Embed Size (px)
Citation preview

ARTICLE
Intrascleral fibrin glue
intraocular lens fixationcombined with Descemet-stripping automatedendothelial keratoplasty or penetratingkeratoplasty
Rajesh Sinha, MD, FRCS, Himanshu Shekhar, MD, Namrata Sharma, MD,Radhika Tandon, MD, FRCSEd, FRCOphth, Jeewan S. Titiyal, MD,
Rasik B. Vajpayee, MS, FRCSEd, FRANZCO
Q
P
1240
2012 Aublished
PURPOSE: To evaluate the outcomes of intrascleral haptic fixation of an intraocular lens (IOL) withfibrin glue combined with penetrating keratoplasty (PKP) or Descemet-stripping automatedendothelial keratoplasty (DSAEK) for aphakic or pseudophakic bullous keratopathy (BKP).
SETTING: Rajendra Prasad Centre for Ophthalmic Sciences, All India Institute of Medical Sciences,New Delhi, India.
DESIGN: Case series.
METHODS: Eyes with BKP had combined PKP or DSAEK with fibrin glue-assisted intrascleral pos-terior chamber (PC) IOL fixation; PKP was performed in eyes with a corneal scar and DSAEK in eyeswithout a scar. The parameters evaluated were corrected distance visual acuity (CDVA), anteriorsegment biomicroscopy, intraocular pressure, central corneal thickness (CCT), and IOL status. In-traoperative events and postoperative complications were recorded.
RESULTS: The study evaluated 11 patients (11 eyes). Intrascleral fixation of a PC IOL with PKP orDSAEK was successfully performed in all eyes; PKP was performed in 6 eyes (54.54%) and DSAEKin 5 eyes. The mean CDVA improved from 1.95 logMAR G 0.29 (SD) to 0.40 G 0.16 logMAR(P<.001). The mean CCT was 0.741 G 0.71 mm preoperatively and 0.579 G 0.20 mm postoper-atively (P<.001). There were no cases of intraoperative or postoperative IOL decentration or othercomplications.
CONCLUSIONS: Fibrin glue-assisted intrascleral fixation of a PC IOL combined with DSAEK or PKPwas a safe, effective method to manage BKP with aphakia or malpositioned IOLs. The IOL fixationwas strong enough to sustain the manipulation required for corneal procedures.
Financial Disclosure: No author has a financial or proprietary interest in any material or methodmentioned.
J Cataract Refract Surg 2012; 38:1240–1245 Q 2012 ASCRS and ESCRS
Bullous keratopathy (BKP) is a major complication ofcataract surgery. In most cases, penetrating kerato-plasty (PKP) or Descemet-stripping automated endo-thelial keratoplasty (DSAEK) are effective surgicalmodalities for treating the condition.1–3 Some casesmay require implantation or exchange of the intraocu-lar lens (IOL). Intraocular lens exchange is recommen-ded in cases with closed-loop IOLs, semiflexibleanterior chamber IOLs (AC IOLs), iris-supportedIOLs, or unstable IOLs because these IOLs have beenincreasingly associated with poor macular function
SCRS and ESCRS
by Elsevier Inc.
postoperatively. Bal�azs et al.3 recommend that theIOL be retained if its position is adequate and the pupilis mobile. In patients with recurrent hemorrhages, un-controlled glaucoma, or chronic iritis resistant to med-ical treatment, the IOL should be removed.
Current techniques for IOL exchange during kerato-plasty, especially in cases with a deficient posteriorcapsule, are less than satisfactory. Transsclerallysutured IOLs have been described in these situa-tions.4,5 However, the technique is associated witha longer learning curve, prolonged intraoperative
0886-3350/$ - see front matter
doi:10.1016/j.jcrs.2012.02.042

1241INTRASCLERAL GLUED IOL WITH CORNEAL PROCEDURES
manipulation, postoperative pseudophacodonesis,and risk for postoperative decentration resultingfrom suture degradation or knot slippage.6–12 To over-come these problems, a new technique of fibrin glue–assisted sutureless fixation of posterior chamberIOLs (PC IOL) in eyes with deficient posterior capsulesupport has been described.13
In this study, we evaluated the technique and out-comes of intrascleral fixation of IOLs with fibringlue combined with corneal transplantation (ie,PKP or DSAEK) for the treatment of endothelialdecompensation.
