INTRODUCTION chest pain to the primary care physician represents an immediate challenge. The correct...
If you can't read please download the document
INTRODUCTION chest pain to the primary care physician represents an immediate challenge. The correct diagnosis is most often derived from detailed history
INTRODUCTION chest pain to the primary care physician
represents an immediate challenge. The correct diagnosis is most
often derived from detailed history (pain description; associated
symptoms; and risk factors) that is supported by specific physical
findings, an ECG, and/or chest x-ray. Chest pain accounts for
approximately 6million annual visits to emergency departments (ED)
in (US), making chest pain the 2d most common complaint.
Slide 3
EPIDEMIOLOGY IN PRIMARY CARE POPULATIONS A prospective study of
399 episodes of chest pain in patients seen in multiple outpatient
centers over a one-year period noted the following prevalences of
various causes of chest pain.
Slide 4
Approximately 60 percent of chest pain diagnoses were not
"organic" in origin (ie, not due to cardiac, gastrointestinal, or
pulmonary disease). Musculoskeletal chest pain accounted for 36
percent of all diagnoses (of which costochondritis accounted for 13
percent) followed by reflux esophagitis. Stable angina pectoris was
responsible for 11 percent of chest pain episodes; unstable angina
or myocardial infarction occurred in only 1.5 percen.
GASTROINTESTINAL CAUSES OF CHEST PAIN Gastroesophageal reflux
disease Esophageal hyperalgesia Abnormal motility patterns and
achalasia Esophageal rupture, mediastinitis, and foreign bodies
Medication-induced esophagitis Other gastrointestinal causes of
chest pain,peptic ulcer disease, cholecystitis or biliary colic,
pancreatitis, kidney stones or even appendicitis Other
gastrointestinal causes of chest pain
Slide 7
PULMONARY CAUSES OF CHEST PAIN Pulmonary vasculature- Acute
pulmonary thromboembolism- Pulmonary hypertension and cor pulmonale
Pulmonary vasculature- Acute pulmonary thromboembolism- Pulmonary
hypertension and cor pulmonale Lung parenchyma- Pneumonia- Cancer-
Sarcoidosis Pleura and pleural space- Pneumothorax-
Pleuritis/serositis- Pleural effusion Pleura and pleural space-
Pneumothorax- Pleuritis/serositis- Pleural effusion Mediastinal
disease
Slide 8
PSYCHOGENIC/PSYCHOSOMATIC CAUSES OF CHEST PAIN Chest pain may
be a presenting symptom of panic disorder, depression, and
hypochondriasis, as well as cardiac, cancer, or other phobias.
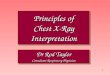
The ascending aortic arch is dilated, displacing the trachea to
the right (black arrow). A left lower lobe density is suggestive of
a pleural effusion. Surgery revealed a dilated ascending aorta with
a dissection
Slide 12
Acute Aortic Dissection
Slide 13
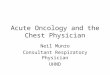
Left panel: A left-sided, simple pneumothorax is seen on this
PA chest radiograph (large white arrows). Right panel: On the
expiratory film, the pneumothorax is larger and more easily seen
(small white arrows).
Slide 14
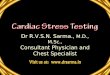
Chest film from a patient with Boerhaave's syndrome reveals air
under both diaphragmatic leaflets.
Slide 15
Cardiomegaly due to a massive pericardial effusion. At least
200 mL of pericardial fluid must accumulate before the cardiac
silhouette enlarges.
Slide 16
Apical 4 chamber view from a 2-D echocardiogram shows a large
pericardial effusion surrounding the heart. The heart has a
swinging motion during the cardiac cycle and there is slight
compression of the right atrium early in diastole, suggesting early
tamponade
Slide 17
diastolic collapse of the right atrium and ventricle, a result
of tamponade.
Slide 18
Slide 19
Slide 20
25 , , , , A.at the time of admission , B.at the time of
discharge
Slide 21
General approach Onset of pain (eg, abrupt or gradual)
Provocation/Palliation (which activities provoke pain; which
alleviate pain) Quality of pain (eg, sharp, squeezing, pleuritic)
Radiation (eg, shoulder, jaw, back) Site of pain (eg, substernal,
chest wall, diffuse, localized) Timing (eg, constant or episodic,
duration of episodes, when pain began)
Slide 22
Comorbidities: hypertension, diabetes mellitus, peripheral
vascular disease, malignancy Recent events: trauma, major surgery
or medical procedures (eg, endoscopy), periods of immobilization
(eg, long plane ride) Other factors: cocaine use, cigarette use,
family history.
