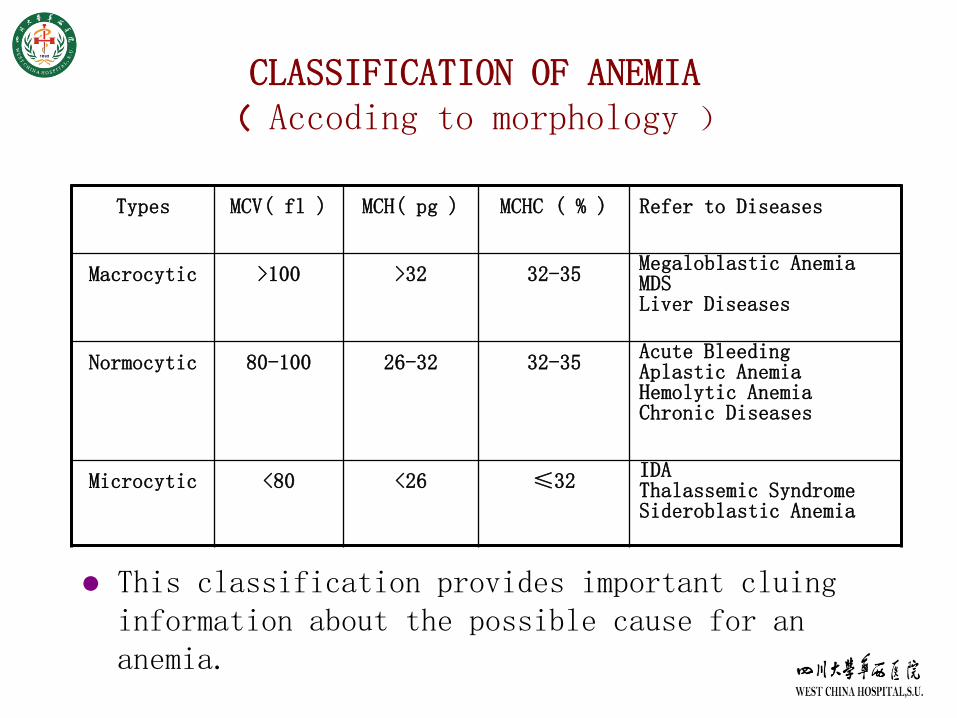
CLASSIFICATION OF ANEMIA( Accoding to morphology )
Types MCV( fl ) MCH( pg ) MCHC ( % ) Refer to Diseases
Macrocytic >100 >32 32-35Megaloblastic AnemiaMDSLiver Diseases
Normocytic 80-100 26-32 32-35Acute BleedingAplastic AnemiaHemolytic AnemiaChronic Diseases
Microcytic <80 <26 ≤32IDAThalassemic SyndromeSideroblastic Anemia
This classification provides important cluing information about the possible cause for an anemia.
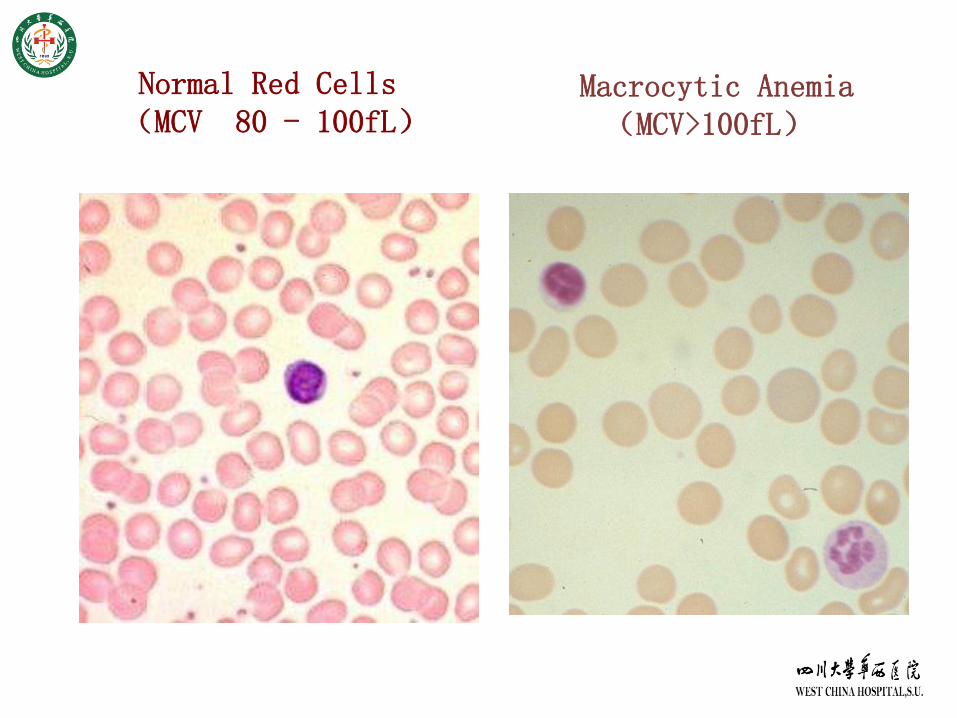
Normal Red Cells(MCV 80 - 100fL)
Macrocytic Anemia(MCV>100fL)
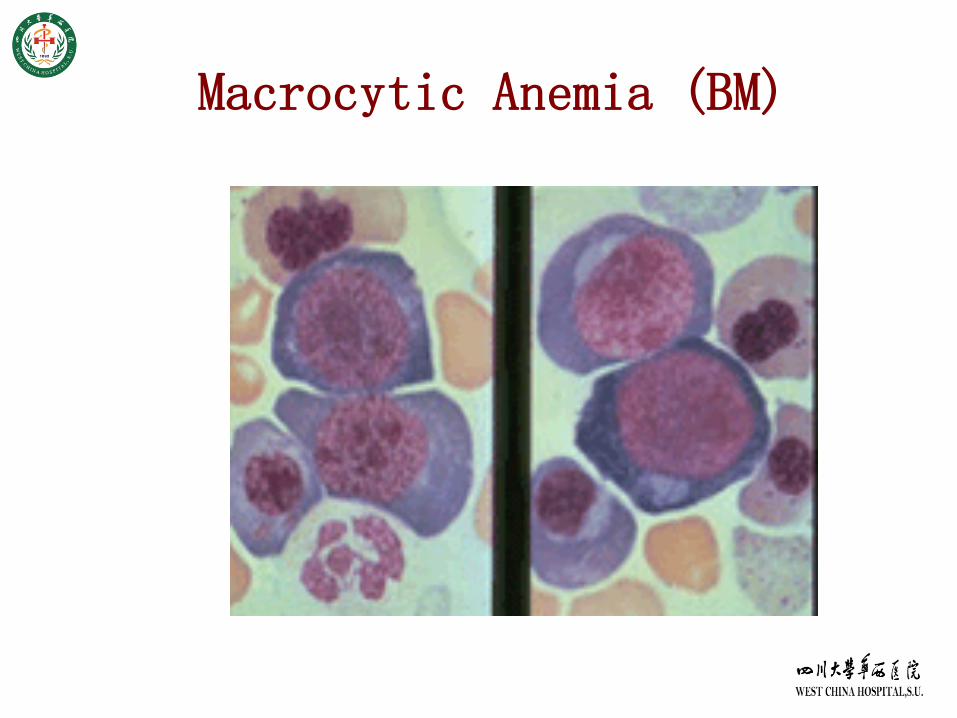
Macrocytic Anemia (BM)
Macrocytic Anemia
MCV>100 fL
Increased MCV is a normal characteristic of reticulocytes
Abnormal DNA synthesis
Folate, B12 deficiency
Abnormal RBC maturation
MDS, leukemia
Alcohol abuse
Liver disease
Hypothyroidism
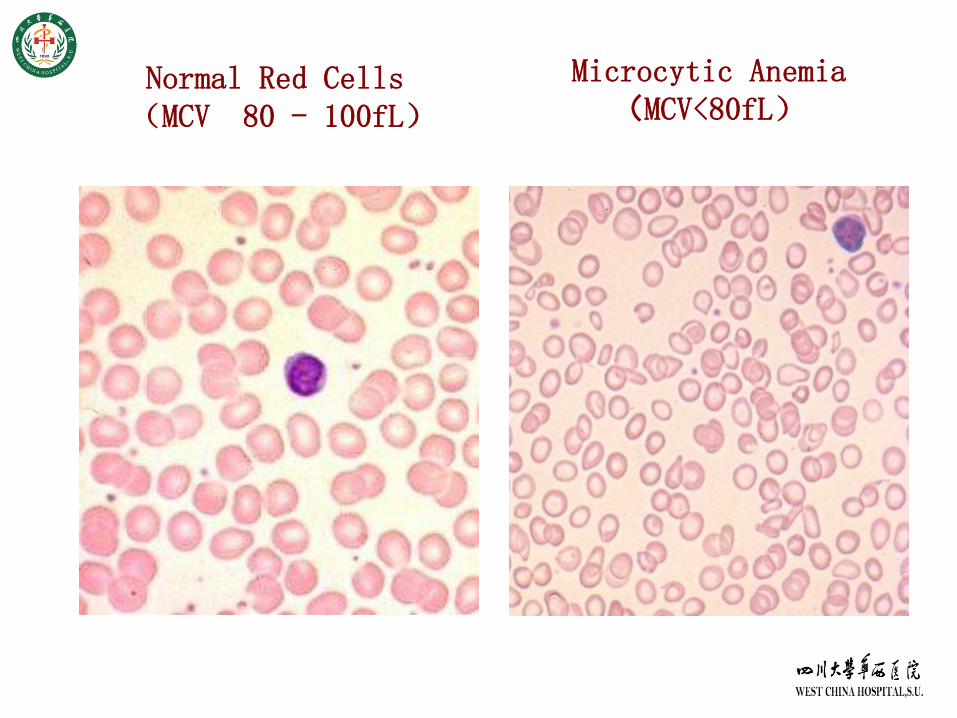
Microcytic Anemia(MCV<80fL)
Normal Red Cells(MCV 80 - 100fL)
Microcytic Anemia
MCV<80 fL
Usually hypochromic as well
Reduced iron availability
Iron deficiency
Anemia of chronic disease
Reduced heme synthesis
Lead poisoning
Reduced globin production
Thalassemia, other hemoglobinopathies
Normocytic Anemia with Low Reticulocyte Count
Decreased stimulation of bone marrow Anemia of chronic disease
Chronic renal insufficiency