PATIENTS AND METHODS
This retrospective study analyzed data of consecutive pa-tients who had PKP or DSAEK combined with intrascleralfixation of PC IOLswith fibrin glue for postsurgical endothe-lial decompensation. The study was performed at a tertiarycare ophthalmic hospital. The original surgery was per-formed elsewhere in all cases. The institute's ethics commit-tee approved the study, and all patients provided informedwritten consent.
Patient Evaluation
A detailed examination was performed in all eyes. Theassessment included uncorrected distance visual acuity;corrected distance visual acuity (CDVA); slitlamp biomicro-scopy of the anterior segment; intraocular pressure (IOP);central corneal thickness (CCT); IOL status; fundus evalua-tion, if possible; and ultrasonography to rule out posteriorsegment pathology. Intraoperative events were recordedand evaluated. In the postoperative period, the patientswere evaluated for similar parameters as well as for thepresence of complications.
Surgical Technique
The same surgeon (R.S.) performed all surgeries usingperibulbar anesthesia of 5 mL lignocaine hydrochloride2.0% and 5 mL bupivacaine hydrochloride 0.5% for bothtechniques. The corneal procedure performed was basedon the presence of corneal scarring; PKP was performedin eyes with a corneal scar and DSAEK in eyes withouta scar.
Descemet-Stripping Automated Endothelial Keratoplasty withGlued Intraocular Lens The donor corneoscleral tissuewas mounted on an artificial anterior chamber (MoriaALTK, Moria). A 350 mm head was chosen for the micro-
Submitted: November 6, 2011.Final revision submitted: February 12, 2012.Accepted: February 14, 2012.
From the Rajendra Prasad Centre for Ophthalmic Sciences, All IndiaInstitute of Medical Sciences, New Delhi, India.
Corresponding author: Rajesh Sinha, MD, FRCS, S-7, RajendraPrasad Centre for Ophthalmic Sciences, All India Institute ofMedical Sciences, New Delhi, India. E-mail: [email protected].
J CATARACT REFRACT SURG
keratome (Moria). The lamellar dissection was performedwith the microkeratome. The posterior lamella with thecorneoscleral rim was placed on a polytetrafluoroethylene(Teflon) block with the endothelial side up, and an 8.0 mmdonor lenticule was fashioned using a circular cuttingtrephine.
A temporal approachwas used in all the cases. A 20-gaugeinfusion cannula was placed via a sclerotomy in the infero-temporal area after a limited conjunctival peritomy wasperformed.
A localized peritomy was made near the superior(12 o'clock) and inferior limbus (6 o'clock). The sclera wasmarked 1.5 mm and 3.0 mm from the limbus. Twopartial-thickness radial scleral incisions were created paral-lel to each other between 1.5 mm and 3.0 mm from the lim-bus. A crescent blade was used to perform the lamellardissection between the 2 incisions. The lamellar dissectionwas extended beyond the radial incisions on the temporalaspect on 1 side and on the nasal aspect on the other side.Partial-thickness scleral flaps were raised by cutting theroof of the tunnel at the fornix side to create a limbus-based scleral flap (Figure 1). A 20-gauge microvitreoretinalblade (Alcon Laboratories, Inc.) was used to create 2 sclerot-omies, 1 each in the bed of the flap, 1.5 mm from thelimbus.
