Embed Size (px)
Citation preview

Intravenous Immunoglobulin Attenuates Experimental Autoimmune Arthritis by
Inducting Reciprocal Regulation of Th17 and Treg in an IL-10-Dependent Manner
Seon-Yeong Lee1*, Young-Ok Jung
2*, Jun-Geol Ryu
1, Chang-Min Kang
1, Eun-Kyung Kim
1,
Hye-Jin Son1, Eun-Ji Yang
1, Ji-Hyeon Ju
1, 3, Young-Sun Kang
4, Sung-Hwan Park
1, 3, Ho-Youn
Kim1, 3
, Mi-La Cho1**,
1The Rheumatism Research Center, Catholic Research Institute of Medical Science, The
Catholic University of Korea, Banpo-dong, Seocho-gu, Seoul, 137-701, South Korea.
2Division of Rheumatology, Department of Internal Medicine, Kangnam Sacred Heart
Hospital, Hallym University, Seoul 137-701, Korea.3Center for Rheumatic Disease, Division
of Rheumatology, Department of Internal Medicine, Seoul St. Mary's Hospital, The Catholic
University of Korea, Banpo-dong, Seocho-gu, Seoul, 137-701, South Korea. 4Department of
Biomedical Science and Technology, Institute of Biomedical Science and Technology,
Konkuk University, 1 Hwayang-dong, Gwangjin-gu, Seoul 143-701, Republic of Korea;
Authorship note: SYL and YOJ contributed equally to this work.
Funding:Funding:Funding:Funding: This study was supported by a grant of the Korean Health Technology R&D
Project, Ministry for Health & Welfare, Republic of Korea (HI09C1555) and also
supported by the Bio & Medical Technology Development Program of the National
Research Foundation (NRF) funded by the Korean government (MEST) (No.
2012M3A9C6049783)
Full Length Arthritis & RheumatismDOI 10.1002/art.38627
This article has been accepted for publication and undergone full peer review but has not beenthrough the copyediting, typesetting, pagination and proofreading process which may lead todifferences between this version and the Version of Record. Please cite this article as an‘Accepted Article’, doi: 10.1002/art.38627© 2014 American College of RheumatologyReceived: May 30, 2013; Revised: Jan 07, 2014; Accepted: Mar 11, 2014

2
Conflict of Interests : None
**Address correspondence to: Mi-La Cho, Rheumatism Research Center, Catholic Institutes
of Medical Science, The Catholic University of Korea, 505 Banpo-dong, Seocho-gu, Seoul
137-040, Korea (South)
Phone: 82-2-2258-7467; Fax: 82-2-599-4287; E-mail: [email protected].
Keywords: Intravenous Immunoglobulin, Th17, Germinal Center, FcγIIB, Rheumatoid
Arthritis
Running Head: IVIG attenuate arthritis by Th17/Treg balance
Page 2 of 32
John Wiley & Sons
Arthritis & Rheumatology

3
ABSTRACT
Objective. Intravenous immunoglobulin (IVIG) is used as a therapeutic agent in
various autoimmune diseases. The aims of this study were to investigate the therapeutic
effects of IVIG on collagen-induced arthritis (CIA) and the mechanism responsible for
any therapeutic effects.
Methods. IVIG was administered to CIA mice and the in vivo effects were
determined. T helper 17 (Th17) and regulatory T (Treg) cell frequencies were analyzed
by flow cytometry, and cytokine levels in the supernatant were measured by enzyme-
linked immunosorbent assays. Subpopulations of T cells and B cells of spleens were
assessed by confocal microscopy.
Results. The arthritis score and incidence of arthritis were lower in mice treated
with IVIG compared with untreated mice. Histopathological analysis showed less joint
damage in mice treated with IVIG. The expression of proinflammatory cytokines,
specific collagen type II antibody, and osteoclast markers was significantly reduced in
mice treated with IVIG. IVIG induced increased Foxp3 expression and inhibited Th17
cell development. The number of Foxp3+ Treg cells increased and the number of Th17
cells decreased in the spleens of mice treated with IVIG. The number of Foxp3+
follicular helper T cells increased and subsequent maturation of germinal center B cells
was inhibited by IVIG. IVIG also upregulated interleukin-10 (IL-10) and FcγγγγIIB
expression. IVIG lost its treatment effects on arthritis induced in IL-10 knockout mice.
Conclusion. Our results showed that IVIG has therapeutic effects by modulating
CD4+ T cell differentiation. The therapeutic effects of IVIG are dependent on IL-10.
Page 3 of 32
John Wiley & Sons
Arthritis & Rheumatology

4
INTRODUCTION
Intravenous immunoglobulin (IVIG) is currently used in the treatment of a wide
variety of inflammatory and autoimmune diseases ((1, 2). Diseases for which IVIG has been
shown to be beneficial include Kawasaki disease, primary immunodeficiency disease, and
refractory polymyositis (1). IVIG is also used empirically to treat other autoimmune diseases
such as systemic lupus erythematosus and vasculitis (3-5).
The mechanism by which IVIG exerts beneficial effects in these diseases cannot be
explained. The classical action of IVIG includes the suppression or neutralization of
autoantibodies and cytokines, neutralization of the complement system, and prevention of the
autoantibody binding to the Fcγ receptor (FcγR) (1). IVIG upregulates the expression of
inhibitory FcγRIIB (6) and regulates cells of the innate immune system. IVIG therapy inhibits
the maturation of dendritic cells (7) and reduces the percentage of natural killer (NK) cells
and activity of NK cells in the peripheral blood (8). However, the beneficial effects of IVIG
extend beyond the half-lives of the infused immunoglobulins (Igs), and its treatment effects
occur in diseases whose pathology is attributed mainly to cellular immunity such as graft-
versus-host disease and cellular rejection (9, 10).
Regulatory T (Treg) cells play important roles in peripheral tolerance and in the
prevention of autoimmune diseases (11, 12). Patients with RA have defective
CD4+CD25
+Foxp3 Treg cells, and activation of Treg cells can improve clinical symptoms of
collagen-induced arthritis (CIA), regulate cytokine production, and inhibit osteoclastogenesis
in vitro and in vivo (13, 14).
The pathogenic roles of interleukin-17 (IL-17) and T helper 17 (Th17) cells, the
major producers of IL-17, are well known in inflammatory arthritis (15, 16). Th17 cells and
IL-17 increase synovial inflammation and joint destruction (15-19). Treg cells and Th17 cells
Page 4 of 32
John Wiley & Sons
Arthritis & Rheumatology