Metabolic disorders
Isolated decrease in RBC precursors Pure red cell aplastic anemia
Bone marrow damage Fibrosis
Stem cell damage
Infiltration with tumor/infection
Myelodysplasia/sideroblastic anemia
Normocytic Anemia with High Reticulocyte Count
High reticulocyte count may lead to macrocytosis
Hemolysis is the most common reason with
Jaundice, cholelithiasis
Risk of aplastic crisis (Parvovirus B19)
Classification
Hereditary vs. acquired
Extravascular vs. intravascular
Immune vs.non-immune
Bleeding
Mild to moderate elevations (3 to 7%) encountered in myelophthisic anemia
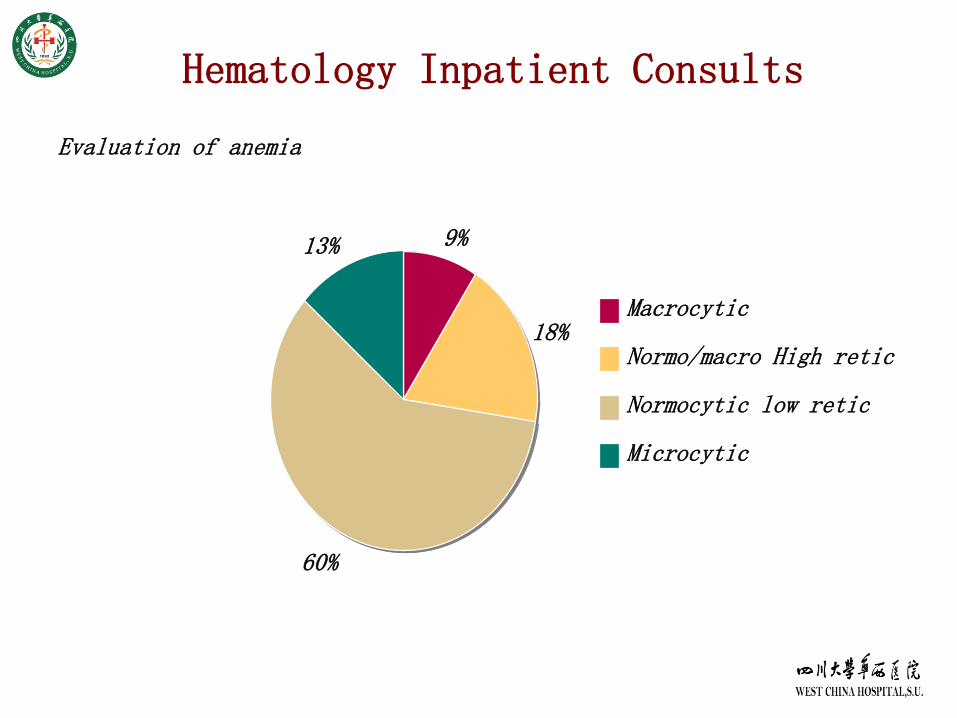
Hematology Inpatient Consults
9%
18%
60%
13%
Macrocytic
Normo/macro High retic
Normocytic low retic
Microcytic
Evaluation of anemia
Clinic Features of Anemia
SYMPTOMS
Fatigue
Headaches
Faintness
Breathlessness
Angina
Intermittent claudicating
Palpitation
Clinic Features of Anemia
SIGNS
Pallor
Tachycardia
Systolic murmur
Cardiac failure
Papilloedema-retinal hemorrhage (rare)
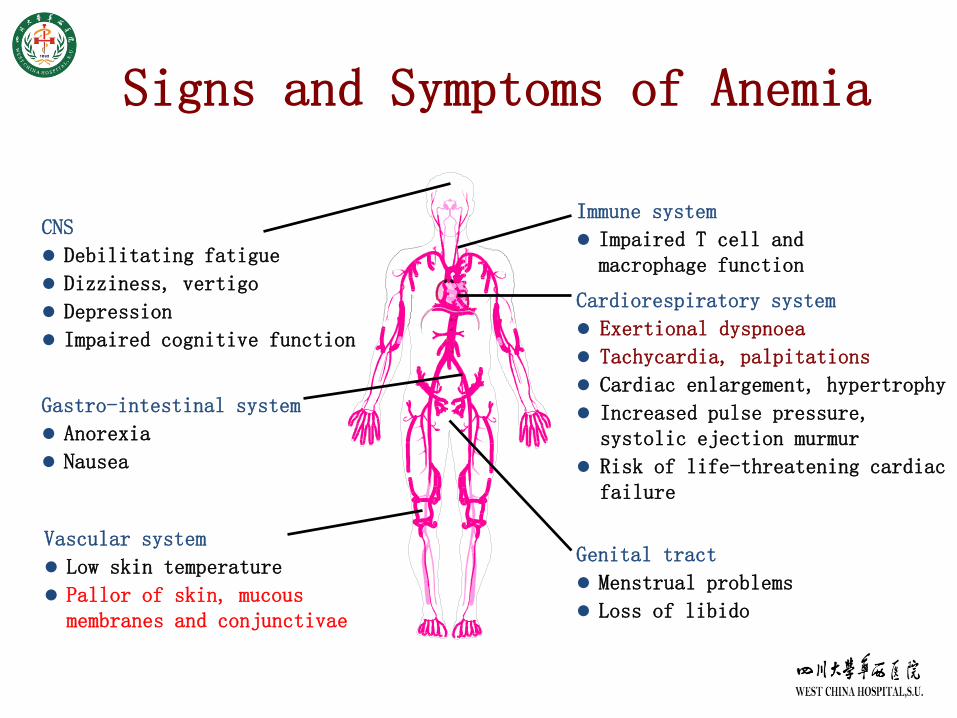
Signs and Symptoms of Anemia
CNS
Debilitating fatigue
Dizziness, vertigo
Depression
Impaired cognitive function
Immune system
Impaired T cell and macrophage function
Cardiorespiratory system
Exertional dyspnoea
Tachycardia, palpitations
Cardiac enlargement, hypertrophy