The center of the cornea was marked with an 8.00 mm cir-cular cutting disposable corneal trephine. A temporal limbaltunnel was made with a 2.75 mm keratome. A paracentesiswas created at the limbus adjacent to the corneal incision.Trypan blue dye was injected into the anterior chamber tostain Descemet membrane. Descemet membrane and the en-dothelium were scored with a reverse Sinskey hook follow-ing the superficial 8.00 mm mark on the cornea, and themembrane was removed. A limited anterior vitrectomywas performed to clear vitreous strands.
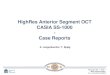
The limbal tunnel was enlarged to 6.0 mm. A multipiecePC IOL was introduced into the anterior chamber witha McPherson forceps. The haptic was then guided into thebent tip of a vitreoretinal forceps introduced through thesuperior sclerotomy site. The haptic was externalizedthrough the sclerotomy site under the superior scleral flap(Figure 2). The second haptic was managed similarly, exter-nalized with the help of a vitreoretinal forceps insertedthrough the inferior sclerotomy and guided into the scleralpocket dissected nasally adjacent to the scleral flap. Thesuperior tip of the haptic was then guided into the dissectedscleral pocket.
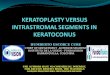
A drop of an ophthalmic viscosurgical device was placedon the endothelial side, and the donor lenticule was folded ina 40/60 fashion. It was held gently with a noncrushing for-ceps and inserted into the anterior chamber (Figure 3). Thedonor lenticule was unfolded and brought into position bygently stroking the cornea. The corneal tunnel was closedwith a single 10-0 monofilament nylon suture. Air was in-jected to fill the anterior chamber and achieve tamponadefor 10 minutes. The reconstituted fibrin glue (Baxter AG)was then injected into the pockets and over the beds of thescleral flap. The scleral flapwas replaced and gentle pressureapplied locally over the flap for 20 to 30 seconds to promoteadherence of the glue to the scleral flaps.
The irrigation cannula was removed and the port closedwith a 6-0 polyglactin suture. The conjunctival flaps wereclosed by sticking them to the sclera with the applicationof fibrin glue. At the end of 10 minutes, 50% of the air inthe chamber was exchanged with saline.
- VOL 38, JULY 2012

Figure 2.Haptic being externalized through the superior sclerotomy.Figure 1. Lamellar scleral flap.
1242 INTRASCLERAL GLUED IOL WITH CORNEAL PROCEDURES
Postoperatively, the patient was asked to remain in a strictsupine position with the face toward the ceiling for 8 to10 hours. Topical moxifloxacin 0.5% 3 times a day, prednis-olone acetate 1.0% eyedrops 4 times a day, tropicamide1.0% eyedrops 2 times a day, and preservative-free lubricat-ing drops 6 times a day were given postoperatively and sub-sequently tapered.
Penetrating Keratoplasty with Glued Intraocular Lens Thedonor tissue was prepared using a manual trephine froma freshly prepared corneoscleral button by punching ona polytetrafluoroethylene block.
The scleral flaps and the adjacent groove were created ina fashion similar to that for DSAEK. The host cornea wastrephined using a 7.2 mm circular cutting disposable tre-phine. A multipiece PC IOL was held with a McPhersonforceps at the pupillary plane with 1 hand and then exter-nalized through the sclerotomy on 1 side and then the otherside with a vitreoretinal forceps inserted through scleroto-my sites, as described earlier. The tips of the haptics were
Figure 3. Donor lenticule being inserted into the anterior chamberwith a vitreoretinal forceps.
J CATARACT REFRACT SURG
tucked into the scleral pocket dissected on both sides. Thegraft was placed, and 10-0 monofilament nylon interruptedcardinal sutures were applied. Similarly, the other 12 su-tures were applied to appose the graft–host junction. The re-constituted fibrin glue was injected through the cannula ofthe double-syringe delivery system under the superior andinferior scleral flaps (Figure 4). Local pressure was appliedover the flaps for 30 seconds to allow adhesion of the flapto the bed. The conjunctiva was also apposed with the glue.
Postoperatively, topical moxifloxacin 0.5% 3 times a day,prednisolone acetate 1.0% eyedrops 4 times a day, tropica-mide 1.0% eyedrops 2 times a day, and preservative-freelubricating drops 6 times a day were prescribed and subse-quently tapered.
