Embed Size (px)
Citation preview

INTRINSIC IMBALANCE IN
RHEUMATOID ARTHRITIS
6TH ANNUAL MEETING:
HAND THERAPY ASSOCIATION OF NORTHERN
CALIFORNIA
Andrew J. Watt MD
The Buncke Clinic

DISCLOSURES:
I have no personal or financial interest in the products contained
within this presentation.
All identifiable photos utilized with permission.
GOALS & OBJECTIVES:
• To review the pathophysiology of Rheumatoid Arthritis
• To understand the basic finger deformities that result from
longstanding Rheumatoid Arthritis
• To understand the Management of Chronic Deformities
Resulting from Rheumatoid arthritis
– Techniques
– Indications
– Contraindications
– Optimizing Success

RHEUMATOID ARTHRITIS
• Chronic, systemic inflammatory
disease of unknown cause
– Autoimmune Disease
– Articular Manifestations
– Extra-articular Manifestations
– Female >>Male (3:1)
– Onset 20-40
– Inflammatory Target:
Synovium

RHEUMATOID ARTHRITIS:
PATHOLOGY
• Characteristic Pathologic
Finding: Chronic
Synovitis with Pannus
Formation
• Inflammatory Pannus Erodes:
– Cartilage
– Bone
– Ligament
– Tendon

RHEUMATOID ARTHRITIS:
PATHOLOGY

RHEUMATOID ARTHRITIS:
DISTRIBUTION

RHEUMATOID ARTHRITIS:
DEFORMITY
• Classic Finger
Deformities:
– Ulnar Drift
• MCP Subluxations
• Ulnar Subluxation /
Dislocation of Extensor
Tendon
– Boutonniere Deformity
– Swan Neck Deformity
The extensor mechanism is an inter-related
system of intrinsic and extrinsic
components in harmonious balance.
Disruption of this balance leads to
mechanical compensation (deformity).

OPPOSITES!
• Rheumatoid Deformities
represents movement in
opposing directions: – Radial Deviation vs. Ulnar
Deviation
– Flexion vs. Extension
• The system will always
try to reach equilibrium
• Deviation occurs at the
next available joint.

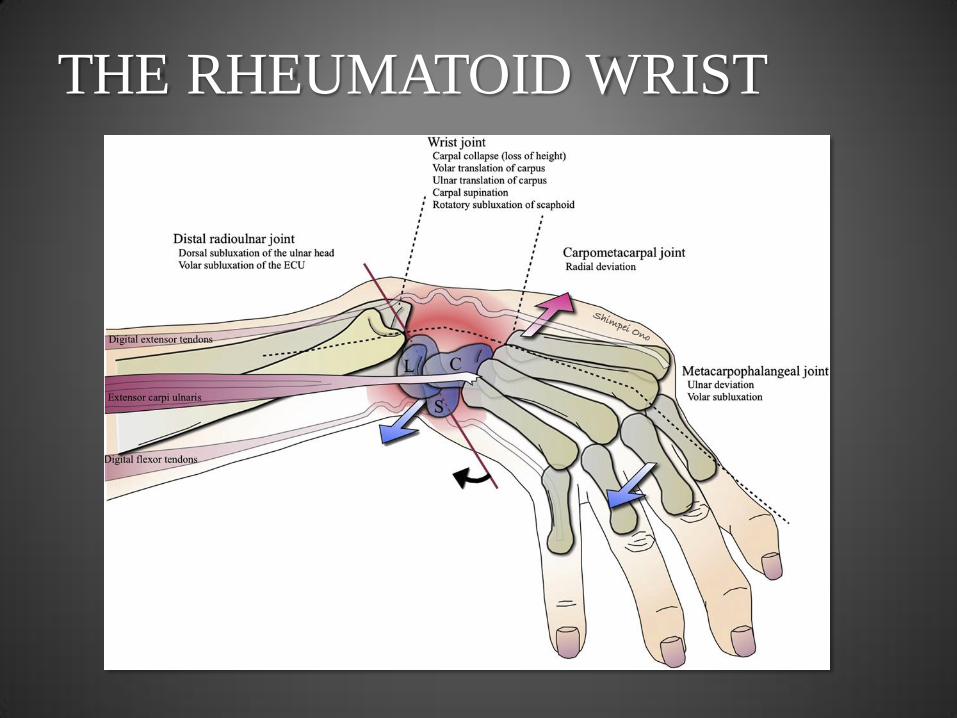
THE RHEUMATOID WRIST
• Characteristics:
– Dorsal Subluxation of the Ulnar
Head
• Loss of Dorsal joint
capsular support and TFCC
• Really volar subluxation of
the radius
– Palmar and Ulnar Translation
of the Carpus
– ECU subluxes volarly
– Radial wrist Extensors
unopposed
– Metacarpals move with the
wrist and become radially
deviated
THE RHEUMATOID WRIST