5
are reciprocally regulated (20, 21) and skewing the balance toward Th17 cells makes the
body prone to inflammation. Therefore, regulating the Treg:Th7 cell ratio is of main interest
when treating autoimmune diseases.
Follicular helper T (TFH) cells, a special CD4+ T cell subset localized in the B cell
follicles, specialize in helping B cells in the germinal center (GC) reaction (22, 23).
Dysregulated TFH cells contribute to the development of autoreactive B cells, which produce
autoantibodies and induce autoimmune diseases (24). There has been no report on the effects
of IVIG on TFH cells and subsequent changes in GC B cells.
Several studies have suggested the possible regulatory effects of IVIG on T cell
subsets (25, 26). Several reports showed therapeutic effects of IVIG on inflammatory arthritis
(27) (28) . In this study, we examined the efficacy of IVIG in the treatment of CIA and the
underlying mechanisms by which IVIG modulated CIA. We investigated the changes in the
numbers of Treg and Th17, and the ratio elicited by IVIG and the effects of IVIG on TFH cells
within the GC B cell population. We also verified that the therapeutic effect of IVIG was lost
in IL-10 knockout (KO) mice.
Page 5 of 32
John Wiley & Sons
Arthritis & Rheumatology

6
MATERIALS AND METHODS
Animals. Six-week-old male DBA1/J mice (SLC, Inc., Shizuoka, Japan) were
maintained in groups of five in polycarbonate cages in a specifically pathogen-free
environment and were fed standard mouse chow (Ralston Purina, Gray Summit, MO) and
water ad libitum. All experimental procedures were examined and approved by the Animal
Research Ethics Committee at the Catholic University of Korea.
Induction of arthritis and injection of IVIG. To examine the effect of IVIG on
CIA, IVIG was injected intravenously (i.v.) once on day 7 after CIA induction. To induce
CIA, 100 µg of bovine type II collagen (CII) and complete Freund’s adjuvant (Chondrex,
Inc.,Redmond, WA) were injected intradermally into the base of the tail. Starting the next day,
three independent observers examined the severity of arthritis three times a week. The
severity of arthritis was recorded using the mean arthritis index on scale of 0–4, as previously
reported (29).
Measurement of Ig concentrations. The serum concentrations of IgG, IgG1, and
IgG2a were measured using mouse IgG, IgG1, and IgG2a enzyme-linked immunosorbent
assay (ELISA) quantitation kits (Bethyl Laboratories, Montgomery, TX).
Immunohistochemistry. Mouse joint tissues were obtained 15 weeks after the immunization
and were fixed in 4% paraformaldehyde, decalcified in EDTA bone decalcifier, and
embedded in paraffin. Joint tissues were sectioned at 7-µm thickness, dewaxed using xylene,
dehydrated through a gradient of alcohol, and then stained with hematoxylin and eosin
(H&E), toluidine blue, Safranin O, and tartrate-resistant acid phosphatase (TRAP) to detect
Page 6 of 32
John Wiley & Sons
Arthritis & Rheumatology

7
proteoglycans. The H&E stained sections were scored for inflammation and bone erosion.
Inflammation was scored according to the following criteria: 0 = no inflammation, 1 = slight
thickening of the lining layeror some infiltrating cells in the underlying layer, 2 = slight
thickening of the lining layer plus some infiltrating cells in the underlying layer, 3 =
thickening of the lining layer, an influx of cells in the underlying layer and the presence of
cells in the synovial space and 4 = synovium highly infiltrated with many inflammatory cells.
Cartilage damage was determined using safranin-O staining and Toluidine blue and the extent
of cartilage damage was scored according to the following criteria: 0 = no destruction, 1 =
minimal erosion limited to single spots, 2 = slight to moderate erosion in a limited area, 3 =
more extensive erosion and 4 = general destruction (30).
Immunohistochemistry was performed using the Vectastain ABC kit (Vector
Laboratories, Burlingame, CA). Joint tissues were incubated with the first primary
monoclonal antibodies (mAbs) at 4°C; the antibodies were goat anti-mouse tumor necrosis
factor-α (anti-TNF-α mAb), rabbit anti-mouse IL-1β mAb, rabbit anti-mouse IL-6 mAb,
rabbit anti-mouse IL-17, rabbit anti-mouse IL-10, and goat anti-mouse FcRIIB mAb. The
primary antibodies were detected with a biotinylated secondary linking Ab, followed by
incubation with streptavidin–peroxidase complex for 1 h. The final color product was
developed using 3,3′-diaminobenzidine chromogen (Dako, Carpinteria, CA). Positive cells
were counted and results are expressed as mean ± standard deviation (SD).
Real-time polymerase chain reaction (PCR). Relative expression of specific
mRNAs was quantified by real-time PCR using SYBR Green I (Roche Diagnostics). The
following sense and antisense primers were used: for TNF-α, 5′-AGC CCC CAG TCT GTA
TCC TT-3′ and 5′-CTC CCT TTG CAG AAC TCA GG-3′; for IL-6, 5′-ATT TGT GTG CTG
Page 7 of 32
John Wiley & Sons
Arthritis & Rheumatology

8
AAG GAG GC-3′ and 5′-AAA GGA CAG GAT GTT GCA GG-3′; for IL-1β, 5′-CTT GGA
TGA GGA CAT GAG CAC CTT C-3′ and 5′-GGA AGA CAG GCT TGT GCT CTG C-3′;
for FcRIIB, 5′-CCC TGG GAA CTC TTC TAC CC-3′ and 5′-CA GCA GCC AGT CAG
AAA TCA-3′; and for β-actin, 5′-GAA ATC GTG CGT GAC ATC AAA G-3′ and 5′-TGT
AGT TTC ATG GAT GCC ACA G-3′.
Flow cytometric analyses of T and B cells. Cell pellets were prepared from the
spleens of CIA and IVIG-injected CIA mice. To examine the population of T helper cells, the
cells were stained with anti-CD4–peridin chlorophyll protein (PerCP) mAb (eBioscience) and
anti-CD25–allophycocyanin (APC) (eBioscience). Cells were permeabilized and fixed with
CytoFix/CytoPerm (BD Pharmingen) as instructed by the manufacturer, and stained further
with anti-Foxp3–phycoerythrin (PE) (eBioscience), anti- IFNγ-APC, anti-IL-4-PE, IL-17-
FITC or IL-10-APC (all purchase eBioscience). To examine the population of B cells, the
cells were stained with anti-CD4–PerCP, anti-B220-APC, GL7-FITC, CXCR5-APC and PD-
1-FITC.
Measurement of IL-17 concentration. The concentration of IL-17 in serum was
measured by sandwich ELISA. Anti-mouse IL-17 mAb (R&D Systems, Minneapolis, MN)
was added to a 96-well plate (Nunc, Roskilde, Denmark) and incubated overnight at 4°C. The
wells were treated with blocking solution (phosphate-buffered saline containing 1% bovine
serum albumin and 0.05% Tween 20), the samples and the standard recombinant IL-17 (R&D
Systems) were added to the 96-well plate, and the plate was incubated. Biotinylated IL-17
polyclonal Ab (R&D Systems) was added, and the reaction was allowed to proceed. The plate
was washed, 1:2,000 diluted ExtrAvidin–alkaline phosphatase (Sigma-Aldrich, St Louis, MO)
Page 8 of 32
John Wiley & Sons
Arthritis & Rheumatology