RESULTS
The study comprised 11 patients (11 eyes). The meanage of the 7 men (63.63%) and 4 women (36.36%)
Figure 4. Fibrin glue being applied on scleral bed after securing do-nor tissue in PKP with 16 10-0 monofilament nylon interruptedsutures.
- VOL 38, JULY 2012

1243INTRASCLERAL GLUED IOL WITH CORNEAL PROCEDURES
was 64 years (range 54 to 78 years). Table 1 shows thepatient characteristics and surgical outcomes.
Intrascleral fixation of a PC IOL with fibrin gluecombined with PKP or DSAEK was successfully per-formed in all eyes. Penetrating keratoplasty was per-formed in 6 eyes (54.54%). Of these, 1 eye had an ACIOL, 1 had a PC IOL in the anterior chamber, and 2had a decentered PC IOL that required explantation.Descemet-stripping automated endothelial kerato-plasty was performed in 5 eyes, all of which wereaphakic except 1. In the latter case, a decentered PCIOL was present and required explantation.
The mean CDVA improved significantly, from1.95 logMAR G 0.29 (SD) (range 1.3 to 2.3 logMAR)preoperatively to 0.40 G 0.16 logMAR (range 0.18 to0.48 logMAR) postoperatively (P!.001). The meanCCT was 0.741 G 0.71 mm (range 0.633 to0.991 mm) and 0.579 G 0.20 mm (range 0.546 to0.612 mm), respectively (P!.001).
By the 6-month follow-up, all 11 patients had main-tained the 3-month CDVA, all grafts were clear, and allIOLs were well centered (Figures 5 and 6). There wereno keratoplasty-related problems (infection, rejection,dehiscence) or IOL-related complications (vitreousincarceration, endophthalmitis, subluxation, hapticextrusion). There were no cases of intraoperative orpostoperative IOL decentration.
DISCUSSION
At the end of the 1990s, pseudophakic bullouskeratopathy (PBK) was the most important indicationfor PKP14–17 because of the high rate of AC IOLimplantation in the 1980s. In the past few years, the
Table 1. Patient details and surgical outcomes.
Preoperat
Pt Age (Y) Sex IndicationCornealSurgery
CDVA(LogMAR)
CCT(mm)
1 62 F ABK DSAEK 2.00 8202 54 M ABK DSAEK 1.78 7883 74 M PBK PKP 2.30 6424 66 M ABK PKP 2.30 6335 56 F ABK DSAEK 1.78 7926 60 M PBK DSAEK 2.00 8327 64 M ABK PKP 2.00 7128 63 M PBK PKP 1.78 6979 59 M ABK DSAEK 1.30 76310 70 F PBK PKP 2.30 67811 78 F PBK PKP 2.00 798
ABKZ aphakic bullous keratopathy; AC IOLZ anterior chamber intraocular lens;DSAEK Z Descemet-stripping automated endothelial keratoplasty; IOL Z intraocopathy; PC IOL Z posterior chamber intraocular lens; PKP Z penetrating keratop
J CATARACT REFRACT SURG
surgical options for endothelial decompensationhave changed significantly. At present, DSAEK isthe procedure of choice to manage endothelial dis-eases such as Fuchs endothelial dystrophy, PBK,and endothelial graft failure. The advantages ofDSAEK over PKP include faster visual recovery,relative refractive neutrality, increased intraoperativesafety, and a smaller incision (5.0 mm), which leavesthe eye stronger and less prone to traumatic rup-ture.18,19 However, in the presence of a dense cornealscar, PKP is the only surgical option because thevisual axis clarity is inadequate for DSAEK. In ourseries, 6 of 11 patients had PKP because of deepcorneal scarring.
