Embed Size (px)
Citation preview

Introduction
Dr Alan HaycoxReader in Health EconomicsHealth Economics UnitUniversity of Liverpool Management
School
Onco-Pharmacoeconomy Training Onco-Pharmacoeconomy Training CourseCourse
Turkey ISPOR Training CourseTurkey ISPOR Training Course

Course objectivesCourse objectives
The two course objectives are:
Understanding the basics of health economics and the underlying rationale
Understanding the application of health economics to oncology especially the concept of opportunity costs

Course timetableCourse timetable
11.00 – 12.00Rationale behind health economics
including opportunity costs13.00 – 15.00Understanding health economics,
health benefit of current cancer drugs and end of life concepts
15.30 – 17.30Workshop around the concept of
opportunity costs based on HERCEPTIN in adjuvant breast cancer in the UK

Rationale for Health EconomicsRationale for Health Economics
Brian Godman
University of LiverpoolMario Negri Institute, Milan, Italy Karolinska Institute, Stockholm, Sweden

Why growing use of Health Why growing use of Health Economics?Economics?Healthcare represents a significant
proportion of national expenditure
New initiatives needed to maintain comprehensive and equitable healthcare with increased volumes and new expensive drugs – especially new oncology drugs
Health economics provides a basis for evaluating different options when resources are scarce – concept of opportunity costs

New specialist drugs key cost driver New specialist drugs key cost driver in Sweden requiring additional in Sweden requiring additional measures measures
Ref: Godman and Wettermark 2009
Total drug expenditures in Stockholm County (prescriptions, hospital, OTC) 1977-2007
0
1
2
3
4
5
6
7
8
1977
1979
1981
1983
1985
1987
1989
1991
1993
1995
1997
1999
2001
2003
2005
2007
Bill
ion
SE
K
Specialist drugs
Non-specialist drugs

The cost of new oncology drugs in Sweden is accelerating matching UK concerns
Ref: Specialist drug project Stockholm, Godman 2009

One UK cancer expert (Professor Sikora at the Hammersmith Hospital) recently estimated that the next generation of cancer drugs could cost the UK alone up to £50billion a year within four years - equivalent to raising the basic tax rate by 15% (15p in the £)
New expensive products (especially new cancer drugs) now account for over 50% of the in-patient hospital drug budget in Marseilles hospitals, with sales growing at over 20% per year. This is leading to a reduction in other services
As a result, use of health economics and concept of opportunity costs will grow especially in cancer
Ref: Sikora 2008, Sermet, Andrieu and Godman et al 2010
The cost of new cancer drugs is a The cost of new cancer drugs is a growing concern in other EU growing concern in other EU countries countries

The Basis of Health EconomicsThe Basis of Health Economics
Demand for healthcare is infinite◦ Increased expectations, ageing populations
and technological changeResources are scarce
◦ Doctors, nurses, hospitals, pharmaceuticalsChoices are necessary
◦ Do we increase the drug budget, pay for more surgeons, increase radiotherapy services or improve pain managements?
Prioritisation is required◦ On what basis? Who should make decisions?
Costs and benefits must be compared◦ How do we measure benefits?

Cost measurement: 3 StagesCost measurement: 3 Stages
Resource identification
Resource measurement
Resource valuation
Resource IdentificationResource Identification
Typically all relevant resource (cost ) items that are used (consumed) during the care process are identified in any health economic evaluation
These are recorded and subsequently costed during the course of undertaking the HE evaluation

Resource MeasurementResource Measurement
The amount of each resource consumed (used) is measured:◦Capital Items (items that provide
services over more than 1 year), e.g. Equipment Buildings
◦Recurrent Items (items consumed within 1 year or less) Materials/ supplies/consumables such as
pharmaceuticals Labour, Utilities (gas, electricity, water, etc.)

Resource ValuationResource Valuation
Average costsMarginal costsOpportunity
costs
A value is attached to each resource consumedResources can be valued differently…
Health economists and policy makers emphasise the importance of ‘opportunity costs’ in valuing overall expenditure as budgets are finite