Slide 23
EMERGENCY RESPONSE TO CHEST PAIN IN THE OFFICE Any patient with
a recent onset of chest pain, especially when the symptoms are
ongoing, who may be potentially unstable based upon history,
appearance, or vital signs, should be transported immediately to an
emergency department in an ambulance equipped with a
defibrillator.
Slide 24
intravenous access, placement of a cardiac monitor, and
supplemental oxygen if breathlessness, hypoxemia, or signs of heart
failure or shock are present. A 12-lead electrocardiogram within 10
minutes after presentation. Chest Radiography blood sample for
cardiac enzyme measurement. Biomarkers, cardiac troponin (T or I;
cTnT or cTnI); creatine kinase MB isoenzyme (CK-MB) is less
sensitive. [8] acute coronary syndrome (ACS) 325 mg aspirin,
Sublingual nitroglycerin.nitroglycerin
Slide 25
EVALUATION The office evaluation of new onset chest pain in
stable individuals should begin with the consideration of
imminently life-threatening causes (including acute coronary
syndrome, pulmonary embolus, aortic dissection, pneumothorax, and
esophageal rupture).
Slide 26
This is usually accomplished using clinical judgement, along
with ECG testing, and less frequently exercise testing, other
noninvasive testing, or invasive angiography.
Slide 27
Description of chest pain A thorough description of the pain is
an essential first step in the diagnosis of chest pain.
Slide 28
Several studies suggest that a diagnosis of "nonspecific" chest
pain carries risk of increased mortality, especially due to
ischemic heart disease. Thus, a diagnosis of nonspecific chest pain
should be made cautiously and may indicate the need for vigilant
follow-up.
Slide 29
Quality of the pain The patient with myocardial ischemia often
denies feeling chest "pain." More typical descriptions include
squeezing, tightness, pressure, constriction, strangling, burning,
heart burn, fullness in the chest, a band-like sensation, knot in
the center of the chest, lump in the throat, heavy weight on chest,
and toothache (when there is radiation to the lower jaw)
Slide 30
Acute chest pain with a classically ripping or tearing quality
may be helpful in diagnosing acute aortic dissection. Pulmonary
embolism presents with pleuritic chest pain in only 40 to 48
percent of patients. The chest pain of myocarditis can be
pleuritic, but it can also mimic that of myocardial ischemia.
Slide 31
Region or location of pain Patients who indicated larger areas
of discomfort were more likely to have an ischemic etiology of pain
than patients who indicated smaller areas of discomfort.
Slide 32
Slide 33
Radiation The pain of myocardial ischemia may radiate to the
neck, throat, lower jaw, teeth, upper extremity, or shoulder. Chest
pain that radiates between the scapulae may be due to aortic
dissection. The pain of pericarditis typically radiates to one or
both trapezius ridges. Cervical radiculopathy may present with
chest, upper back or upper extremity pain.
Slide 34
timing The pain associated with a pneumothorax or a vascular
event such as aortic dissection or acute pulmonary embolism
classically has an abrupt onset with the greatest intensity of pain
at the beginning. The onset of ischemic pain is more often gradual
with an increasing intensity over time. A crescendo pattern of pain
can also be caused by esophageal disease. "Functional" or
nontraumatic musculoskeletal chest pain might have a much more
vague onset.
Slide 35
Provocation Discomfort that reliably occurs with eating is
suggestive of upper gastrointestinal disease. Postprandial chest
pain may be due to gastrointestinal or cardiac disease; in the
latter case it can be a marker of severe myocardial ischemia (eg,
left main or three-vessel CHD. Chest discomfort provoked by
exertion is a classic symptom of angina, although esophageal pain
can present similarly.
Slide 36
Other factors that may provoke ischemic pain include cold,
emotional stress, meals, or sexual intercourse. Pain made worse by
swallowing is likely of esophageal origin. Truly pleuritic chest
pain is worsened by respiration and may be exacerbated when lying
down.
Slide 37
Palliation Pain that responds to sublingual nitroglycerin is
frequently thought to have a cardiac etiology or to be due to
esophageal spasm.nitroglycerin The pain of pericarditis typically
improves with sitting up and leaning forward. On the other hand,
pain that abates with cessation of activity strongly suggests an
ischemic origin.
Slide 38
Severity The severity of pain is not a useful predictor of the
presence of CHD. As many as one-third of myocardial infarctions may
go unnoticed by the patient.