In cases of PBK, the IOL is not appropriately placedin some cases and may require removal, replacement,or repositioning. Intraocular lens exchange is recom-mended in cases with closed-loop IOLs, semiflexibleAC IOLs, iris-supported IOLs, or unstable IOLs be-cause these IOLs have been increasingly associatedwith endothelial compromise and poor macular func-tion postoperatively. In our series, all cases requiredIOL explantation because the IOLs were decenteredor malpositioned or were AC IOLs that were touchingor were very close to the endothelium, causing itsdecompensation.
Brunette et al.20 found that implanting a PC IOL atthe time of PKP provides better results thanimplanting an AC IOL; graft survival is longer, theIOP is lower, and the postoperative visual outcomesare better, even when the posterior capsule is dam-aged. Because all cases in our series had compromisedcapsule support, intrascleral haptic fixation of a PCIOL assisted with fibrin glue was a viable option.
ive Postoperative
IOP(mm Hg)
CDVA(LogMAR)
CCT(mm)
IOP(mm Hg)
ExplantedIOL
18 0.60 585 14 None16 0.48 562 12 None19 0.30 573 16 AC IOL18 0.30 612 16 None20 0.18 598 18 None14 0.60 605 14 PC IOL17 0.60 589 16 None16 0.48 564 18 PC IOL14 0.18 578 12 None16 0.30 546 12 PC IOL12 0.48 560 14 PC IOL
CCTZ central corneal thickness; CDVAZ corrected distance visual acuity;ular lens; IOP Z intraocular pressure; PBK Z pseudophakic bullous kerat-lasty; Pt Z patient
- VOL 38, JULY 2012

Figure 5. Clear cornea with intrasclerally fixated IOL 6 months afterDSAEK.
Figure 6. Clear graft with intrasclerally fixated IOL 6 months afterPKP.
1244 INTRASCLERAL GLUED IOL WITH CORNEAL PROCEDURES
Furthermore, in casesof aphakia, there is a risk forpos-teriormigration of injected air and dislocation of the len-ticule into the vitreous cavity.21 Placement of an IOLbefore the donor lenticule will not only improve the airtamponade but also reduce the risk for donor lenticuledislocation. Scleral fixation of a PC IOL combined withDSAEK has been successfully performed.22 The safetyand long-term efficacy of a transsclerally sutured PCIOL are less than satisfactory.7,8,23 In addition to prob-lems related to accurate suturing at the ciliary sulcus,there are issues with IOL–iris contact, pigment disper-sion, high aqueous flare, and vitreous incarceration.
Sutureless positioning of standard 3-piece PC IOLsby fixating the haptics in a limbus-parallel scleraltunnel has been reported in eyes without capsulesupport.24 Gabor and Pavlidis24 used a technique inwhich a sclerotomy is made in full-thickness scleraand the haptics are externalized and then introducedinto a scleral tunnel created with a needle. In ourstudy, we created a partial-thickness scleral flap andthe sclerotomy was made in the scleral bed. This scle-rotomy was covered by replacing the scleral flap backand sticking it with fibrin glue. Thus, there was no riskfor the creation of a communication track from outsideto inside the eye, theoretically reducing the risk for in-fectious organisms gaining access into the eye. Use offibrin glue completely blocks the sclerotomy, reducingthe risk for hypotony and infection. However, use offibrin glue increases the cost of the procedure.
Intrascleral glue fixation of a PC IOL combined withDSAEK has potential benefits over use of an AC IOLbecause it does not reduce the anterior chamber vol-ume, does not require intact iris tissue, and unlikesuture-fixated IOLs, does not carry the risk for knot
J CATARACT REFRACT SURG
slippage or pseudophakodonesis.25 No patient in ourseries had a significant complication, and all main-tained a stable CDVA of approximately 20/40.
In PKP, intrascleral fixation of IOL with fibrin gluecan also be a safe and effective alternative. Thistechnique reduces the surgical time25,26 and the timerequired for IOL fixation in an open globe after hosttrephination. The only additional time required is forexternalizing and tucking the haptic; this reduces therisk for expulsive hemorrhage or choroidal effusion.No intraoperative complication occurred in eyeshaving PKP with IOL fixation.