Increased pulse pressure, systolic ejection murmur
Risk of life-threatening cardiac failure
Gastro-intestinal system
Anorexia
Nausea
Genital tract
Menstrual problems
Loss of libido
Vascular system
Low skin temperature
Pallor of skin, mucous membranes and conjunctivae
Factors Influencing Symptoms of Anemia
The rapidity of onset and severity of anemia
The ability of patients to make cardiovascular
compensations
Age: old person with severe symptoms
Sex: female with severe symptoms
Diagnosis
History: Nutrition,Reproduction,Bleeding,Drugs,
Occupation, Family History, Underlying
disease
Physical Examination: Skin, Eye ground, Mouth,
Heart, Abdomen, Lymph nodes, Nervous System
RBC Indices: Blood Smear, CBC, Ret. MCV, MCHC
History Taking in Anemia
What is the complaint
Duration
Age of onset
History of bleeding disorder
Family history of bleeding disorder
Family history of anemia
History of recent bleed
History of menorrhagia
History Taking in Anemia
Is anemia episodic
History of drug intake
Dietary habits
History of worm infestation
Abdominal complaints
History of fever
History of swelling in the neck/axila/groin
Examination of Anemic Patient
Demeanor
Dyspnoea
Pallor
Jaundice
Glositis/stomatitis
Shape of skull
Lymph nodes palpable
Hepatomegaly
Splenomegaly
Leg ulcers
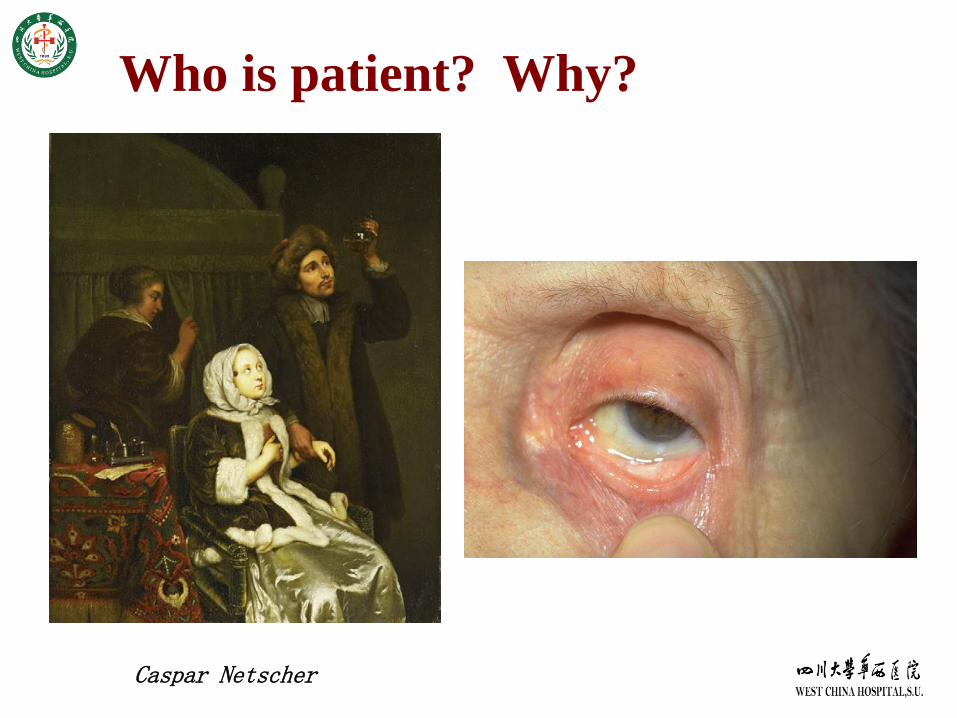
Who is patient? Why?