ULNAR DRIFT
• Characteristics:
– Metacarpophalangeal Joint
Volar Subluxation
– Ulnar Subluxation /
Dislocation of Extensor
Tendon

ULNAR DRIFT
MCP Arthritis with Synovitis
1. Loss of ulnar wrist support
2. Attenuation of Dorsal Joint Capsule & Volar Plate
3. Attenuation of Radial Collateral Ligament
4. Radial Deviation of MC
Volar & Ulnar Subluxation of MCP Joint
1. Introduces laxity into the extensor mechanism
- Radial intrinsic placed on stretch
- Ulnar intrinsic lax
2. Attenuation of the Radial Sagittal Band
Ulnar Subluxation / Dislocation of Extensor Tendon
New Equilibrium
• Ulnar intrinsic at shorter resting length, tightens
• Radial intrinsic at longer resting length, attenuates

ULNAR DRIFT
MCP Arthritis with Synovitis
1. Loss of Ulnar Wrist Support
2. Attenuation of Dorsal Joint Capsule & Volar Plate
3. Attenuation of Radial Collateral Ligament
4. Radial Deviation of MC
Volar & Ulnar Subluxation of MCP Joint
1. Introduces laxity into the extensor mechanism
- Radial intrinsic placed on stretch
- Ulnar intrinsic lax
2. Attenuation of the Radial Sagittal Band
Ulnar Dislocation of Extensor Tendon
New Equilibrium
• Ulnar intrinsic at shorter resting length, tightens
• Radial intrinsic at longer resting length, attenuates
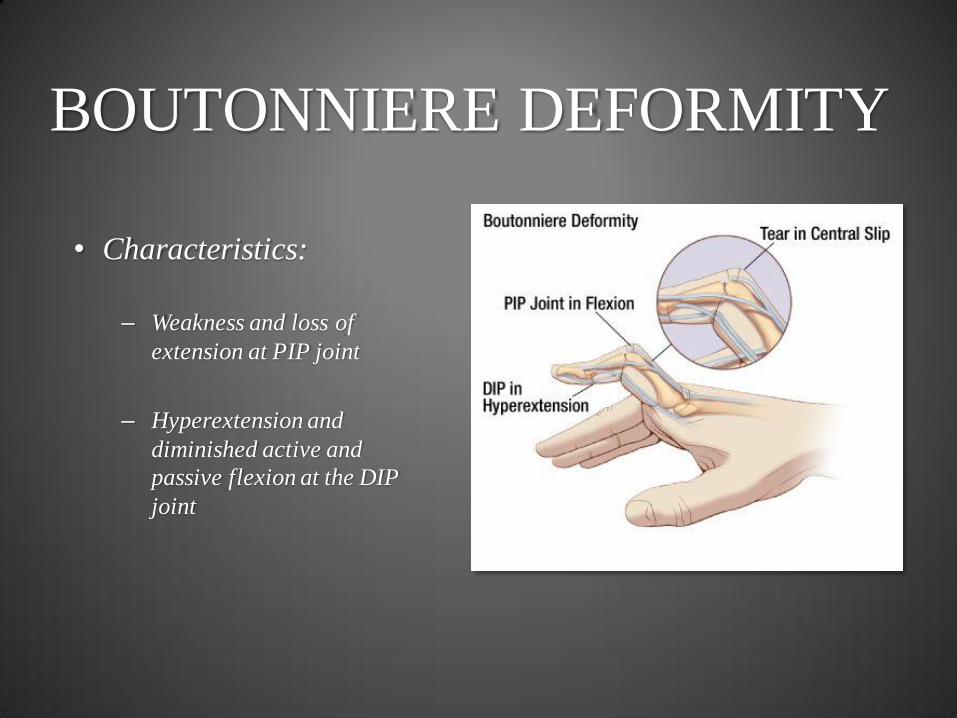
BOUTONNIERE DEFORMITY
• Characteristics:
– Weakness and loss of
extension at PIP joint
– Hyperextension and
diminished active and
passive flexion at the DIP
joint