Slide 39
Associated symptoms Belching, a bad taste in the mouth, and
difficult or painful swallowing are suggestive of esophageal
disease, although belching and indigestion also may be seen with
myocardial ischemia. Vomiting may occur in the setting of
myocardial ischemia (particularly transmural myocardial
infarction), in addition to gastrointestinal problems such as
peptic ulcer disease, cholecystitis, and pancreatitis.
Slide 40
Diaphoresis, Dyspnea, Cough,Palpitations Syncope The patient
with myocardial ischemia may describe presyncope. However, syncope
associated with chest pain should raise a concern for aortic
dissection, a hemodynamically significant pulmonary embolus, a
ruptured abdominal aortic aneurysm, or critical aortic
stenosis.
Slide 41
Psychiatric symptoms Symptoms of panic disorder, generalized
anxiety, depression, or somatization may occur in patients with
chest pain. Constitutional symptoms The elderly in particular may
describe profound fatigue as the presenting complaint of myocardial
infarction.
Slide 42
Symptoms associated with coronary heart disease in women In a
report of 515 women with an acute MI, only 57 percent reported
acute chest pain; the other presenting symptoms were shortness of
breath (58 percent), weakness (55 percent), and fatigue (43
percent.
Slide 43
Risk factors The presence of hyperlipidemia, left ventricular
hypertrophy, or a family history of premature CHD increase the risk
for myocardial ischemia. Hypertension is a risk factor for both CHD
and aortic dissection. A recent infection, especially viral, may
precede an episode of pericarditis or myocarditis. Cigarette
smoking is a nonspecific risk factor for serious pathology; it is
associated with CHD, thromboembolism, aortic dissection,
pneumothorax, and pneumonia.
Slide 44
Physical examination The focused physical examination is used
to support or disprove hypotheses generated by the history. The
general appearance,A full set of vital signs,complete cardiac
examination Examination of Cardiovascular System
Slide 45
ALGORITHM FOR THE APPROACH TO THE DIAGNOSIS OF CHEST PAIN Step
1 (Evaluate need for emergent care ) Consider potentially
life-threatening causes of chest pain. Patients in whom an acute
coronary syndrome (acute myocardial infarction or unstable angina)
is suspected should receive emergent care. critical noncoronary
diagnosis such as pulmonary embolus, pneumothorax, aortic
dissection, esophageal rupture, or acute abdomen.
Slide 46
Step 2 (Emergent care not needed) In patients in whom a
diagnosis of stable CHD appears likely based on symptoms that are
suggestive of angina and/or a history of cardiac risk factors.
Slide 47
Step 3 (Symptoms consistent with stable angina ) Evaluate the
patient for CHD. outpatient management, admitting the patient to
the hospital, especially if symptoms are progressive, Consider
other causes of anginal chest pain, such as cardiac syndrome X and
pulmonary hypertension.
Slide 48
Step 4 (Evaluation for CHD was negative ) Evaluate the patient
for gastrointestinal disease. This evaluation may initially involve
a trial of acid suppression.
Slide 49
Step 5 (Symptoms not suggestive of angina) Step 5a For patients
who are felt not to have an ischemic etiology for chest pain but
who have significant risk factors for CHD, consider arranging for
an evaluation for CHD. Step 5b If symptoms suggest a
musculoskeletal etiology, a trial of an NSAID is appropriate. Step
5c If symptoms suggest a gastrointestinal etiology, evaluate the
patient for gastrointestinal disease.
Slide 50
Step 5d If symptoms suggest a psychogenic etiology, evaluate
the patient for a psychosocial source of chest pain. Step 5e
Consider chest anatomy as a guide to other less common causes of
non-life-threatening chest pain including (zoster, breast
disease,pericarditis, lung parenchyma, vasculature, or pleura.
Slide 51
Step 6 (Persistent chest pain ) If chest pain persists and
evaluations for CHD (as in step 5a), musculoskeletal pain (as in
step 5b), gastrointestinal pain (as in step 5c), psychogenic pain
(as in step 5d), and other causes (as in step 5e) have not all been
performed, those evaluations should now be undertaken.
Slide 52
Step 7 (Diagnostic evaluations negative ) Patient likely has
chronic idiopathic chest pain. Since this is known to cause
significant disability, consider referral to a pain management
center or medical symptom reduction program.
Slide 53
Slide 54
Algorithm for the initial diagnostic approach to a patient with
chest pain
Slide 55
Slide 56
Slide 57
Algorithm for the evaluation and management of patients
suspected of having ACS.
Slide 58
Slide 59
Options for transporting STEMI patients and initial reperfusion
treatment