9
was added, and the reaction was allowed to proceed. The plate was washed, and 50 µl of p-
nitrophenyl phosphate disodium salt (Pierce Chemical Company, Rockford, IL) diluted in
diethanolamine buffer was applied.
Staining for confocal microscopy. Spleen tissues were obtained 15 weeks after
primary immunization. The various cell populations were identified with specific antibodies
(all from eBioscience). To examine the populations of Th cells, the tissues were stained with
anti-CD4–PerCP, anti-interferon (IFN)-γ–fluorescein isothiocyanate (FITC), anti-IL-4–FITC,
anti-CD25–APC, anti-Foxp3–FITC, anti-IL-17–PE, and anti-IL-10–PE. To analyze the
populations of cells expressing signal transducer and activator of transcription (STAT), the
tissues were stained with (all from eBioscience) anti-CD4–PE, anti-p-STAT3 705–FITC,
anti-p-STAT3 727–FITC, and anti-p-STAT5–FITC. To analyze the populations of B cells,
the tissues were stained with anti-CD4–PerCP, anti-B220-APC, anti-CD138–PE, anti-ICOS–
PE, anti-GL7–FITC, anti-IgD–FITC, anti-IgM–biotin (BD Biosciences, San Jose, CA), and
streptavidin–PerCP. To analyze FcRIIB expression in cells, the tissues were stained with anti-
IL-10–PE, anti-FcRIIB–FITC, anti-CD4–APC, anti-CD19–APC, anti-F4/80–APC, and anti-
CD11c–APC. Stained sections were analyzed using a confocal microscopy system (LSM 510
Meta, Carl Zeiss). All images were analyzed with the MetaMorph software (Molecular
Devices, PA, USA).
Statistical analysis. All data were expressed as the mean ± SD. Statistical analysis
was performed using SPSS 10.0 for Windows (IBM Corp., Armonk, NY). Comparing
numerical data between groups was performed with nonparametric Mann-Whitney tests.
Statistical analysis was performed using SPSS 10.0 for Windows (SPSS, Chicago, IL, USA).
Page 9 of 32
John Wiley & Sons
Arthritis & Rheumatology

10
P values <0.05 were considered significant.
Page 10 of 32
John Wiley & Sons
Arthritis & Rheumatology

11
RESULTS
Prolonged IVIG-induced suppression of CIA and decreased expression of
inflammatory cytokines. We examined the effect of IVIG in the CIA animal model. IVIG
was given to CIA mice once on day 7 after the primary immunization. The arthritis score and
the incidence of arthritis were significantly lower in IVIG-treated mice compared with the
untreated group (Figure 1A). The single injection of IVIG after the first immunization
suppressed the arthritis score for >15 weeks.
Consistent with the arthritis score, the histological observations of tissues stained
with H&E, toluidine blue, and Safranin O showed less inflammatory infiltration and cartilage
damage in IVIG-treated CIA mice compared with the untreated group (Figure 1C). In
particular, the levels of CII antigen-specific IgG1 and IgG2a were decreased (Figure 1B). The
number of TRAP-positive cells was also lower in joint tissues from IVIG-treated mice
(Figure 1D). Next, we observed the effects of IVIG on the expression of inflammatory
cytokines in joint tissues of IVIG-treated CIA and CIA mice. The number of cells staining
positively for IL-1β, IL-6, TNF-α, and IL-17 in the immunohistochemically were lower in
joint tissues from IVIG-treated mice compared with CIA mice (Figure 1E). The mRNA levels
of IL-1β, IL-6, and TNF-α were also lower in IVIG-treated mice (Figure 1F). The mRNA
level of FcRIIB was higher in IVIG-treated mice (Figure 1G). These results suggest that
IVIG suppressed the induction and inflammation of CIA.
Counterregulatory effects of IVIG on Th17 and Treg cells in CIA mice. We
investigated the effects of IVIG on Th17 and Foxp3+ Treg cell populations. Confocal
microscopic examination and FACs analysis showed significantly more Th17 cells in spleens
of untreated CIA mice than in IVIG-treated CIA mice. By contrast, more Foxp3+ Treg cells
Page 11 of 32
John Wiley & Sons
Arthritis & Rheumatology

12
were found in spleens of IVIG-treated mice than in untreated CIA mice (Figure 2A, B).
Confocal microscopic examination also showed more STAT3+ cells and fewer STAT5
+ cells
in spleens of untreated CIA mice than in IVIG-treated CIA mice (Figure 2C). All images were
analyzed with the MetaMorph software.
Serum IL-17 level also decreased by IVIG treatment (Figure 2D), but the mRNA
levels of IL-10 and suppressor of cytokine signaling 3 (SOCS3) increased in the serum from
IVIG-treated mice (Figure 2E). Confocal microscopic examination and FACs analysis of the
spleen showed more CD4+CD25
+Foxp3
+IL-10
+ Treg cells in IVIG-treated CIA mice than in
untreated CIA mice (Figure 2F, G). These results suggest that these effects seemed to be
related to counterregulatory control of Th17 and Treg cells through STAT3 and STAT5.
Regulatory effects of IVIG on immature and mature B cells. We investigated the
effects of IVIG on B cell populations. Confocal microscopic examination showed fewer
CD138+ plasma B cells and GL-7
+ GC B cells in spleens of IVIG-treated CIA mice. By
contrast, more IgM+B220
+ immature B cells were seen in the spleens of IVIG-treated mice
(Figure 3A). The B220+GL7
+ GC B cells significantly decreased in IVIG-treated CIA (Figure
3B). Additionally, there were fewer IL-17- and IFN-γ-expressing TFH cells and more Foxp3-
expressing TFH cells in the spleen from IVIG-treated mice (Figure 3C). In FACs analysis,
CD4+CXCR5
+PD-1
+ TFH cells were decreased in IVIG-treated. There were fewer IL-17-
expressing TFH cells and more Foxp3-expressing TFH cells increased (Figure 3D, E). These
results suggest that IVIG can control the production of pathogenic B cells in the GC of the
spleen by regulating TFH cells.
Upregulation of IL-10 and FcγγγγIIB by IVIG. IL-10 expression was significantly
increased in the spleen of IVIG-treated mice (Figure 4A). Double staining showed a
Page 12 of 32
John Wiley & Sons
Arthritis & Rheumatology