The most important concept:The most important concept:Opportunity CostOpportunity CostThe opportunity cost of using resources
to produce a good or service is the benefits foregone from those resources not being used in their next best alternative. The concept of opportunity cost lies at the heart of all economic analyse
The health policy goal is to maximise patient outcomes with available resources. This means some benefits will be foregone – but these should be minimised
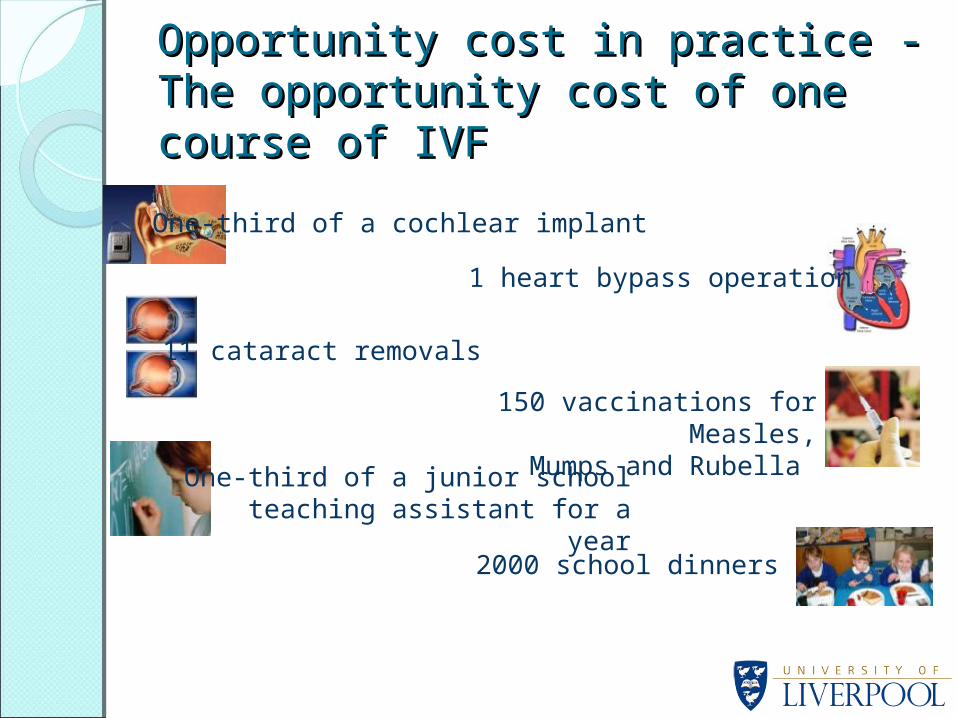
150 vaccinations for Measles,Mumps and Rubella
One-third of a cochlear implant
11 cataract removals
1 heart bypass operation
One-third of a junior school teaching assistant for a year
2000 school dinners
Opportunity cost in practice - The Opportunity cost in practice - The opportunity cost of one course of opportunity cost of one course of IVF IVF

Case History – Adjuvant HERCEPTIN Case History – Adjuvant HERCEPTIN in Breast Cancer in one UK Hospitalin Breast Cancer in one UK HospitalCurrently 355 patients receive adjuvant
treatment in Norfolk and Norwich at GB£0.503mn/ year (16 cured at a cost/ cure ranging from £23000 - £137,000)
Treating 75 patients with early stage breast cancer with HERCEPTIN would cost GB£1.94mn/ year rising to GB£2.3mn with testing, monitoring and administration at a cost/ cure of £650,000
Finite budgets mean tough decisions need to be made on which treatments should be funded and which should be terminated or reduced
Ref: Barrett et al BMJ 2006

Costs and potential benefits of Costs and potential benefits of adjuvant cancer treatments in adjuvant cancer treatments in Norfolk HospitalNorfolk Hospital
Treatment and number of patients Drug cost (GB£000)
Cost/cured patient
(GB£000)
Adjuvant chemotherapy for lung cancer (15 patients)
23 23
Oxaliplatin as adjuvant therapy for colon cancer compared with fluorouracil alone (20 patients)
137 137
Neoadjuvant chemotherapy for oesophageal cancer (25 patients)
8 2.67
Rituximab in addition to CHOP for non-hodgkin lymphoma in patients over 60 (25)
215 71.67
Adjuvant aromatase inhibitors in postmenopausal breast cancer (270 patients) [NB drug costs will fall substantially in Europe once generics routinely available]
120 15
Total – 355 patients and 16 cured 503Ref: Barrett et al BMJ 2006
Possible lessons for TurkeyPossible lessons for Turkey
Other countries have approached the fact of finite resources through a variety of initiatives including:o Setting value criteria for funding new
drugs, e.g. cost/ QALY and minimum effectiveness criteria
o Establishing pre-launch the potential budget impact of new drugs along with potential savings, e.g. new generics becoming available. Subsequently agreeing patient characteristics/ prescribing criteria ahead of launch with key clinicians and monitoring their effectiveness and utilisation post launch

Ref: Ferguson et al 2000
Key stakeholders including leading cancer clinicians agreed only new cancer products with A and B effectiveness criteria and alpha data quality should be funded and prescribed at premium prices in view of resource constraints
Effectiveness
A
B
C
alpha -
D
Data Quality
alpha +
Criteria
beta
Median survival improved > 9months + improved QoL
Median survival improved 3 - 6 months + improved QoL
Improved QoL, no impact on survival
Minimal impact QoL, no impact survival
Criteria
Meta analysis or two high quality RCTs
One poor quality RCT and/or several Phase II studies
One high quality RCTs and supporting Phase II data
3 Levels of effectiveness and data quality chosen
Minimum effectiveness criteria for Minimum effectiveness criteria for funding new drugs in UK cancer funding new drugs in UK cancer hospitalshospitals

Overall survival
Time to progression (TTP)/ Progression free survival (PFS)
Response rate, e.g. OR, PR
Other
2
11
13
1
Primary efficacy end point in main studies
Number
7%
41%
48%
4%
%
• Survival data (when available – overall 13 trials):o Range: 0 – 3.7 months additional survival
versus comparatoro Mean: 1.5 months, Median: 1.2 months
Survival data important as limited Survival data important as limited additional benefits for most cancer additional benefits for most cancer drugsdrugs
Ref: Apolone et al 2005

There are 4 Methods of economic There are 4 Methods of economic evaluationevaluationThe four methods are
◦Cost Minimisation Analysis (CMA)◦Cost Effectiveness Analysis (CEA)◦Cost Utility Analysis (CUA)◦Cost Benefit Analysis (CBA)
These four approaches will be discussed after the coffee break
Any questions?