Caspar Netscher
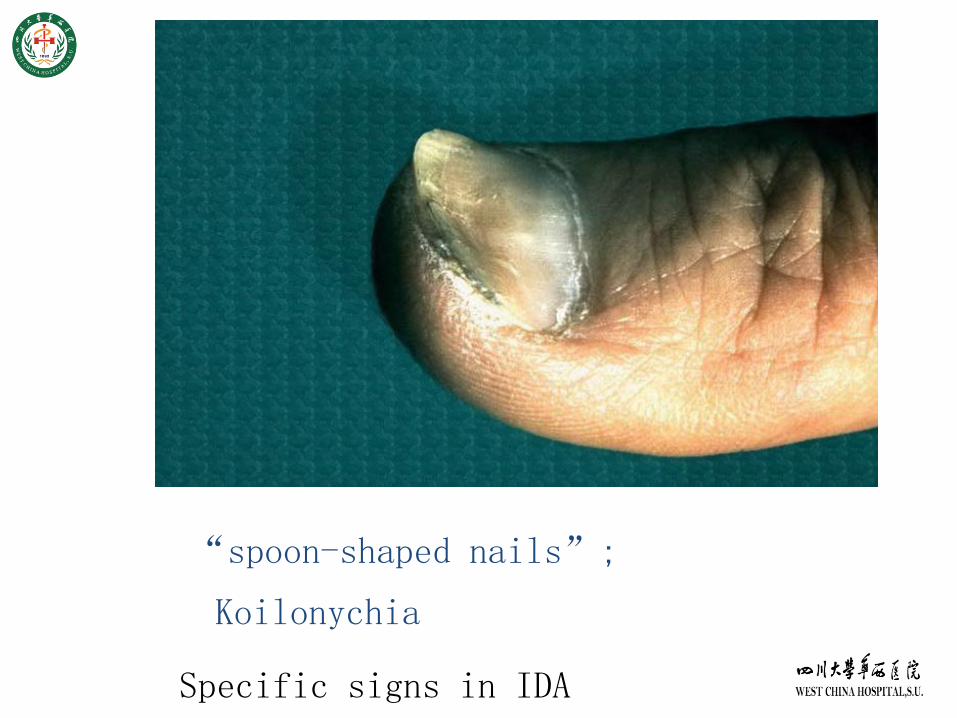
“spoon-shaped nails”;
Koilonychia
Specific signs in IDA
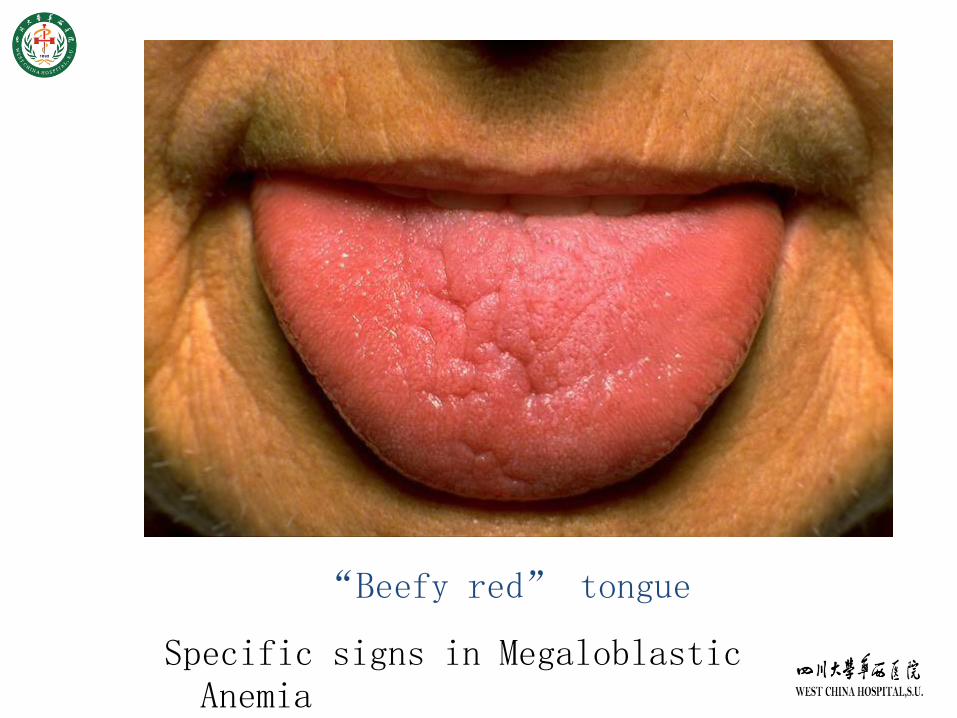
“Beefy red” tongue
Specific signs in Megaloblastic Anemia

“mirror tongue”
Specific signs in megaloblastic anemia
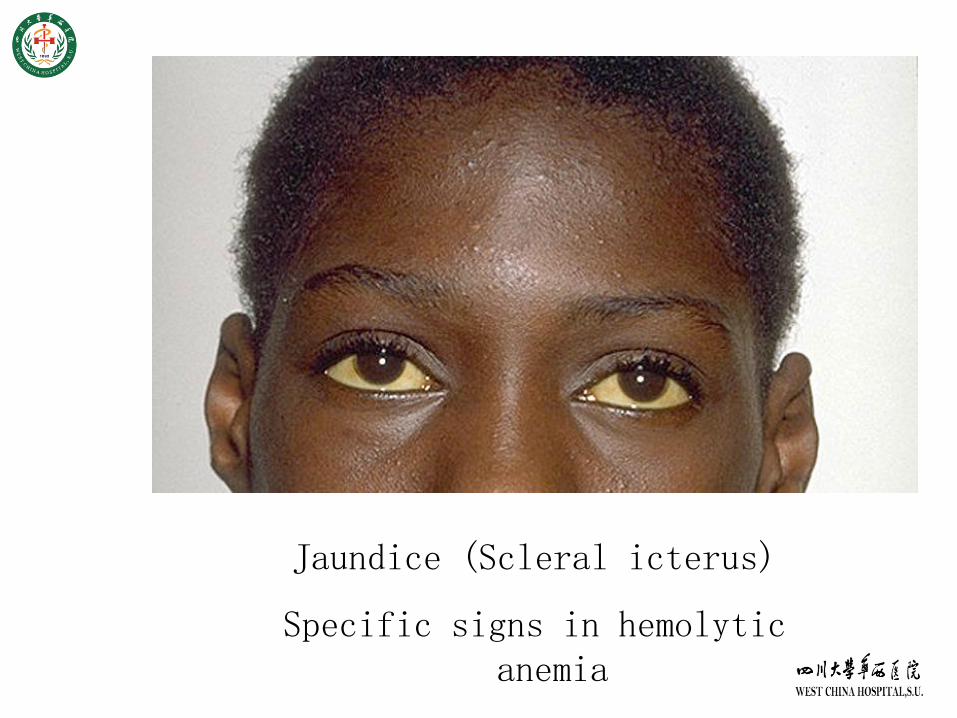
Jaundice (Scleral icterus)
Specific signs in hemolytic anemia
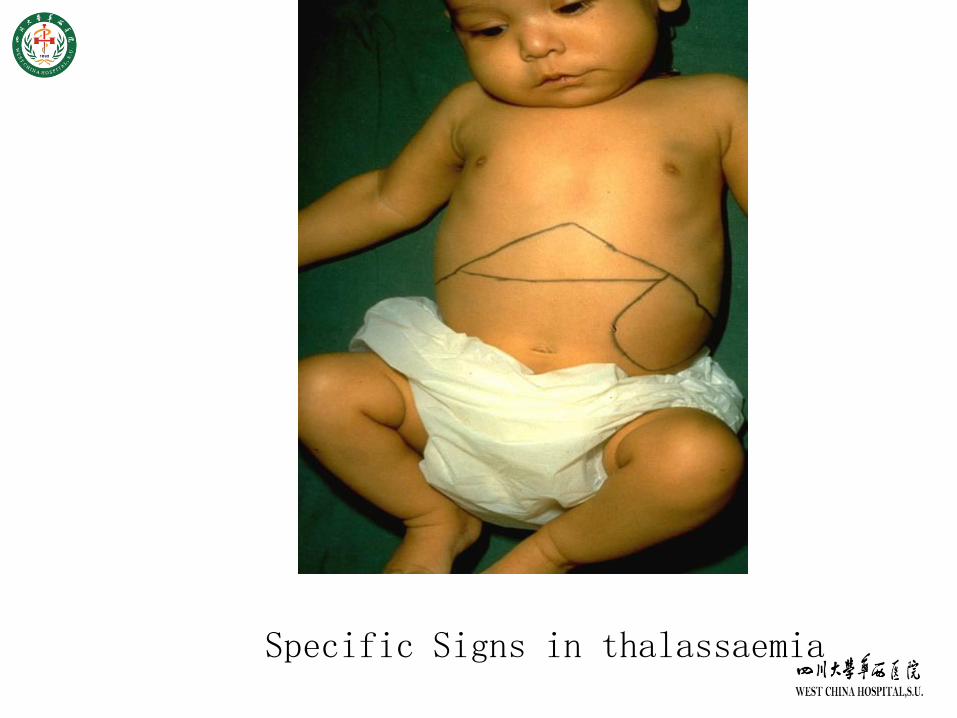
Specific Signs in thalassaemia
Lab. Investigations
Begin with
Complete blood count (CBC)
Peripheral blood smears
Mean corpuscular volume (MCV)
Reticulocyte count (Retic count)
Special Tests
Bone marrow smear, biopsy
FCM, Immunology
Genetics…
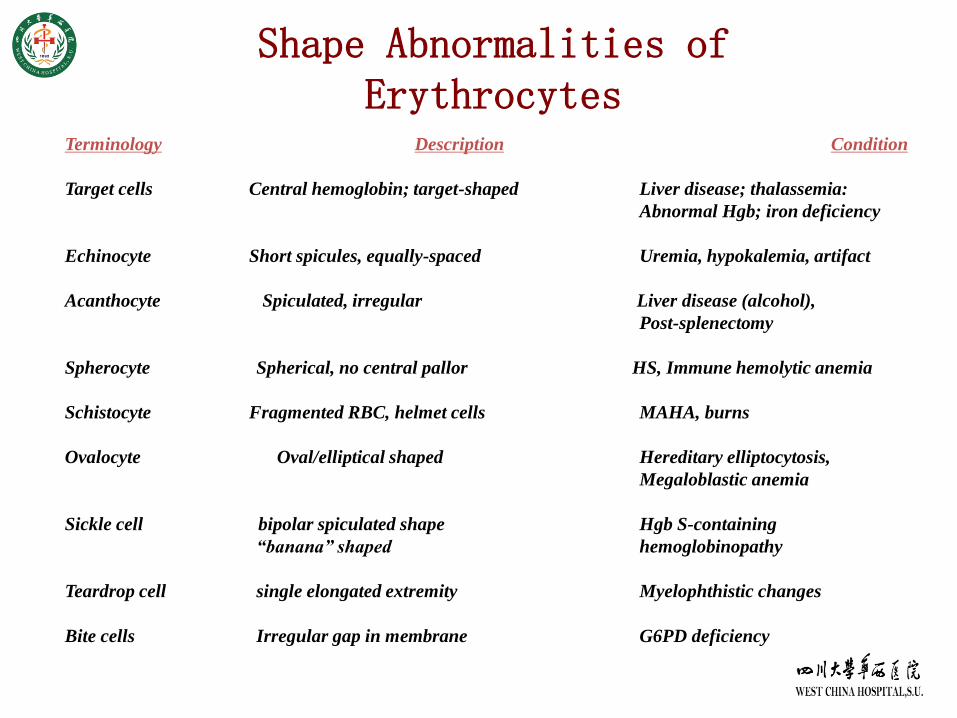
Shape Abnormalities of Erythrocytes
Terminology Description Condition