Another aim of our study was to determine whetherintrascleral fixation of an IOL by this technique isstrong enough to sustain the manipulations requiredduring DSAEK and PKP. Because there were no casesof IOL decentration during the procedures, we believethe technique provides strong fixation and an ade-quately stable IOL.
A limitation of this study is its short follow-upbecause with transscleral fixation of IOLs, there isa risk for complications in the late postoperativeperiod resulting from disappearance of fibrin glue.There is also the possibility of inadequate scleral-flaphealing.
In summary, fibrin glue-assisted intrascleral fixa-tion of a PC IOL combined with DSAEK or PKPwas a safe and effective method to manage pseudo-phakic corneal edema with aphakia or a malposi-tioned IOL. Although our initial results with thistechnique are good, larger comparative trials witha longer follow-up are needed to evaluate the long-term outcomes and to provide more conclusiveevidence.
- VOL 38, JULY 2012

1245INTRASCLERAL GLUED IOL WITH CORNEAL PROCEDURES
WHAT WAS KNOWN
� Intrascleral haptic fixation of a PC IOL with fibrin glue isa known technique for the visual rehabilitation of aphakiawith inadequate or absent capsule support.
� There are very few isolated case reports of the techniquecombining scleral fixation of IOL and DSAEK.
WHAT THIS PAPER ADDS
� Intrascleral haptic fixation of a PC IOL with fibrin glue of-fers adequate stability to the IOL so it can sustain manip-ulations required for DSAEK or PKP.
� In cases of aphakia, there is a risk for posterior migrationof injected air and dislocation of the lenticule into the vit-reous cavity. A posterior chamber IOL fixated intrasclerallyprevents posterior migration of air bubble, thereby en-abling good air tamponade, which in turn may providea better chance of donor lenticule adhesion.
REFERENCES1. F€orster W, Atzler U, Ratkay I, Busse H. Therapeutic use of the
193-nm excimer laser in corneal pathologies. Graefes Arch
Clin Exp Ophthalmol 1997; 235:296–305
2. Chen ES, Terry MA, Shamie N, Hoar KL, Friend DJ. Descemet-
stripping automated endothelial keratoplasty; six-month results
in a prospective study of 100 eyes. Cornea 2008; 27:514–520
3. Bal�azs E, Bal�azs K, M�odis L Jr, Berta A. Penetrating kerato-
plasty for pseudophakic bullous keratopathy. Acta Chir Hung
1997; 36:11–13
4. SoongHK,MeyerRF, Sugar A. Techniques of posterior chamber
lens implantationwithoutcapsular support duringpenetratingker-
atoplasty: a review. Refract Corneal Surg 1989; 5:249–255
5. Kocak-Altintas AG, Kocak-Midillioglu I, Dengisik F, Duman S. Im-
plantation of scleral-sutured posterior chamber intraocular lenses
during penetrating keratoplasty. J Refract Surg 2000; 16:456–458
6. Busin M, Brauweiler P, B€oker T, Spitznas M. Complications of
sulcus-supported intraocular lenses with iris sutures, implanted
during penetrating keratoplasty after intracapsular cataract ex-
traction. Ophthalmology 1990; 97:401–405; discussion by RF
Meyer, 405–406
7. Manabe S-I, Oh H, Amino K, Hata N, Yamakawa R. Ultrasound
biomicroscopic analysis of posterior chamber intraocular lenses
with transscleral sulcus suture. Ophthalmology 2000;
107:2172–2178
8. Buckley EG. Safety of transscleral-sutured intraocular lenses in
children. J AAPOS 2008; 12:431–439
9. Asadi R, Kheirkhah A. Long-term results of scleral fixation of
posterior chamber intraocular lenses in children. Ophthalmology
2008; 115:67–72
10. Vote BJ, Tranos P, Bunce C, Charteris DG, Da Cruz L. Long
term outcome of combined pars plana vitrectomy and scleral fix-
ated sutured posterior chamber intraocular lens implantation.
