Embed Size (px)
Citation preview

Introduction
Chapter 1
Alice YY. Cheng
Canadian Diabetes Association 2013 Clinical Practice Guidelines

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Faculty for Slide Deck Development
• Jonathan Dawrant, BSc, MSc, MD, FRCPC• Zoe Lysy, MDCM, FRCPC• Geetha Mukerji, MD, FACP, FRCPC• Dina Reiss, MD, FACP, FRCPC• Steven Sovran, BSc, MD, MA, FRCPC
• Alice Y.Y. Cheng, MD, FRCPC• Peter J. Lin, MD, CCFP• Catherine Yu, MD, FRCPC, MHSc

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Outline
• Epidemiology of diabetes in Canada
• Care gap still exists
• Overview
• Committee structure
• Major changes in 2013

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Prevalence of Diabetes among Individuals aged 20-79 years, Europe, North America, Oceania, 2010

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Diabetes in Canada: Prevalence by Province and Territory
Public Health Agency of Canada. Diabetes in Canada: Facts and figures from a public health perspective. Ottawa, 2011.
NL6.5%
ON 6.0%
QC 5.1%
PE5.6%
NB5.9%
NS 6.1%
MB 5.9%
SK 5.4%
AB 4.9%
BC 5.4%
NT 5.5%
YT 5.4%
NU 4.4%
† Age-standardized to the 1991 Canadian population.
Age-standardized† prevalence of diagnosed DM among individuals ≥ 1 year, 2008/09
NL, NS and ON had the highest prevalence, while NU, AB and QC had the lowest.
< 5.0
5.0 < 5.5
5.5 < 6.0
6.0 < 6.5
≥ 6.5
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association Public Health Agency of Canada. Diabetes in Canada: Facts and figures from a public health perspective. Ottawa, 2011.
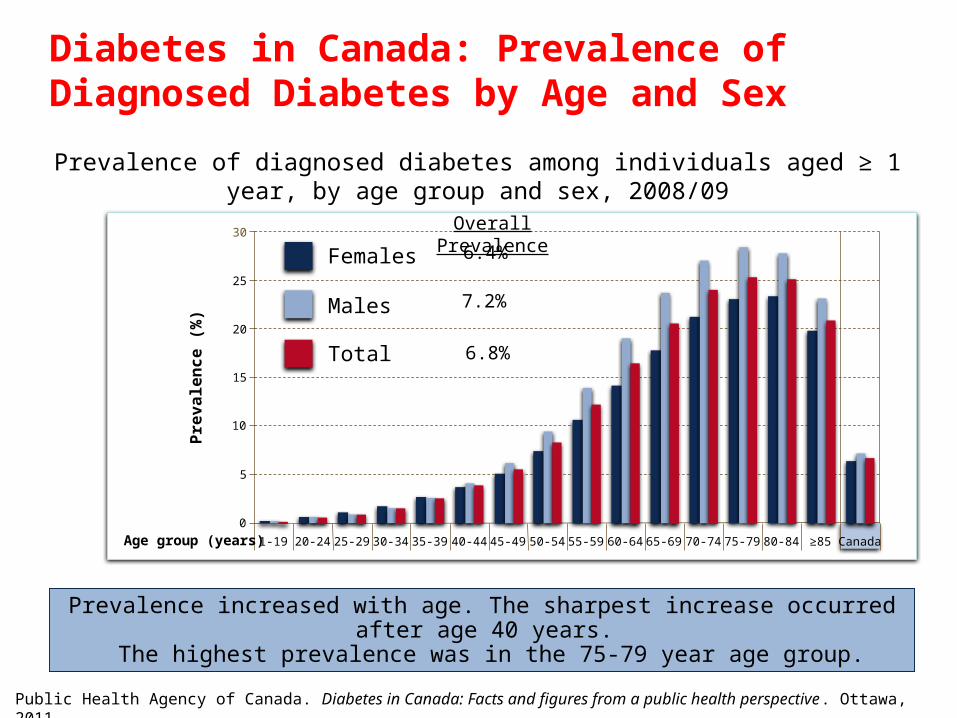
Prevalence increased with age. The sharpest increase occurred after age 40 years. The highest prevalence was in the 75-79 year age group.
Pre
va
len
ce
(%
)
0
10
15
25
30
1-19
5
20
20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64 65-69 70-74 75-79 80-84 ≥85 CanadaAge group (years)
Females
Males
Total
Overall Prevalence
6.4%
7.2%
6.8%
Diabetes in Canada: Prevalence of Diagnosed Diabetes by Age and Sex
Prevalence of diagnosed diabetes among individuals aged ≥ 1 year, by age group and sex, 2008/09

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Diabetes in Canada: Prevalence of Diagnosed Diabetes 1998/99 to 2008/09Age-standardized prevalence and number of cases of diagnosed diabetes among
individuals aged ≥ 1 year, 1998/99 to 2008/09
3.3%
5.6%
Public Health Agency of Canada. Diabetes in Canada: Facts and figures from a public health perspective. Ottawa, 2011.