13
significant increase in the number of CD4+IL-10
+ cells and F4/80
+IL-10
+ cells, suggesting
that CD4+ T cells and macrophages are the main source of IL-10 production induced by IVIG
(Figure 4B). FcγIIB expression was increased in CD11c+IL-10
+ cells and F4/80
+IL-10
+ cells
in the spleen from IVIG-treated CIA mice (Figure 4C). All images were analyzed with
MetaMorph software.
Requirement for IL-10 in the treatment effects of IVIG. We generated CIA in IL-
10 KO mice to examine whether IVIG maintains its treatment effects on arthritis induced in
IL-10 KO mice. IVIG was given to IL-10 KO CIA mice in the same manner as for the wild-
type CIA mice. There was no significant difference between the arthritis score and the
incidence of arthritis between IVIG-treated and untreated groups (Figure 5A). Consistent
with the arthritis score, histological findings and TRAP staining showed no difference
between the IVIG-treated CIA and the untreated groups (Figure 5B). The IgG concentration
did not differ significantly between groups (Figure 5C). Flow cytometric analysis showed
similar numbers of Th17 cells and Foxp3+ Treg cells in the spleens in the two groups (Figure
5D).
Page 13 of 32
John Wiley & Sons
Arthritis & Rheumatology

14
DISCUSSION
In our experiments, we observed the effects of IVIG on CIA. IVIG decreased the
severity and incidence of arthritis for a prolonged period in this CIA animal model. IVIG also
decreased osteoclastogenesis, joint destruction, and the expression of inflammatory cytokines
TNF-α, IL-1β, IL-6, and IL-17 in joint tissues. IVIG increased the number of Treg cells with
a decrease in the number of Th17 cells causing a marked increase in the Treg:Th17 cell ratio.
Similarly, IVIG increased the expression of STAT5, the signal molecule essential for Treg cell
generation, but decreased the expression of STAT3, the signal molecule for Th17 generation.
The number of Foxp3+ TFH cells increased and subsequent induction of immature B cells in
the GC was observed in spleens of IVIG-treated mice. IVIG increased IL-10 expression, and
IL-10 KO mice showed no effects of IVIG, indicating that IL-10 is an essential factor in the
treatment effects of IVIG.
The therapeutic effects of IVIG in various autoimmune diseases are known, however,
the mechanism responsible for these therapeutic effects has not been elucidated. IVIG
interacts with the innate and adaptive immune systems in various ways (31). Recent reports
have shown that IVIG expands the CD4+CD25
+ Treg cell population (32) and decreases the
Th17 cell population (25).
We focused on the regulating effects of IVIG in T cells (26, 32) because T cells play
important roles in the pathogenesis of inflammatory arthritis. In an autoimmune
encephalomyelitis model, the number of CD4+CD25
+Foxp3
+ Treg cells increased in the
peripheral blood and the therapeutic effect of IVIG disappeared when Treg cells were
depleted (32) suggesting that Treg cells play a key role in the therapeutic effects of IVIG.
These experiments also reproduced the enhancing effect of IVIG on Treg cells. In the spleens
of IVIG-treated mice, the number of CD4+CD25
+Foxp3
+ Treg cells increased significantly. In
addition to the size of the Treg cell population, the Treg:Th17 cell ratio is also important in
Page 14 of 32
John Wiley & Sons
Arthritis & Rheumatology

15
RA pathogenesis.
IVIG also inhibited Th17 cell generation in vitro (25). The Th17 cell population
decreased markedly in the spleens of IVIG-treated mice. The major cytokine produced by
Th17 cells, IL-17, upregulates synovial inflammation and bone injury by promoting
osteoclastogenesis (18, 19). We postulate that skewing the balance toward Treg cells and the
simultaneous decrease in Th17 cell number are responsible for the treatment effects of IVIG
on CIA. This is the first report to show a simultaneous regulatory effect of IVIG on Th17 and
Treg cells, and the ratio of these two cell types. An imbalance between Th17 and Treg cells
has been previously reported in patients with Kawasaki disease (33), an inflammatory disease
for which IVIG has a remarkable therapeutic effect. Therefore, it is possible that the
treatment effects of IVIG may be extended to patients with other inflammatory diseases with
a Treg:Th17 imbalance.
Autoimmune diseases are characterized as the loss of self-tolerance and generation of
autoreactive B cells that produce autoantibodies (34). TFH cells play an important role in the
selection of B cell clones in GCs. Dysregulated TFH cells have been found during the
development of systemic autoimmune disease including RA (24, 35). Surface molecules and
cytokines expressed on TFH cells determine the characteristics of these cells (24). We
observed a decrease in the number of IL-17- and IFN-γ-expressing TFH cells, but an increase
in the number of Foxp3-expressing TFH cells in the spleen of IVIG-treated mice. TFH cells
expressing Foxp3 have been reported to suppress the GC reaction (36).
Th cell differentiation from naïve CD4+ T cells is affected by microenvironmental
cytokines, which signal through STAT or other transcription factors, leading to the
differentiation to specific types of Th cells, which reciprocally inhibit the alternate
differentiation pathway. The proinflammatory cytokines IL-1β, IL-6, and IL-23 are known to
Page 15 of 32
John Wiley & Sons
Arthritis & Rheumatology

16
be important to Th17 cell generation and Treg cell suppression, in which IL-6 plays a pivotal
role in the reciprocal relationship between Th17 and Treg cell generation (37). IL-6
concentration increased markedly in synovial membranes of RA patients favouring Th17
differentiation within the intra-articular environment (38). Both Th17 and TFH lineages
require IL-6, IL-21, and STAT3 (39) although Bcl6 acts as the specific transcriptional
regulator for TFH differentiation (39, 40). By contrast, STAT5 efficiently inhibits Th17 cells
(41) and TFH cells by inhibiting Blimp-1, a TFH cell suppressor (42). Mice with STAT5
deficiency show impairment of B cell tolerance. In our experiment, IVIG induced the
expression of STAT5 and suppressed the expression of STAT3, which explains the shifts to
Treg cells and Foxp3+ TFH cells.
FcγRs are important in many antibody-directed effector functions and blocking
FcγRs is effective in the treatment of inflammatory and autoimmune diseases. The anti-
inflammatory activity of IVIG is more closely linked to the upregulation of FcγIIB, the
inhibitory receptor (1). IVIG induces the expression of FcγRIIB on macrophages (6, 43). In
our experiments, the upregulation of FcγRIIB was seen in CD11C+ dendritic cells of IVIG-
treated mice and in F4/80+ macrophages.
Increased expression of FcRIIB is related to the decreased production of
autoantibodies by inhibition of the GC and GC B cell activation (44). We observed that the
GC of spleens of IVIG-treated mice was markedly inhibited and the expression of FcRIIB
and IL-10 in B19+ B cells increased (data not shown). Therefore, the anti-inflammatory
effects of FcRIIB and IL-10 seem to suppress GC B cells and the subsequent suppression of
GC B cells may explain the impaired production of CII-specific IgG in IVIG-treated mice.
We propose that IVIG controls adaptive immunity directly by regulating T and B cells in
addition to antigen-presenting cells. This finding suggests that induction of FcγRIIB in
Page 16 of 32
John Wiley & Sons
Arthritis & Rheumatology