Am J Ophthalmol 2006; 141:308–312
11. G€uell JL, Barrera A, Manero F. A review of suturing techniques
for posterior chamber lenses. Curr Opin Ophthalmol 2004;
15:44–50
J CATARACT REFRACT SURG
12. Hannush SB. Sutured posterior chamber intraocular lenses:
indications and procedure. Curr Opin Ophthalmol 2000;
11:233–240
13. Agarwal A, Kumar DA, Jacob S, Baid C, Agarwal A,
Srinivasan S. Fibrin glue-assisted sutureless posterior
chamber intraocular lens implantation in eyes with deficient
posterior capsules. J Cataract Refract Surg 2008;
34:1433–1438
14. Patel NP, Kim T, Rapuano CJ, Cohen EJ, Laibson PR. Indica-
tions for and outcomes of repeat penetrating keratoplasty,
1989–1995. Ophthalmology 2000; 107:719–724
15. Flowers CW, Chang KY, McLeod SD, Irvine JA, McDonnell PJ,
Rao N, Smith RE. Changing indications for penetrating kerato-
plasty, 1989–1993. Cornea 1995; 14:583–588
16. Haamann P, Jensen OM, Schmidt P. Changing indications for
penetrating keratoplasty. Acta Ophthalmol (Copenh) 1994;
72:443–446
17. Mamalis N, Anderson CW, Kreisler KR, Lundergan MK,
Olson RJ. Changing trends in the indications for penetrating ker-
atoplasty. Arch Ophthalmol 1992; 110:1409–1411
18. Price MO, Price FW. Descemet’s stripping endothelial kerato-
plasty. Opin Ophthalmol 2007; 18:290–294
19. Price FW Jr. Corneal transplantation as a refractive surgi-
cal procedure [guest editorial]. J Refract Surg 2005;
21:216–217
20. Brunette I, Stulting RD, Rinne JR, Waring GO III, Gemmil M.
Penetrating keratoplasty with anterior or posterior chamber
intraocular lens implantation. Arch Ophthalmol 1994;
112:1311–1319
21. Suh LH, Kymionis GD, Culbertson WW, O’Brien TP, Yoo SH.
Descemet stripping with endothelial keratoplasty in aphakic
eyes. Arch Ophthalmol 2008; 126:268–270. Available at:
http://archopht.ama-assn.org/cgi/reprint/126/2/268. Accessed
April 1, 2012
22. Wylegala E, Tarnawska D. Management of pseudophakic bul-
lous keratopathy by combined Descemet-stripping endothelial
keratoplasty and intraocular lens exchange. J Cataract Refract
Surg 2008; 34:1708–1714
23. Price MO, Price FW Jr, Werner L, Berlie C, Mamalis N. Late dis-
location of scleral-sutured posterior chamber intraocular lenses.
J Cataract Refract Surg 2005; 31:1321–1326
24. Gabor SGB, Pavlidis MM. Sutureless intrascleral posterior
chamber intraocular lens fixation. J Cataract Refract Surg
2007; 33:1851–1854
25. Prakash G, Agarwal A, Jacob S, Kumar DA, Chaudhary P,
Agarwal A. Femtosecond-assisted Descemet stripping auto-
mated endothelial keratoplasty with fibrin glue-assisted suture-
less posterior chamber lens implantation. Cornea 2010;
29:1315–1319
26. Prakash G, Jacob S, Kumar DA, Narsimhan S, Agarwal A,
Agarwal A. Femtosecond-assisted keratoplasty with fibrin
glue-assisted sutureless posterior chamber lens implantation:
new triple procedure. J Cataract Refract Surg 2009; 35:
973–979
- V
OL 38, JULY 2012First author:Rajesh Sinha, MD, FRCS
Rajendra Prasad Centre for OphthalmicSciences, All India Institute of MedicalSciences, New Delhi, India