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Diabetes in Canada: Incidence of Diagnosed Diabetes 1998/99 to 2008/09
Age-standardized incidence and number of cases of diagnosed diabetes among individuals aged ≥ 1 year, 1998/99 to 2008/09
Public Health Agency of Canada. Diabetes in Canada: Facts and figures from a public health perspective. Ottawa, 2011.
5.6 per 1000
individuals
5.6 per 1000
individuals

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Guideline Targets Achieved
A1c (≤7%) (n=5103) LDL (≤2.0 mmol/L) (n=5069) SBP/DBP (<130/80 mm HG) (n=5099)
All 3 Endpoints (A1c, LDL,
BP) (n=5104)
0%
20%
40%
60%
50%
57%
36%
13%
% o
f p
atie
nts
Leiter LA et al. Can J Diabetes 2013; in press
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Dr. Meng-Hee Tan
16 pages

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Dr. Sara Meltzer and Dr. Lawrence Leiter
31 pages

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Dr. Stewart Harris
150 pages

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Dr. Vincent Woo
201 pages

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Dr. Alice Cheng
212 pages

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
CPG Objective
• Provide guidance on the most appropriate
management for people with diabetes mellitus
• Enhance diabetes prevention efforts with the goal of
reducing the burden of diabetes related complications
• Inform clinical decisions made by healthcare
professionals
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Overview
• 38 chapters
• 120 professional volunteers– Family medicine, Endocrine, Internal medicine, Pediatrics,
Cardiology, Neurology, Infectious Disease, Ophthalmology,
Nephrology, Urology, Psychology, Obstetrics, Optometry
– Nurses, Dietitians, Nurse Practitioners, Pharmacists,
Psychologists, Exercise Physiologists
2013

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Committee structure
Expert committee
Steering committee
Executive committee
Executive Editor Independent LibrarianCDA Support Team
External R
eviewers
(National and International)
Independent Methods R
eview
DISSEMINATION AND IMPLEMENTATION COMMITTEE
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Executive Committee
• Alice Y.Y. Cheng, Chair
• Gillian Booth, Methodology Chair
• Maureen Clement
• William Harper
• Aileen Knip
• Vincent Woo
2013

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Steering Committee
Sub-Group Chairs
– Ron Goldenberg - Diagnosis & Classification
– Robyn Houlden - Management (1)
– Amir Hanna - Management (2)
– Bruce Perkins - Microvascular
– David Fitchett - Macrovascular
– Danièle Pacaud - Pediatrics
– David Thompson - Pregnancy
2013

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Steering Committee
Advisors
– Onil Battarcharya
– Lori Berard
– Stewart Harris
– Lawrence Leiter
– Stuart Ross
– Jean-François Yale
– Catherine Yu
2013

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Community Representatives
• Mr. Ram Krishna
• Ms. Diana Provenzano
2013

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Expert CommitteeRejeanne GougeonSteven GroverGord GubitzBetty HarveyRob Hegele Cheri HernandezJonathan HowlettCéline HuotNadira HuseinS. Ali ImranHelen JonesTina KaderErin KeelyGlen KennyAngela KohSharon KozakRam KrishnaPhilippe L'AllierEric LaroseDavid Lau Richard LewanczukPeter LinMeera LuthraLori MacCallum
John MacFadyenGail MacNeillAndrea MainG.B. John Mancini Phil McFarlane Angela McGibbonGraydon MeneillyAmanda MikalachkiDavid MillerBeth MitchellRichard NahasMariam NaqshbandiConstadina PanagiotopoulosBreay W.PatyRonald PlotnikoffPaul PoirierAlly PrebtaniDiana ProvenzanoZubin PunthakeeRémi Rabasa-LhoretDoreen RabiTom RansomSonja Reichert
Ravi RetnakaranCindy RichardsonMichael RiddellDavid RobinsonRob Roscoe Edmond RyanElizabeth SellersPeter SeniorMathew SermerArya SharmaMichael SharmaDiana SherifaliJohn SievenpiperRonald SigalFrank Stockl James StoneJean-Claude TardifDaniel TessierCory TothEllen TothMicheal VallisChristina VinokuroffSean WhartonDiane WherrettDana WhithamSandi Williams
Andrew AdvaniFiliberto AltomareKathryn ArcudiMarni ArmstrongHoward BergerIan BlumerKeith BoweringShelley BoydVera BrilGerald BrockSarah CapesAndre CarpentierDale ClaytonPam ColbyJohn DornanRobert DufourPaula DworatzekRoland DyckJean-Marie EkoéJohn EmbilDenice FeigRobert Gagnon Jeremy GilbertRichard Gilbert Jeannette Goguen
2013

