Embed Size (px)
Citation preview

J. Anat. (2001) 198, pp. 491–495, with 5 figures Printed in the United Kingdom 491
Short Report
Intrathymic lymph nodes in humans
A. TANEGASHIMA1, I . USHIYAMA2, Y. KIKUI1 AND H. YAMAMOTO1
"Department of Forensic Medicine and Sciences, Mie University School of Medicine, Mie, and
#Department of Legal Medicine, Shiga University of Medical Science, Shiga, Japan
(Accepted 14 November 2000)
An unusual lymph node exists in the centre of the human thymus. This lymph node, which we call an
intrathymic lymph node (ITLN), possesses some interesting morphological characteristics. In ontogeny, this
node seems to appear at the latter half of fetal period. The function of the ITLN is still unknown, but it is
assumed that it may play a different role in the immune system than other peripheral lymph nodes by
its characteristics.
Key words : Lymphatic system; thymus.
The human thymus is located in the anterior medias-
tinum and overlies the pericardium. It comprised of
right and left lobes which are completely invested by
fibrous capsules, and each lobe is subdivided by septa
from the capsule into many lobuli. The upper portion
(cervical thymus) and the lower portion (thoracic
thymus) are clearly divided by septa containing large
blood vessels. We have previously reported the
existence of several lymph nodes, called parathymic
lymph nodes (PTLNs), located at the apex of the
cervical lobes or between the cervical and thoracic
lobes, and some interesting characteristics of those
lymph nodes (Tanegashima et al. 1999). In this study,
we made sequential sections of the whole thymus, and
discovered the existence of the intrathymic lymph
node (ITLN) located in the centre of the thymus.
All thymus samples were obtained from cadavers
during autopsy in the Osaka Medical Examiner’s
Office, Department of Forensic Medicine and
Sciences, Mie University School of Medicine, and the
Department of Legal Medicine, Shiga University of
Medical Science. Age, sex and cause of death of each
donor in this study were summarised in the Table.
For Cases 1–5 in the Table, the whole thymus was
Correspondence to Dr Akio Tanegashima, Department of Forensic Medicine and Sciences, Mie University School of Medicine, 2-174,
Edobashi, Tsu, Mie 514-8507, Japan. Tel. : 81-59-232-1111, ex: 6383; fax: 81-59-231-5014; e-mail : tane!doc.medic.mie-u.ac.jp
fixed in 10% phosphate buffered formalin, embedded
in celloidin and 25 µm serial sections were cut. All
sections were stained with haematoxylin and eosin.
For Cases 6–8 in the Table, the whole thymus was
fixed in 10% phosphate buffered formalin, embedded
in paraffin and serial 10 µm sections were cut (Cases 7,
8) or at 15 µm (Case 6). In addition to haematoxylin
and eosin, immunohistochemical staining was per-
formed; deparaffinised sections were treated with
methanol containing 0±3% H#O
#to block endogenous
peroxidase, hydrated and treated with PBS (0±1
phosphate buffered saline) 3 times. They were then
incubated in PBS containing 1% bovine serum
albumin (BSA) for 30 min. After blotting dry with
paper filter, the sections were incubated with mono-
clonal antibody (1:100) at room temperature of 2 h.
Tissue sites reactive with the antibody were visualised
with the streptavidin-biotin-peroxidase complex
method, using the Histofine SAB-PO kit (Nichirei,
Tokyo, Japan). Finally, the sections were counter-
stained with haematoxylin. Anti-CD20 mouse mono-
clonal antibody was perchased from DAKO A}S
(Glostrup, Denmark).
An ITLN was present in all 7 cases except for a fetus
of 5 mo gestational age (Table, Case 7) and was