Target cells Central hemoglobin; target-shaped Liver disease; thalassemia:
Abnormal Hgb; iron deficiency
Echinocyte Short spicules, equally-spaced Uremia, hypokalemia, artifact
Acanthocyte Spiculated, irregular Liver disease (alcohol),
Post-splenectomy
Spherocyte Spherical, no central pallor HS, Immune hemolytic anemia
Schistocyte Fragmented RBC, helmet cells MAHA, burns
Ovalocyte Oval/elliptical shaped Hereditary elliptocytosis,
Megaloblastic anemia
Sickle cell bipolar spiculated shape Hgb S-containing
“banana” shaped hemoglobinopathy
Teardrop cell single elongated extremity Myelophthistic changes
Bite cells Irregular gap in membrane G6PD deficiency
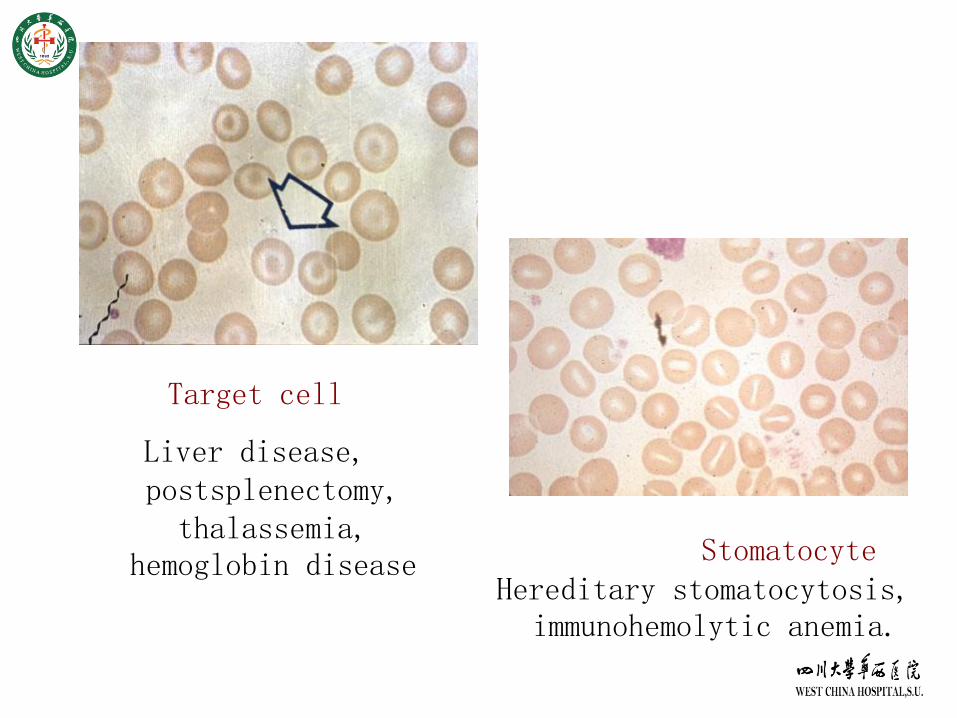
Target cell
Liver disease, postsplenectomy, thalassemia,
hemoglobin disease StomatocyteHereditary stomatocytosis,
immunohemolytic anemia.