17
antigen-presenting cells is induced by IVIG and that this may be one explanation for the
treatment effects of IVIG.
Various cytokines are important in the pathogenesis of RA. IL-10 plays a role by
preventing inflammation and immune-mediated damage (45, 46). We have reported that IL-
10 plays an important role in the generation of Treg cells in RA (47). IL-10 has been shown
to effectively block the activation and effector function of T cells, monocytes, and
macrophages (48) to suppress Th17 cells, and to promote Treg cells within the CD4+ T cell
population in RA patients and a murine RA model (47, 49).
There have been few therapeutic trials of IL-10 in the treatment of RA even though
IL-10 is a potent anti-inflammatory cytokine. In our experiments, the development of CD4+ T
cells polarized toward Treg cells and subsequent therapeutic effects of IVIG were not
reproduced in IL-10 KO mice, indicating that IL-10 has critical effects on CD4+ T cell
development into Th17 or Treg cells.
The duration of the effect of IVIG in CIA mice lasted for >15 weeks, suggesting that
IVIG given in the early phase of disease has significant disease-controlling effects. The single
injection of IVIG showed continuous immunomodulatory effects by regulating macrophages,
B cells, and T cells.
In conclusion, our study showed that IVIG has treatment efficacy in CIA by
increasing the Treg:Th17 cell ratio and by reducing the population of pathogenic B cells by
modulating TFH cells. Our study suggests that IVIG may be a treatment option for patients
with inflammatory arthritis. The clinical applications of IVIG in treating RA should be
evaluated further.
Page 17 of 32
John Wiley & Sons
Arthritis & Rheumatology

18
AUTHOR CONTRIBUTIONS
All authors were involved in drafting the article or revising it critically for important
intellectual content.All of the authors have approved the final version to be published. M-L
Cho had full access to all of the data in the study and takes responsibility for the integrity of
the data and the accuracy of the data analysis.
Study conception and design. Seon-Yeong Lee, Young Ok Jung, Mi-La Cho
Acquisition of data. Seon-Yeong Lee, Jun-Geol Ryu, Chang-Min Kang, Eun-Kyung Kim,
Hye-Jin Son, Eun-Ji Yang, Young-Sun Kang
Analysis and Interpretation of data. Seon-Yeong Lee, Young-Ok Kim, Eun-Kyung Kim, Ji-
Hyeon Ju, Sung-Hwan Park, Ho-Youn Kim, Mi-La Cho
Page 18 of 32
John Wiley & Sons
Arthritis & Rheumatology

19
REFERANCES
1. Gelfand EW. Intravenous immune globulin in autoimmune and inflammatory
diseases. N Engl J Med.367(21):2015-25.
2. Nimmerjahn F, Ravetch JV. Anti-inflammatory actions of intravenous
immunoglobulin. Annu Rev Immunol. 2008;26:513-33.
3. Hundt M, Manger K, Dorner T, Grimbacher B, Kalden P, Rascu A, et al. Treatment
of acute exacerbation of systemic lupus erythematosus with high-dose intravenous
immunoglobulin. Rheumatology (Oxford). 2000;39(11):1301-2.
4. Levy Y, Sherer Y, Ahmed A, Langevitz P, George J, Fabbrizzi F, et al. A study of 20
SLE patients with intravenous immunoglobulin--clinical and serologic response. Lupus.
1999;8(9):705-12.
5. Levy Y, Sherer Y, George J, Langevitz P, Ahmed A, Bar-Dayan Y, et al. Serologic and
clinical response to treatment of systemic vasculitis and associated autoimmune disease with
intravenous immunoglobulin. Int Arch Allergy Immunol. 1999;119(3):231-8.
6. Samuelsson A, Towers TL, Ravetch JV. Anti-inflammatory activity of IVIG mediated
through the inhibitory Fc receptor. Science. 2001;291(5503):484-6.
7. Shioji K, Kishimoto C, Sasayama S. Fc receptor-mediated inhibitory effect of
immunoglobulin therapy on autoimmune giant cell myocarditis: concomitant suppression of
the expression of dendritic cells. Circ Res. 2001;89(6):540-6.
8. Finberg RW, Newburger JW, Mikati MA, Heller AH, Burns JC. Effect of high doses
of intravenously administered immune globulin on natural killer cell activity in peripheral
blood. J Pediatr. 1992;120(3):376-80.
9. Casadei DH, del CRM, Opelz G, Golberg JC, Argento JA, Greco G, et al. A
randomized and prospective study comparing treatment with high-dose intravenous
immunoglobulin with monoclonal antibodies for rescue of kidney grafts with steroid-resistant
Page 19 of 32
John Wiley & Sons
Arthritis & Rheumatology

20
rejection. Transplantation. 2001;71(1):53-8.
10. Sokos DR, Berger M, Lazarus HM. Intravenous immunoglobulin: appropriate
indications and uses in hematopoietic stem cell transplantation. Biol Blood Marrow
Transplant. 2002;8(3):117-30.
11. Bach JF. Regulatory T cells under scrutiny. Nat Rev Immunol. 2003;3(3):189-98.
12. Sakaguchi S. Control of immune responses by naturally arising CD4+ regulatory T
cells that express toll-like receptors. J Exp Med. 2003;197(4):397-401.
13. Mottonen M, Heikkinen J, Mustonen L, Isomaki P, Luukkainen R, Lassila O. CD4+
CD25+ T cells with the phenotypic and functional characteristics of regulatory T cells are
enriched in the synovial fluid of patients with rheumatoid arthritis. Clin Exp Immunol.
2005;140(2):360-7.
14. Kelchtermans H, Geboes L, Mitera T, Huskens D, Leclercq G, Matthys P. Activated
CD4+CD25+ regulatory T cells inhibit osteoclastogenesis and collagen-induced arthritis. Ann
Rheum Dis. 2009;68(5):744-50.
15. Nakae S, Nambu A, Sudo K, Iwakura Y. Suppression of immune induction of
collagen-induced arthritis in IL-17-deficient mice. J Immunol. 2003;171(11):6173-7.
16. Nakae S, Saijo S, Horai R, Sudo K, Mori S, Iwakura Y. IL-17 production from
activated T cells is required for the spontaneous development of destructive arthritis in mice
deficient in IL-1 receptor antagonist. Proc Natl Acad Sci U S A. 2003;100(10):5986-90.
17. Fossiez F, Djossou O, Chomarat P, Flores-Romo L, Ait-Yahia S, Maat C, et al. T cell
interleukin-17 induces stromal cells to produce proinflammatory and hematopoietic cytokines.
J Exp Med. 1996;183(6):2593-603.
18. Katz Y, Nadiv O, Beer Y. Interleukin-17 enhances tumor necrosis factor alpha-
induced synthesis of interleukins 1,6, and 8 in skin and synovial fibroblasts: a possible role as
a "fine-tuning cytokine" in inflammation processes. Arthritis Rheum. 2001;44(9):2176-84.
Page 20 of 32
John Wiley & Sons
Arthritis & Rheumatology