BOUTONNIERE DEFORMITY
PIP Arthritis of Central Slip
1. Synovial inflammation attenuates central slip
Disruption of Triangular Ligament
1. Attenuated in setting of inflammatory pannus
Volar Migration of Lateral Bands
* Move volar to the axis of rotation of the PIP joint.
Mechanically become a flexor of the PIP joint rather than an extensor
Contracture of ORL, CL & Volar Plate

SWAN NECK DEFORMITY
• Characteristics:
– Loss of DIP extension
– Imbalance of Extension force at the PIP joint.
– Hyperextension and diminished active and passive flexion at the PIP joint

SWAN NECK DEFORMITY
• What causes a swan neck
deformity in Rheumatoid
Arthritis?
– Wrist in origin
– MCP in origin
– PIP in origin
– DIP in origin

SWAN NECK DEFORMITY:
DIP ORIGIN DIP Joint Arthritis
Attenuation of Terminal Tendon
Flexion of DIP Joint
1. Laxity Introduced into Lateral Bands
• Decreased functional length
2. Lateral Bands Migrate Dorsal to the Axis of Rotation of the PIP Joint
DIP Hyperextension

SWAN NECK DEFORMITY:
PIP ORIGIN PIP Joint Arthritis
1. Attenuation of Volar Plate
2. Rupture of FDS insertion
Hyperextension of PIP Joint
1. Lateral Bands Migrate Dorsal to the Axis of Rotation of the PIP Joint
2. Laxity Introduced into Terminal Tendon
• Decreased functional length
DIP Flexion

SWAN NECK DEFORMITY:
MCP ORIGIN MCP Joint Arthritis
1. Volar Subluxation & Ulnar Drift
2. Laxity introduced into extensor mechanism
PIP Hyperextension
1. Lateral Bands Migrate Dorsal to the Axis of Rotation of the PIP Joint
2. Volar Plate Attenuation
3. Laxity Introduced into Terminal Tendon
• Decreased functional length
DIP Flexion

ADDRESSING IMBALANCE
IN RA • Keys to Success:
– Recognize the 1° deformity
and distinguish from the 2°
deformity
• ie MCP Subluxation >>
Ulnar Subluxation
– Realign the skeletal
components.
– Rebalance the soft tissue
• Eliminate deforming
forces
• Augment corrective
forces
– Work Proximal to Distal

SURGICAL OPTIONS FOR
TREATING INTRINSIC
IMBALANCE IN RA
• Tools & Techniques:
– Joints:
• Arthroplasty
• Arthrodesis
– Soft Tissue:
• Rebalancing
• Tendon Transfer
• Soft Tissue
Reconstruction