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Changes to Structure in 2013
• Harmonization: – Canadian Hypertension Education Panel (CHEP)
– Society of Obstetrics and Gynecology of Canada (SOGC)
– Canadian Cardiovascular Society (CCS)
– C-CHANGE
• Inclusions:– Drug cost table included
– “Practical Tips” box
2013

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Changes to Structure in 2013 (continued) 2013
• Expanded Dissemination & Implementation
• Diabetes in high-risk ethnic populations chapter moved into Screening and Reduction of risk chapters
• Stroke in Diabetes is a new chapter

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Highlights of Major Changes
Diagnosis • A1C for the diagnosis of diabetes (A1C ≥6.5%)
• A1C for the diagnosis of prediabetes (A1C 6.0-6.4%)
Organization of Care • New “Diabetes Patient Care Flow Sheet”
Glycemic Targets • Individualization of glycemic targets
• Vast majority of people with diabetes target an A1C ≤7.0%
• Better definition of scenarios to consider a target A1C ≤6.5%
or less stringent target of A1C 7.1-8.5%
2013

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Highlights of Major Changes (continued)
Self-monitoring Blood Glucose (SMBG)
• Recommendations for frequency of SMBG for those with
type 2 diabetes, not receiving insulin therapy
Nutrition Therapy
• Continued emphasis on balanced, individualized nutritional
therapy with the inclusion of alternative dietary patterns as
options
2013
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Pharmacologic Management of type 2 diabetes– Achieve target A1C within 3-6 months of diagnosis
– New algorithm for the pharmacologic management of
T2DM with emphasis on individualization of agent choice
– Metformin may be used at the time of diagnosis
– A1C ≥8.5% at the time of diagnosis should receive
immediate pharmacologic therapy and consideration for
use of ≥ 2 antihyperglycemic therapies and/or insulin
– Inclusion of Cost Table for antihyperglycemic therapies
Highlights of Major Changes (continued) 2013

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
In-hospital Management– Glycemic targets premeal blood glucose (BG) 5-8 mmol/L
and random BG <10 mmol/L for the majority of non-
critically ill patients
– BG 8-10 mmol/L for critically ill
– BG 5-10 mmol/L in the perioperative period
Highlights of Major Changes (continued) 2013

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Vascular Protection • Statins if:
– Macrovascular or microvascular disease
– Age ≥ 40 years
– DM > 15 years and age > 30 years, or
– As per CCS 2012 lipid guidelines
• ACE-inhibitor or ARB if:
– Macrovascular or microvascular disease
– Age ≥ 55 years
• ASA not routinely recommended for primary prevention
Highlights of Major Changes (continued) 2013
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Chronic Kidney Disease• Microalbuminuria = albumin-creatinine ratio (ACR) ≥2.0
mg/mmol for both men and women
• Sick Day Management document for acute illness
Diabetes in Pregnancy • New criteria for screening and diagnosis of gestational
diabetes
Diabetes in the Elderly• Frail elderly glycemic target of A1C ≤8.5%, fasting and pre-
prandial BG of 5-12 mmol/L
Highlights of Major Changes (continued) 2013

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
“Neither evidence nor clinical judgment alone is sufficient.
Evidence without judgment can be applied by a technician.
Judgment without evidence can be applied by a friend.
But the integration of evidence and judgment is what the healthcare provider does in order to dispense the best clinical care.”
(Hertzel Gerstein, 2012)

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
CDA Clinical Practice Guidelines
http://guidelines.diabetes.ca – for professionals
1-800-BANTING (226-8464)
http://diabetes.ca – for patients












![No~ KM +" w m ] R ÔK UqO Ð > aq Ô 11/ 8* ~ 9*]_M `h{ q Ô 11/ 15 * ~ 16 * L Â ç ý _w]KM^m E ¯ gÄ Êù Õ g E ¯ gÄ × ¿ E ¯ gÄ ¿ E ¯ gÄ Êù Õ yy Ä yy yy yy yy yy](https://img.pdfslide.us/doc/110x75/60b2e348c8efc8547128bb3c/no-km-w-m-r-k-uqo-aq-11-8-9m-h-q-11-15-.jpg)