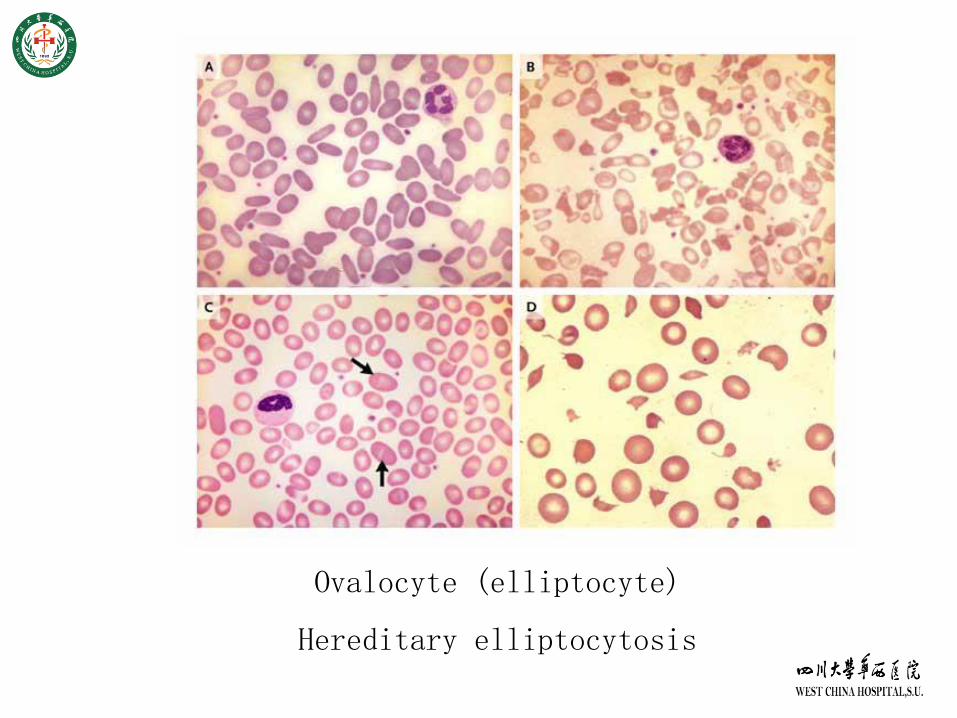
Ovalocyte (elliptocyte)
Hereditary elliptocytosis
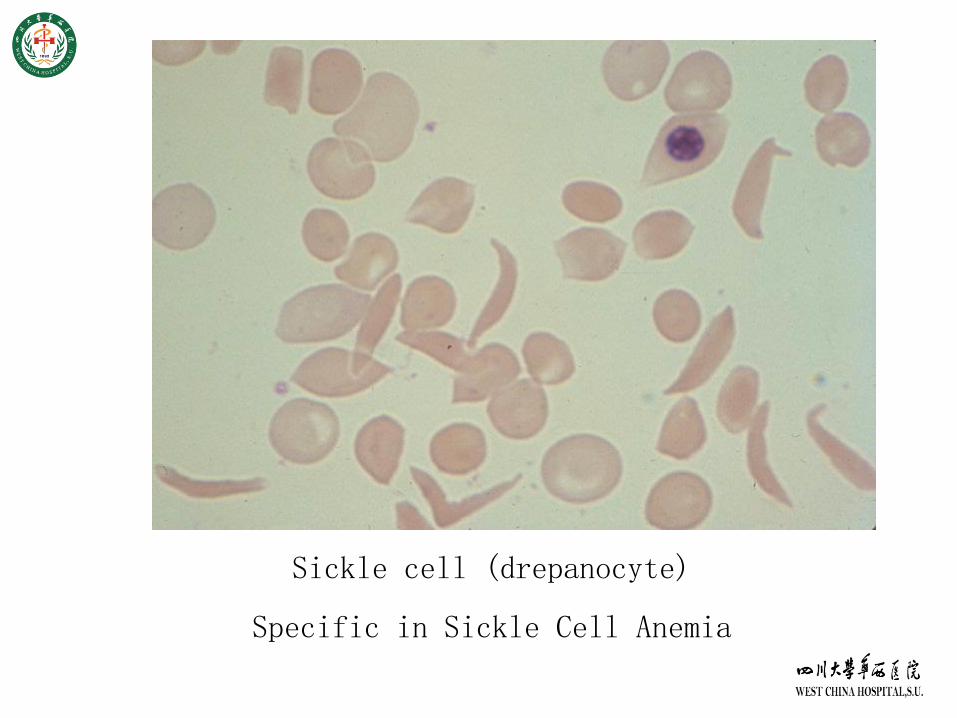
Sickle cell (drepanocyte)
Specific in Sickle Cell Anemia
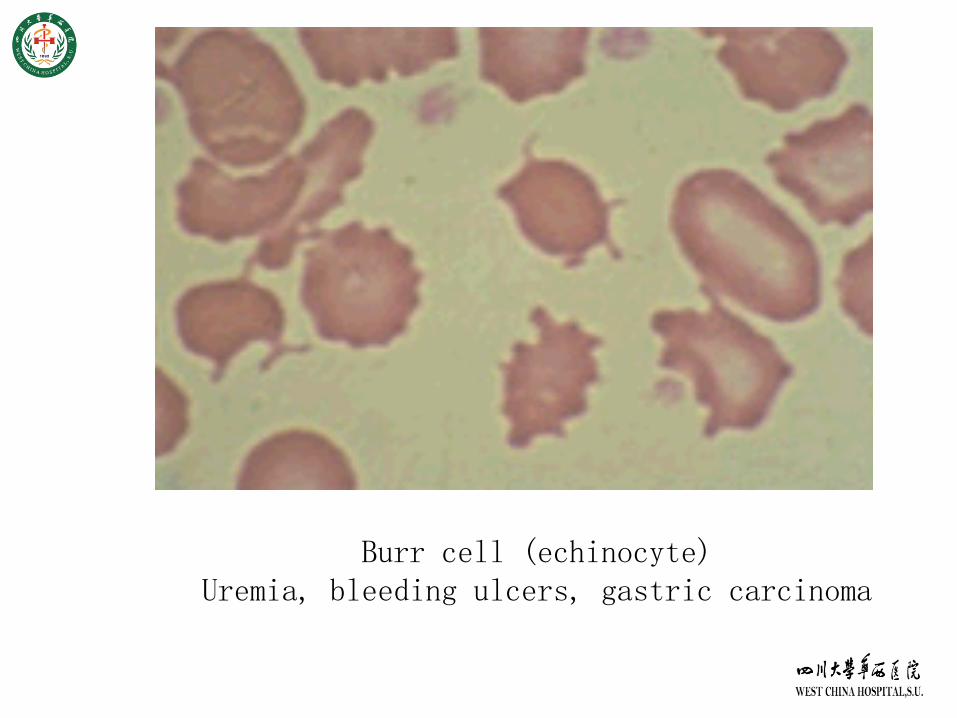
Burr cell (echinocyte) Uremia, bleeding ulcers, gastric carcinoma
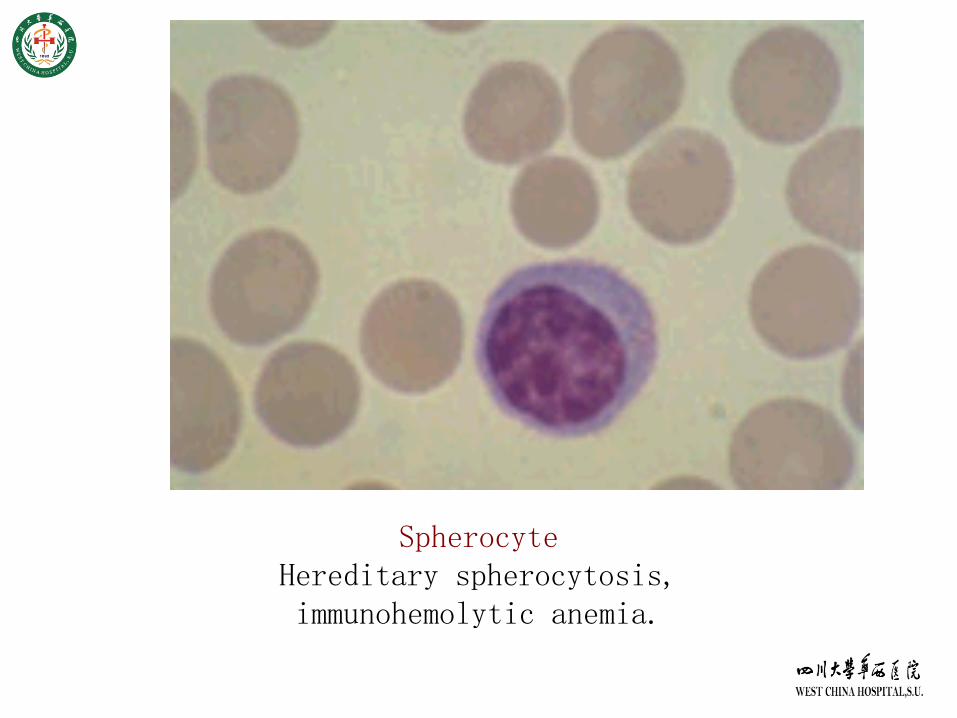
SpherocyteHereditary spherocytosis, immunohemolytic anemia.