SURGICAL OPTIONS FOR
TREATING INTRINSIC
IMBALANCE IN RA
• Surgical Considerations – Patient’s Goals:
• Pain Relief
• Functional Gains
• Aesthetics
– Durability:
• Stability over time
– Medical Control of
Disease
– Concordant Expectations
• ***Address the Wrist
First*** – Arthroplasty
– Arthrodesis
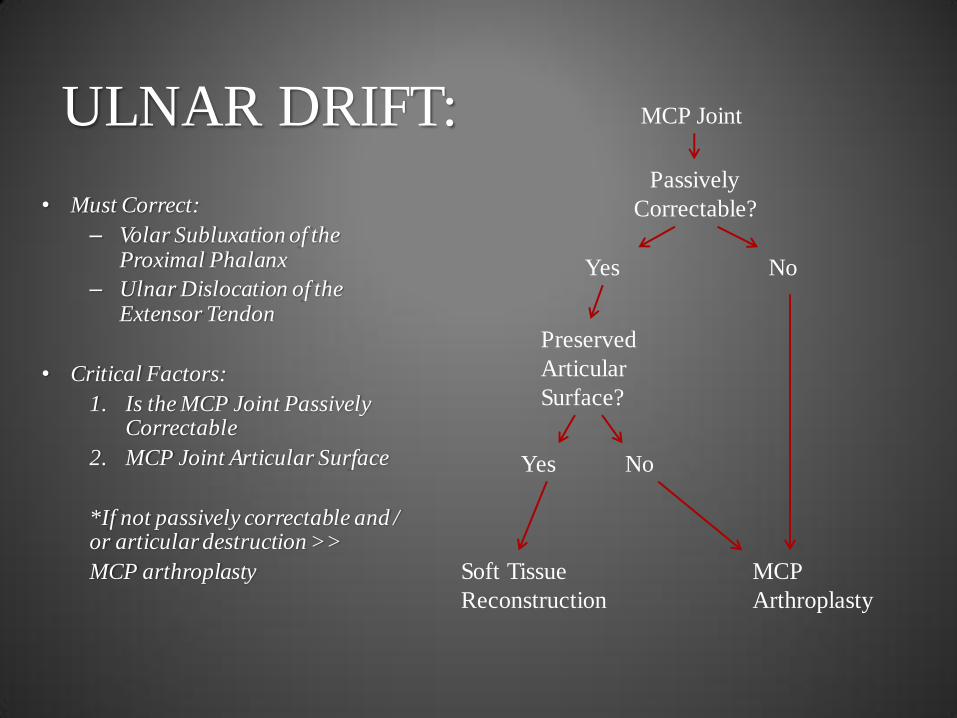
ULNAR DRIFT:
• Must Correct:
– Volar Subluxation of the Proximal Phalanx
– Ulnar Dislocation of the Extensor Tendon
• Critical Factors:
1. Is the MCP Joint Passively Correctable
2. MCP Joint Articular Surface
*If not passively correctable and / or articular destruction >>
MCP arthroplasty
MCP Joint
Passively
Correctable?
Yes No
MCP
Arthroplasty
Preserved
Articular
Surface?
Yes No
Soft Tissue
Reconstruction

ULNAR DRIFT: SOFT
TISSUE RECONSTRUCTION
• Crossed Intrinsic
Transfer
– Transfer of Ulnar
Intrinsic to the Radial
Side of the Adjacent
Finger
– Reefing of Radial
collateral ligament
– +/- Sagittal Band
Reconstruction Courtesy K. C. Chung

ULNAR DRIFT: SOFT
TISSUE RECONSTRUCTION
• EDC Tenodesis
– Central Slip of EDC
used to create a
restraint to ulnar
displacement
– Passed beneath MCP
RCL
– Reefing of Radial
sagittal band &
collateral ligament
PC Dell et al JHS (Br) 2001.