Table. Age, sex and cause of death of each donor
Case Age Sex Cause of death
1 3 mo Fe Sudden infant death syndrome
2 4 mo M Pneumonia
3 8 mo M Subdural haemorrhage, trauma
4 11 mo Fe Asphyxia
5 15 y Fe Sudden death*
6 31 y Fe Subarachnoid haemorrhage, moyamoya disease
7 Fetus** M Stillbirth
8 Fetus*** Fe The mother’s sudden death
* Unexplained sudden death; cause of death could not be determined at autopsy; ** fetus at 5 mo gestational age; *** fetus at 6 mo
gestational age.
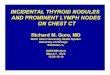
Fig. 1. Thymus obtained from a 3-mo-old infant (Table, Case 1). (a) Macroscopic view of section 275 of 598 sequential sections. The yellow
arrow shows ITLN located in the centre of the thymus, and the red arrow PTLNs located between left cervical and thoracic lobes. (b)
Microscopic view of PTLNs. (c) Microscopic view of ITLN. A large part of this node is dominated by the paracortical area and, in contrast,
only a thin cortex with a few follicles is poorly developed. Medullary cords and sinus are scarce. (d ) High magnification view of the paracortical
area adjacent to the hilus (surrounded by a yellow box in Fig. c). Many blood vessels (yellow arrows) spread radially from the hilus, yielding
HEVs. Medullary cords and sinus are lacking in this area.
492 A. Tanegashima and others

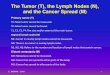
Fig. 2. Thymus obtained from an 11-mo-old infant (Table, Case
3). (a) Macroscopic view of section 220 of 336 sequential sections.
The yellow arrow shows ITLN located in the centre of the thymus,
and the red arrows show PTLNs located at the apex of the cervical
thymus and between left cervical and thoracic lobe. (b) Microscopic
view of ITLN. Germinal centres are relatively more developed
compared with Case 1. Similar to Case 1, a large part of this node
is dominated by the paracortical area, and medullary cords and
sinus are scarce.
always located to the right of the septum dividing the
thymus into left and right lobes. The ITLNs in
postnatal individuals (Table, Cases 1–6) possessed
some morphological characteristics in common (Figs
1c, d, e, 2b, 3a), as all had a well-developed para-
cortical area rich in high endothelial venules (HEVs)
which occupied most parts of this node, and only a
thin cortex with a few follicles. The marginal sinus
showed many macrophage-like cells. It is of interest
that there were few trabeculae, medullary cords or
medullary sinuses. Immunohistochemical staining
with anti-CD20 antibody revealed that the superficial
cortex possessed small-sized follicles containing B
cells and CD20-positive B cells were also present in
the perivascular area (Fig. 3b). These unusual his-
tological findings are similar to those of the human
PTLNs which we have reported previously.
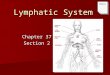
Fig. 3. Thymus obtained from a 4-mo-old infant (Table, Case 2).
(a) Microscopic view of ITLN. A large part of this node is
dominated by the paracortical area and, in contrast, only a thin
cortex with a few follicles are seen. Medullary cord and sinus are
scarce. Haematoxylin and eosin. (b) Immunohistochemical staining
with anti-CD20 antibody. The subcapsular area and small primary
follicles (Fol) are stained. CD20-positive B cells are also present
generally in the perivascular area.
The ITLN was barely detectable in the thymus of a
fetus at 5 mo gestational age in this study (Table,
Case 7), which may suggest that at this fetal age the
ITLN is still in early stages of development and does
not possess sufficient cell density to be detectable. In
the thymus of a fetus at 6 mo gestational age (Table,
Case 8), the ITLN was detected clearly (Fig. 4). At
this fetal age, the cellular density of this node was still
low, but HEVs were well-developed (Fig. 4b). Im-
munohistochemical staining with anti-CD20 antibody
showed that only a few B cells were detected in the
perivascular area but the follicles were not formed in
the ITLN at this fetal age (data not shown). Lymph
nodes in various stage of development can be observed
in a single fetus (Bailey & Weiss, 1975), and therefore,
it is thought that the development of the ITLN may
occur relatively later in ontogeny.
The phylogenesis of the lymphoid tissues starts in
the lower vertebrates (Jonsson & Christensen, 1978),
Intrathymic lymph nodes in humans 493