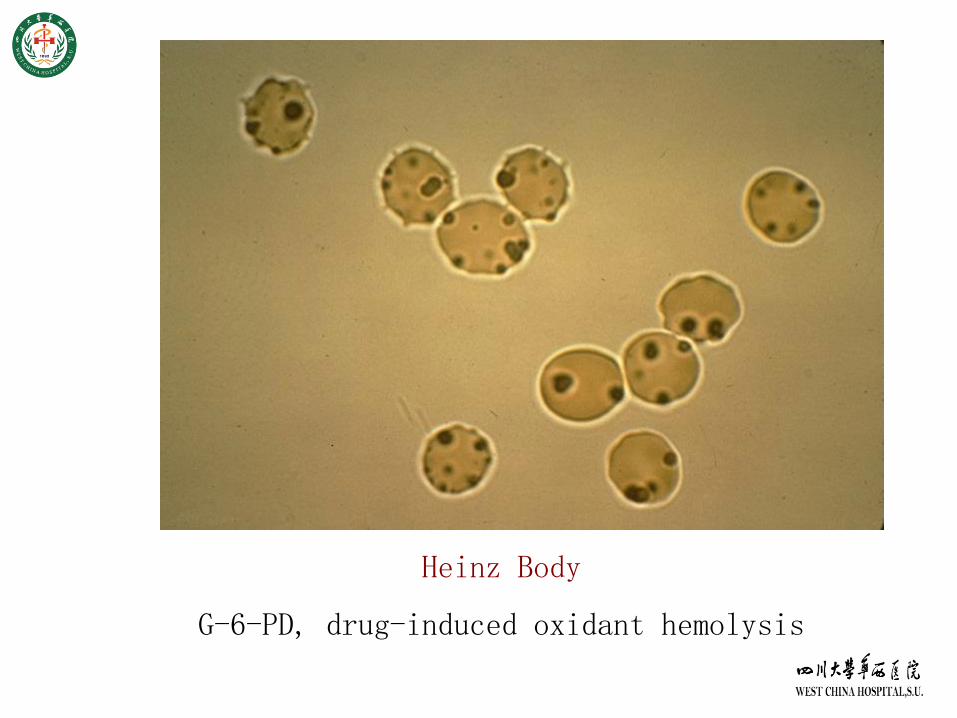
Heinz Body
G-6-PD, drug-induced oxidant hemolysis
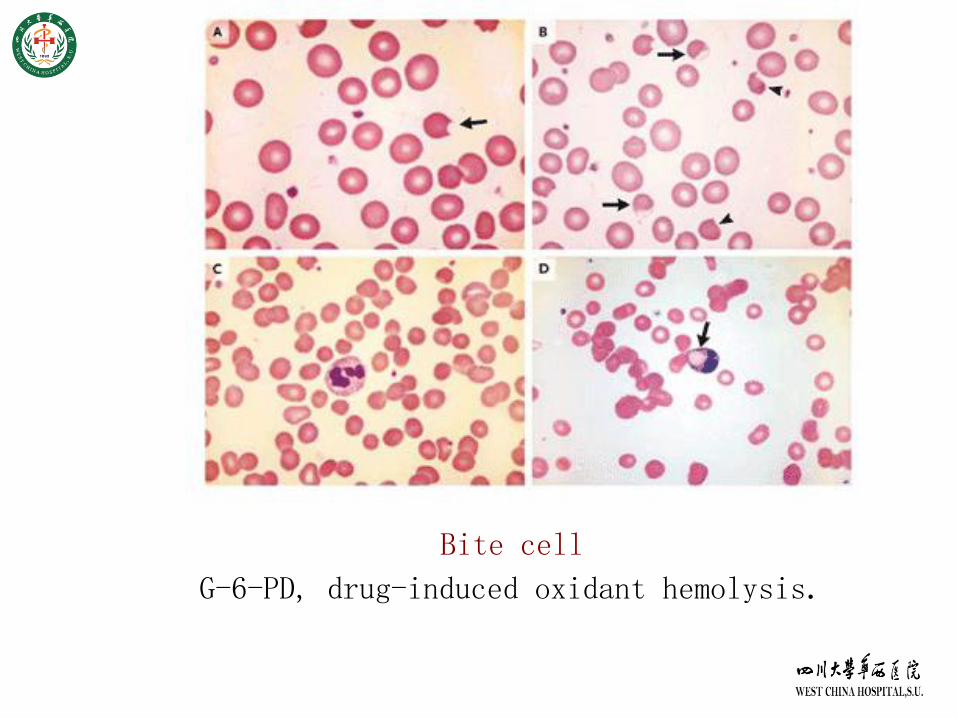
Bite cell
G-6-PD, drug-induced oxidant hemolysis.