21
19. Adamopoulos IE, Chao CC, Geissler R, Laface D, Blumenschein W, Iwakura Y, et al.
Interleukin-17A upregulates receptor activator of NF-kappaB on osteoclast precursors.
Arthritis Res Ther.12(1):R29.
20. Bettelli E, Carrier Y, Gao W, Korn T, Strom TB, Oukka M, et al. Reciprocal
developmental pathways for the generation of pathogenic effector TH17 and regulatory T
cells. Nature. 2006;441(7090):235-8.
21. Koenen HJ, Smeets RL, Vink PM, van Rijssen E, Boots AM, Joosten I. Human
CD25highFoxp3pos regulatory T cells differentiate into IL-17-producing cells. Blood.
2008;112(6):2340-52.
22. Fazilleau N, Mark L, McHeyzer-Williams LJ, McHeyzer-Williams MG. Follicular
helper T cells: lineage and location. Immunity. 2009;30(3):324-35.
23. Fazilleau N, McHeyzer-Williams LJ, Rosen H, McHeyzer-Williams MG. The
function of follicular helper T cells is regulated by the strength of T cell antigen receptor
binding. Nat Immunol. 2009;10(4):375-84.
24. Zhang X, Ing S, Fraser A, Chen M, Khan O, Zakem J, et al. Follicular helper T cells:
new insights into mechanisms of autoimmune diseases. Ochsner J.13(1):131-9.
25. Maddur MS, Sharma M, Hegde P, Lacroix-Desmazes S, Kaveri SV, Bayry J.
Inhibitory effect of IVIG on IL-17 production by Th17 cells is independent of anti-IL-17
antibodies in the immunoglobulin preparations. J Clin Immunol.33 Suppl 1:S62-6.
26. Kessel A, Ammuri H, Peri R, Pavlotzky ER, Blank M, Shoenfeld Y, et al. Intravenous
immunoglobulin therapy affects T regulatory cells by increasing their suppressive function. J
Immunol. 2007;179(8):5571-5.
27. Siragam V, Brinc D, Crow AR, Song S, Freedman J, Lazarus AH. Can antibodies
with specificity for soluble antigens mimic the therapeutic effects of intravenous IgG in the
treatment of autoimmune disease? J Clin Invest. 2005;115(1):155-60.
Page 21 of 32
John Wiley & Sons
Arthritis & Rheumatology

22
28. Anthony RM, Kobayashi T, Wermeling F, Ravetch JV. Intravenous gammaglobulin
suppresses inflammation through a novel T(H)2 pathway. Nature. 2011;475(7354):110-3.
29. Kim WU, Lee WK, Ryoo JW, Kim SH, Kim J, Youn J, et al. Suppression of collagen-
induced arthritis by single administration of poly(lactic-co-glycolic acid) nanoparticles
entrapping type II collagen: a novel treatment strategy for induction of oral tolerance.
Arthritis and rheumatism. 2002;46(4):1109-20.
30. Camps M, Ruckle T, Ji H, Ardissone V, Rintelen F, Shaw J, et al. Blockade of
PI3Kgamma suppresses joint inflammation and damage in mouse models of rheumatoid
arthritis. Nature medicine. 2005;11(9):936-43.
31. Tha-In T, Bayry J, Metselaar HJ, Kaveri SV, Kwekkeboom J. Modulation of the
cellular immune system by intravenous immunoglobulin. Trends Immunol. 2008;29(12):608-
15.
32. Ephrem A, Chamat S, Miquel C, Fisson S, Mouthon L, Caligiuri G, et al. Expansion
of CD4+CD25+ regulatory T cells by intravenous immunoglobulin: a critical factor in
controlling experimental autoimmune encephalomyelitis. Blood. 2008;111(2):715-22.
33. Jia S, Li C, Wang G, Yang J, Zu Y. The T helper type 17/regulatory T cell imbalance
in patients with acute Kawasaki disease. Clin Exp Immunol.162(1):131-7.
34. Liu Z, Davidson A. Taming lupus-a new understanding of pathogenesis is leading to
clinical advances. Nat Med.18(6):871-82.
35. Ma J, Zhu C, Ma B, Tian J, Baidoo SE, Mao C, et al. Increased frequency of
circulating follicular helper T cells in patients with rheumatoid arthritis. Clin Dev
Immunol.2012:827480.
36. Chung Y, Tanaka S, Chu F, Nurieva RI, Martinez GJ, Rawal S, et al. Follicular
regulatory T cells expressing Foxp3 and Bcl-6 suppress germinal center reactions. Nat
Med.17(8):983-8.
Page 22 of 32
John Wiley & Sons
Arthritis & Rheumatology