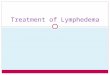
Fig. 4. Thymus obtained from a fetus at 6 mo gestational age
(Table, Case 8). (a) Macroscopic view of the thymus. The yellow
arrow shows the ITLN located in the centre of the thymus, and the
red arrow a PTLN located between left cervical and thoracic lobes.
(b) Microscopic view of ITLN. HEVs are well-developed, but the
cellular density of this node is much less than in postnatal
individuals (see Fig. 1). The developing capsular sinus can be seen.
The nodal capsule is still thin.
but the definitive forms of lymph node-like structures
are first present in the lower mammals. Furthermore,
the ITLN is thought to be first present in the higher
mammals in phylogeny because such lymph nodes
are absent at least in the thymus of rats and mice.
In adults, the ITLN may gradually involute
following thymic involution. It is interesting to
consider that the fatty degeneration of the ITLN may
start from the outer side (Fig. 5), which for peripheral
lymph nodes usually occurs by replacement of the
parenchyma with adipose tissue (Luscieti et al. 1980).
As shown in Figure 5b, replacement with adipose
tissue is seen in the capsule ; the boundary between
ITLN and thymic parenchyma thus becomes less
definite as involution progresses.
It seems likely that the human ITLN and PTLNs
may be located downstream from the thymus, and
that some newborn T cells produced in the thymus
may enter these nodes because it is generally con-
sidered that the human thymus has no afferent
lymphatic vessels (Goldstein & Mackay, 1969;
Fig. 5. Thymus obtained from a 34-y-old adult (Table, Case 6). (a)
Microscopic view of ITLN. (b) High magnification view (sur-
rounded by a green box in a). There is some replacement by adipose
tissue in the capsule and subcapsular area. Arrows show the capsule
infiltrated with adipose tissue. The marginal sinus (*) is filled with
many macrophage-like cells.
Bloodworth et al. 1975). Moreover, self antigens and
some antigen-presenting cells (e.g. macrophages and}or dendritic cells) may also enter these nodes from the
thymus through the lymphatics. On the other hand,
some peripheral lymphocytes may also enter these
nodes through the HEV. Thus these nodes are likely
to be the place for interaction between peripheral
lymphocytes and cells from the thymus.
The role of intra- and parathymic lymph nodes is
still unknown. It is suggested, however, that these
nodes may play a particular role in the immune
system which differs from that of other peripheral
lymph nodes on the basis of the morphological
characteristics of these nodes. Moreover, it is
suggested that the ITLN may be related to some
autoimmune diseases (e.g. myasthenia gravis) with the
development of germinal centres in the thymus.
This work was supported in part by a Grant-in-Aid
for Scientific Research (B)(2) from the Japanese
Ministry of Education, Science, Sports, and Culture.
494 A. Tanegashima and others

We thank Miss Naoko Mizuhara and Miss Misako
Okuno for technical assistance and Dr Steven Rand
for valuable comments and English corrections.
BAILEY RP, WEISS L (1975) Ontogeny of human fetal lymph
nodes. American Journal of Anatomy 142, 15–28.
BLOODWORTH JMB J, HIRATSUKA H, HICKEY RC, WU
J (1975) Ultrastructure of human thymus, thymic tumors, and
myasthenia gravis. In Pathology Annual (ed. Sommers SC), vol.
10, p. 329. New York: Appleton-Century-Crofts.
GOLDSTEIN G, MACKAY IR (1969) The Human Thymus, p. 3.
Heinemann, London.
JONSSON V, CHRISTENSEN BJ (1978) The phylogenetic
evolution of the lymph node. Scandinavian Journal of Hae-
matology 20, 5–12.
LUSCIETI P, HUBSCHMID TH, COTTIER H, HESS MW,
SOBIN LH (1980) Human lymph node morphology as a function
of age and site. Journal of Clinical Pathology 33, 454–461.
TANEGASHIMA A, YAMASHITA A, YAMAMOTO H,
FUKUNAGA T (1999) Human parathymic lymph node:
morphological and functional significance. Immunology 97,
301–308.
Intrathymic lymph nodes in humans 495