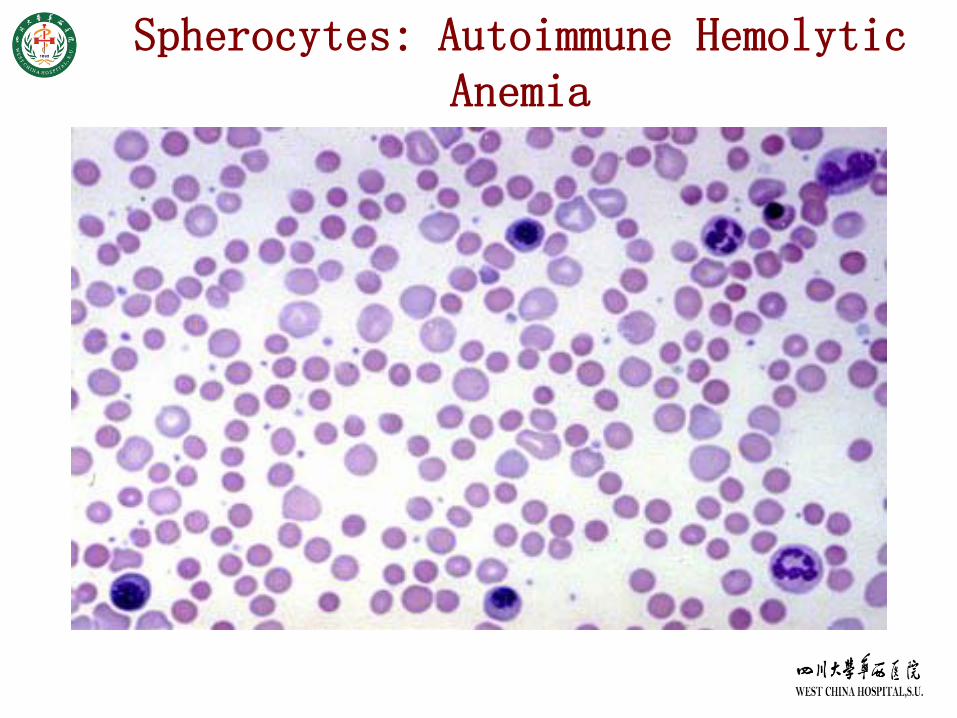
Spherocytes: Autoimmune Hemolytic Anemia
Diagnosis Approach
Step One:
Is there a anemia? and how is the severity?
Step Two:
What’s kind of anemia?
Step Three:
What’s reason caused anemia?
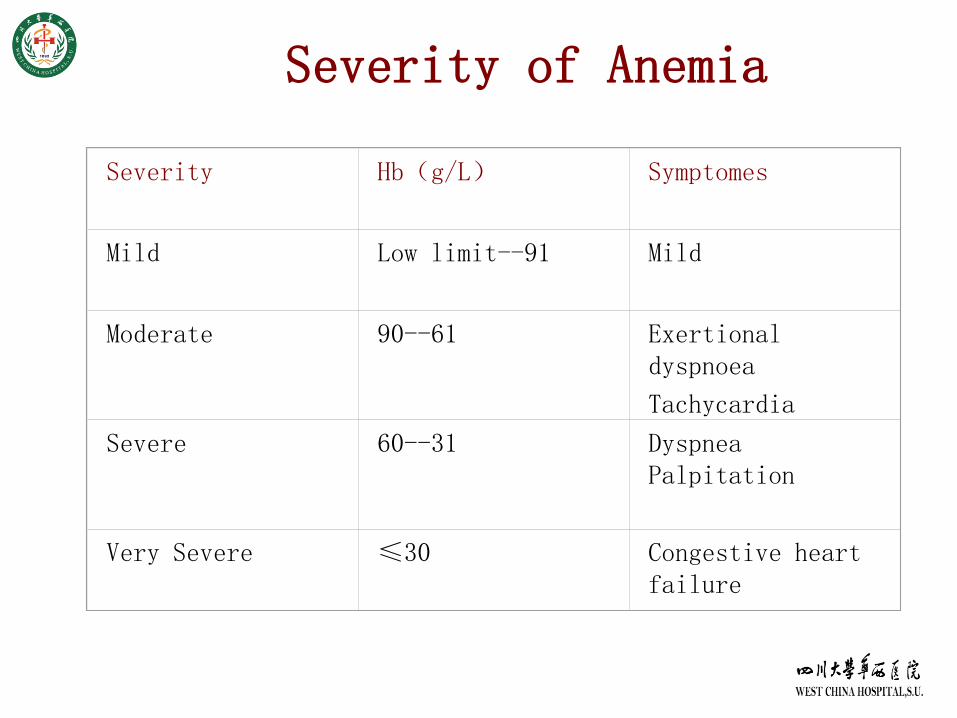
Severity of Anemia
Severity Hb(g/L) Symptomes
Mild Low limit--91 Mild
Moderate 90--61 Exertional dyspnoea
Tachycardia
Severe 60--31 DyspneaPalpitation
Very Severe ≤30 Congestive heart failure
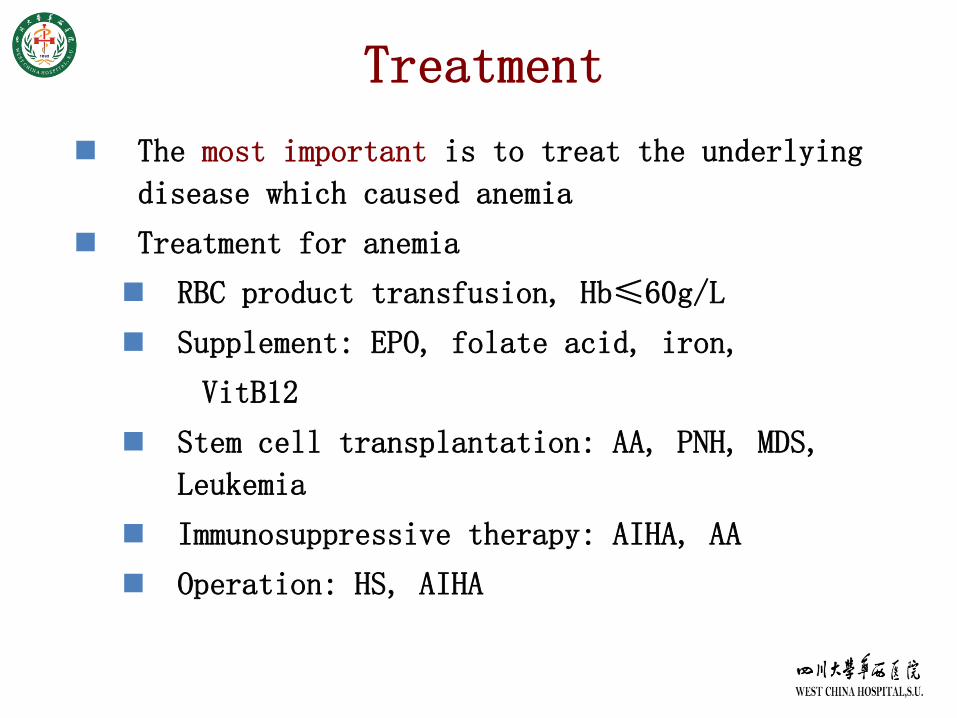
Treatment
The most important is to treat the underlying
disease which caused anemia
Treatment for anemia
RBC product transfusion, Hb≤60g/L
Supplement: EPO, folate acid, iron,
VitB12
Stem cell transplantation: AA, PNH, MDS,
Leukemia
Immunosuppressive therapy: AIHA, AA
Operation: HS, AIHA
Learn from yesterday, live for today, hope for tomorrow. The important thing is to not stop questioning.
Albert Einstein






