23
37. Chen X, Howard OM, Oppenheim JJ. Pertussis toxin by inducing IL-6 promotes the
generation of IL-17-producing CD4 cells. J Immunol. 2007;178(10):6123-9.
38. Houssiau FA, Devogelaer JP, Van Damme J, de Deuxchaisnes CN, Van Snick J.
Interleukin-6 in synovial fluid and serum of patients with rheumatoid arthritis and other
inflammatory arthritides. Arthritis Rheum. 1988;31(6):784-8.
39. Eto D, Lao C, DiToro D, Barnett B, Escobar TC, Kageyama R, et al. IL-21 and IL-6
are critical for different aspects of B cell immunity and redundantly induce optimal follicular
helper CD4 T cell (Tfh) differentiation. PLoS One.6(3):e17739.
40. Crotty S. Follicular helper CD4 T cells (TFH). Annu Rev Immunol.29:621-63.
41. Laurence A, Tato CM, Davidson TS, Kanno Y, Chen Z, Yao Z, et al. Interleukin-2
signaling via STAT5 constrains T helper 17 cell generation. Immunity. 2007;26(3):371-81.
42. Johnston RJ, Choi YS, Diamond JA, Yang JA, Crotty S. STAT5 is a potent negative
regulator of TFH cell differentiation. J Exp Med.209(2):243-50.
43. Bruhns P, Samuelsson A, Pollard JW, Ravetch JV. Colony-stimulating factor-1-
dependent macrophages are responsible for IVIG protection in antibody-induced autoimmune
disease. Immunity. 2003;18(4):573-81.
44. Espeli M, Clatworthy MR, Bokers S, Lawlor KE, Cutler AJ, Kontgen F, et al.
Analysis of a wild mouse promoter variant reveals a novel role for FcgammaRIIb in the
control of the germinal center and autoimmunity. J Exp Med.209(12):2307-19.
45. Fiorentino DF, Zlotnik A, Mosmann TR, Howard M, O'Garra A. IL-10 inhibits
cytokine production by activated macrophages. J Immunol. 1991;147(11):3815-22.
46. Fiorentino DF, Zlotnik A, Vieira P, Mosmann TR, Howard M, Moore KW, et al. IL-
10 acts on the antigen-presenting cell to inhibit cytokine production by Th1 cells. J Immunol.
1991;146(10):3444-51.
47. Heo YJ, Joo YB, Oh HJ, Park MK, Heo YM, Cho ML, et al. IL-10 suppresses Th17
Page 23 of 32
John Wiley & Sons
Arthritis & Rheumatology

24
cells and promotes regulatory T cells in the CD4+ T cell population of rheumatoid arthritis
patients. Immunol Lett.127(2):150-6.
48. Moore KW, de Waal Malefyt R, Coffman RL, O'Garra A. Interleukin-10 and the
interleukin-10 receptor. Annu Rev Immunol. 2001;19:683-765.
49. Gu Y, Yang J, Ouyang X, Liu W, Li H, Bromberg J, et al. Interleukin 10 suppresses
Th17 cytokines secreted by macrophages and T cells. Eur J Immunol. 2008;38(7):1807-13.
Page 24 of 32
John Wiley & Sons
Arthritis & Rheumatology

25
FIGURE LEGENDS
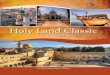
Figure 1. IVIG suppressed induction of CIA and expression of inflammatory cytokines. IVIG
was injected i.v. once 7 days after CIA induction (number of mice per experiment=6). (A)
Arthritis severity was recorded as the mean arthritis index score and incidence score. (B)
Total IgG, IgG1, and IgG2a, and CII-specific IgG, IgG1, and IgG2a concentrations were
measured in serum. (C, D) Ankle joint tissues were obtained from CIA and IVIG-treated
mice in week 15 and stained with toluidine blue, Safranin O, H&E, and TRAP. The
inflammation and cartilage scores are shown in bar graphs (right). (E) Joint tissue from each
group was stained immunohistochemically with specific antibodies to TNF-α, IL-1β, IL-6,
and IL-17. (F, G) mRNA levels of TNF-α, IL-1β, IL-6, and FcγRIIB were analyzed by real-
time PCR. Data represent the mean ± SD of three independent experiments (*P < 0.05, **P <
0.005).
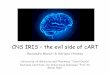
Figure 2. Counterregulatory effects of IVIG on Th17 and Treg cells in CIA. Spleen tissue was
obtained from each group in week 15. (A) The tissues were stained with specific antibody to
CD4 (red or green), CD25 (blue), IFNγ (green), IL-4 (green), Foxp3 (green), or IL-17 (red).
(B) Isolated spleen single cells were stained with CD4–PerCP, IFNγ-APC, IL-4-PE, IL-17-
FITC, CD25–APC, and Foxp3–PE for T helper cells analysis (C) For analysis of STAT-
positive T cells, the tissues were stained with specific antibodies for CD4 (red) and p-STAT3
727 (green), p-STAT3 705 (green), or p-STAT5 (green). Yellow-colored cells were considered
to be activated STAT-positive T cells. (D) In week 15, serum was collected from the mice,
and the protein level of IL-17 was measured by ELISA. (E) mRNA levels of IL-10 and
SOCS3 were measured by real-time PCR. (F) For IL-10-positive Treg cells, spleen tissues
were stained with specific antibodies to CD4 (red), CD25 (blue), Foxp3 (green), and IL-10
Page 25 of 32
John Wiley & Sons
Arthritis & Rheumatology

26
(white). (G) Isolated spleen single cells were stained with CD4–PerCP, CD25–FITC, Foxp3–
PE and IL-10-APC. Positive cells of all confocal Images were analyzed with MetaMorph
software. Three images were analyzed and the percentage of showing positive cell in each
image was measured. Data are expressed as the mean ± SD of three independent experiments
(*P < 0.05, **P < 0.005).
Figure 3. Regulatory effects of IVIG on immature and mature B cells. To examine the effect
of IVIG on B cell activation and GC formation, spleen tissues were stained with B cell-
specific antibodies. (A) To analyze GC formation and B cell phenotype, the tissues were
stained with specific antibodies to CD4 (white), B220 (blue), CD138 (red), ICOS (red), GL-7
(green), IgM (green), and IgD (white). (B) For GC B cells, spleen single cells were stained
with specific antibodies to B220-APC, GL7-FITC. (C) To analyze TFH cells in the GC, spleen
tissues were stained with antibodies to CD4 (blue), B220 (white), GL-7 (green), IFNγ (red),
IL-17(red), and Foxp3(red). (D, E) Spleen single cells were stained with CD4-PerCP,
CXCR5-APC, PD-1-FITC, IL-17-PE or Foxp3-PE for subtypes of TFH cells. Data are
expressed as the mean ± SD of three independent experiments (*P < 0.05, **P < 0.005).
Figure 4. Upregulation of IL-10 and FcγRIIB by IVIG. (A) Spleen tissues were stained
immunohistochemically with specific antibodies to IL-10. (B) To analyze IL-10-positive cells,
spleen tissues were stained with specific antibodies to IL-10, CD4, CD19, CD11c, and F4/80.
(C) Spleen tissue was stained with antibodies to CD11c, F4/80, IL-10, and FcγRIIB. Positive
cells of all confocal Images were analyzed with MetaMorph software. Three images were
analyzed and the percentage of showing positive cell in each image was measured. Data are
expressed as the mean ± SD of three independent experiments (*P < 0.05, **P < 0.005).
Page 26 of 32
John Wiley & Sons
Arthritis & Rheumatology