ULNAR DRIFT: SOFT
TISSUE RECONSTRUCTION
• Sagittal Band
Reconstruction
– Palmaris Longus
Tendon Graft + Bone
Tunnel
– Reefing of Radial
Sagittal Band &
Collateral Ligament

ULNAR DRIFT: JOINT & SOFT
TISSUE RECONSTRUCTION
• Silicone MCP Arthroplasty
• Crossed Intrinsic Transfer

BOUTONNIERE:
• Must Correct:
– Central Slip Incompetence
– Volar Migration of Lateral Bands
– PIP Flexion Deformity
• Critical Factors:
1. Is the PIPJoint Passively Correctable
2. PIP Joint Articular Surface
*Boutonniere corrections in RA are highly unpredictable and tend to fail.
PIP Joint
Passively
Correctable?
Yes No
PIP
Arthrodesis
Preserved
Articular
Surface?
Yes No
Trial of
Splinting

SWAN NECK:
• Must Correct:
– PIP Hyperextension
– DIP Flexion Deformity
• Critical Factors:
1. Is the PIP Joint Passively
Correctable
2. PIP Joint Articular Surface
*If not passively correctable
and / or articular destruction
>> PIP arthrodesis
PIP Joint
Passively
Correctable?
Yes No
PIP
Arthrodesis
Preserved
Articular
Surface?
Yes No
Soft Tissue
Reconstruction

SWAN NECK DEFORMITY:
• Treat Wrist and MCP joint
deformity first then move distally
• PIP Hyperextension:
– Create palmar restraint that
will allow flexion but prevent
hyperextension
– Tenodesis
• Conjoint lateral band
tenodesis
• FDS Tenodesis
• ORL (Littler) Tenodesis

SWAN NECK DEFORMITY:
SOFT TISSUE
RECONSTRUCTION • Conjoint Lateral Band Tenodesis
• Indications:
– Mild Swan Neck (<20° of PIP Hyperextension)
– Preserved PIP Joint Surface
– Adequate soft tissue integrity
• Lateral Bands mobilized and secured volar to the axis of PIP rotation
• Lateral bands become:
– Flexor of the PIP joint
– Extensor of the DIP joint

SWAN NECK DEFORMITY:
SOFT TISSUE
RECONSTRUCTION • FDS Tenodesis
• Indications:
– Supple Swan Neck, any
degree of deformity
– Preserved PIP Joint Surface
– Intact FDS!!!
• FDS Tendodesis
– 1 slip transected proximally
and sutured to tendon
sheath or proximal phalanx

SWAN NECK DEFORMITY:
SOFT TISSUE
RECONSTRUCTION • FDS Tenodesis
• Indications:
– Supple Swan Neck, any
degree of deformity
– Preserved PIP Joint Surface
– Intact FDS!!!
• FDS Tendodesis
– 1 slip transected proximally
and sutured to tendon
sheath or proximal phalanx

SWAN NECK DEFORMITY:
SOFT TISSUE
RECONSTRUCTION
• ORL Ligament Tenodesis
• Indications:
– Supple Swan Neck, any
degree of deformity
– Preserved PIP Joint Surface
– No available FDS

SWAN NECK DEFORMITY:
SOFT TISSUE
RECONSTRUCTION
• ORL Ligament Tenodesis
• Indications:
– Supple Swan Neck, any
degree of deformity
– Preserved PIP Joint Surface
– No available FDS

CONCLUSIONS
• Rheumatoid arthritis affects the hand, both the articular surfaces and
ligamentous support structures, via progressive synovial inflammation,
pannus formation and erosion
• Rheumatoid hand deformity is characterized by deformity at the level of the
wrist, MCP, PIP and DIP with distal mobile components displacing to
counteract proximal deformity (ie wrist deformity leads to compensatory
MCP deformity leads to compensatory PIP deformity….)
• Surgical treatment relies of identifying the principle actor causing
imbalance and working proximal to distal to correct the deforming forces

THANK YOU






















![Untitled-2 [cea-ca.org]](https://img.pdfslide.us/doc/110x75/61c45919c8ee2f43021ebae5/untitled-2-cea-caorg.jpg)