27
Figure 5. Requirement of IL-10 for the treatment effects of IVIG. CIA was induced in IL-10
KO mice, and IVIG was injected i.v. once 7 days after CIA induction (number of mice per
experiment=6). (A) Arthritis severity was recorded as the mean arthritis index score and
incidence score. (B) Ankle joint tissues were obtained from CIA and IVIG-treated mice in
week 15 and stained with toluidine blue, Safranin O, H&E, and TRAP. The inflammation and
cartilage scores are shown in bar graphs (right). (C) Total IgG, IgG1, and IgG2a levels were
measured in serum from each group. (D) Isolated spleen single cells were stained with CD4–
PerCP, CD25–APC, Foxp3–FITC, and IL-17–PE to analyze the Treg and Th17 cells. Data are
expressed as the mean ± SD of three independent experiments (*P < 0.05, **P < 0.005).
Page 27 of 32
John Wiley & Sons
Arthritis & Rheumatology

Figure 1. IVIG suppressed induction of CIA and expression of inflammatory cytokines. IVIG was injected i.v. once 7 days after CIA induction (number of mice per experiment=6). (A) Arthritis severity was recorded as the mean arthritis index score and incidence score. (B) Total IgG, IgG1, and IgG2a, and CII-specific IgG,
IgG1, and IgG2a concentrations were measured in serum. (C, D) Ankle joint tissues were obtained from CIA and IVIG-treated mice in week 15 and stained with toluidine blue, Safranin O, H&E, and TRAP. The
inflammation and cartilage scores are shown in bar graphs (right). (E) Joint tissue from each group was stained immunohistochemically with specific antibodies to TNF-α, IL-1β, IL-6, and IL-17. (F, G) mRNA levels of TNF-α, IL-1β, IL-6, and FcγRIIB were analyzed by real-time PCR. Data represent the mean ± SD of three
independent experiments (*P < 0.05, **P < 0.005). 287x411mm (300 x 300 DPI)
Page 28 of 32
John Wiley & Sons
Arthritis & Rheumatology

Figure 2. Counterregulatory effects of IVIG on Th17 and Treg cells in CIA. Spleen tissue was obtained from each group in week 15. (A) The tissues were stained with specific antibody to CD4 (red or green), CD25 (blue), IFNγ (green), IL-4 (green), Foxp3 (green), or IL-17 (red). (B) Isolated spleen single cells were
stained with CD4–PerCP, IFNγ-APC, IL-4-PE, IL-17-FITC, CD25–APC, and Foxp3–PE for T helper cells analysis (C) For analysis of STAT-positive T cells, the tissues were stained with specific antibodies for CD4
(red) and p-STAT3 727 (green), p-STAT3 705 (green), or p-STAT5 (green). Yellow-colored cells were considered to be activated STAT-positive T cells. (D) In week 15, serum was collected from the mice, and
the protein level of IL-17 was measured by ELISA. (E) mRNA levels of IL-10 and SOCS3 were measured by real-time PCR. (F) For IL-10-positive Treg cells, spleen tissues were stained with specific antibodies to CD4
(red), CD25 (blue), Foxp3 (green), and IL-10 (white). (G) Isolated spleen single cells were stained with CD4–PerCP, CD25–FITC, Foxp3–PE and IL-10-APC. Positive cells of all confocal Images were analyzed with
MetaMorph software. Three images were analyzed and the percentage of showing positive cell in each image was measured. Data are expressed as the mean ± SD of three independent experiments (*P < 0.05, **P <
Page 29 of 32
John Wiley & Sons
Arthritis & Rheumatology

0.005). 276x377mm (300 x 300 DPI)
Page 30 of 32
John Wiley & Sons
Arthritis & Rheumatology

Figure 3. Regulatory effects of IVIG on immature and mature B cells. To examine the effect of IVIG on B cell activation and GC formation, spleen tissues were stained with B cell-specific antibodies. (A) To analyze GC
formation and B cell phenotype, the tissues were stained with specific antibodies to CD4 (white), B220
(blue), CD138 (red), ICOS (red), GL-7 (green), IgM (green), and IgD (white). (B) For GC B cells, spleen single cells were stained with specific antibodies to B220-APC, GL7-FITC. (C) To analyze TFH cells in the GC,
spleen tissues were stained with antibodies to CD4 (blue), B220 (white), GL-7 (green), IFNγ (red), IL-17(red), and Foxp3(red). (D, E) Spleen single cells were stained with CD4-PerCP, CXCR5-APC, PD-1-FITC,
IL-17-PE or Foxp3-PE for subtypes of TFH cells. Data are expressed as the mean ± SD of three independent experiments (*P < 0.05, **P < 0.005).
249x305mm (300 x 300 DPI)
Page 31 of 32
John Wiley & Sons
Arthritis & Rheumatology

Figure 4. Upregulation of IL-10 and FcγRIIB by IVIG. (A) Spleen tissues were stained immunohistochemically with specific antibodies to IL-10. (B) To analyze IL-10-positive cells, spleen tissues were stained with specific antibodies to IL-10, CD4, CD19, CD11c, and F4/80. (C) Spleen tissue was stained
with antibodies to CD11c, F4/80, IL-10, and FcγRIIB. Positive cells of all confocal Images were analyzed with MetaMorph software. Three images were analyzed and the percentage of showing positive cell in each image was measured. Data are expressed as the mean ± SD of three independent experiments (*P < 0.05, **P <
0.005). 210x226mm (300 x 300 DPI)
Page 32 of 32
John Wiley & Sons
Arthritis & Rheumatology

Figure 5. Requirement of IL-10 for the treatment effects of IVIG. CIA was induced in IL-10 KO mice, and IVIG was injected i.v. once 7 days after CIA induction (number of mice per experiment=6). (A) Arthritis severity was recorded as the mean arthritis index score and incidence score. (B) Ankle joint tissues were
obtained from CIA and IVIG-treated mice in week 15 and stained with toluidine blue, Safranin O, H&E, and TRAP. The inflammation and cartilage scores are shown in bar graphs (right). (C) Total IgG, IgG1, and
IgG2a levels were measured in serum from each group. (D) Isolated spleen single cells were stained with CD4–PerCP, CD25–APC, Foxp3–FITC, and IL-17–PE to analyze the Treg and Th17 cells. Data are expressed
as the mean ± SD of three independent experiments (*P < 0.05, **P < 0.005). 228x260mm (300 x 300 DPI)
Page 33 of 32
John Wiley & Sons
Arthritis & Rheumatology












![Treg cells maintain selective access to IL-2 and immune homeostasis … · survival signals downstream of IL-2 signaling maintain Treg cells [4, 5]. Notably, Treg cells cannot make](https://img.pdfslide.us/doc/110x75/5e779032b1981e5188625c5e/treg-cells-maintain-selective-access-to-il-2-and-immune-homeostasis-survival-signals.jpg)