Embed Size (px)
Citation preview

The Journal of Arthroplasty Vol. 26 No. 2 2011
Case Report
From thCalifornia.
SubmitNo benReprint
Institute, 1© 20110883-5doi:10.1
Intrapelvic Displacement of a Trial Femoral HeadDuring Total Hip Arthroplasty and a Method to
Retrieve It
Kunal Kalra, MD, Michael D. Ries, MD, and Kevin J. Bozic, MD, MBA
Abstract: We describe a technique to retrieve a dislodged femoral trial during total hip arthroplasty.During a revision total hip arthroplasty performed through a direct lateral approach, the femoral trialhead was dislodged deep into the pelvis, superior and anterior to the hip joint and behind theanterior pelvic rim. This was retrieved via a posterior approach through the same incision bymanipulating the trial head through the pelvis from the anterior to posterior direction. To ourknowledge, this technique has not been described previously. Keywords: intrapelvic displacement,trial femoral head, total hip arthroplasty, retrieval.© 2011 Elsevier Inc. All rights reserved.
Dislodgement of a femoral head trial and its subsequentmigration deep into pelvis during total hip arthroplastyhave been previously described [1-3]. This is a verychallenging situation where the surgeon has to decide toeither leave the trial inside the pelvis or make anothersurgical approach to retrieve it. Often, this necessitatesgoing through a retroperitoneal approach and requiresthe expertise of an abdominal surgeon, thus carrying withit an additional surgical risk.We describe a case scenario in a patient in whom the
femoral trial head was dislodged deep into the pelvisduring a revision total hip arthroplasty via a lateralapproach. The trial head was dislodged superior andanterior to the hip joint and behind the anterior pelvicrim. This was ultimately retrieved through a posteriorapproach through the same incision by manipulating thetrial head through the pelvis from the anterior toposterior direction. To our knowledge, this techniquehas not been described previously.
Case ReportRevision total hip arthroplasty was performed in a
58-year-old woman with symptoms of recurrent disloca-
e Division of Arthroplasty, University of California, San Francisco
ted July 30, 2009; accepted December 5, 2009.efits or funds were received in support of this study.requests: Kevin Bozic, MD, Mission Bay Orthopaedic500 Owens St, San Francisco, CA 94158.Elsevier Inc. All rights reserved.
403/2602-0032$36.00/0016/j.arth.2009.12.005
33
,
8.e
tions to correct acetabular component malposition andincrease the femoral head size. The patient was placedin the lateral position, and a direct lateral approachthrough the previous incision was used. The anteriorthird of the gluteus medius and minimus muscles wasreflected from the greater trochanter. The implant wasexposed, and the hip dislocated anteriorly.The femoral component was well fixed and hence
retained. The modular femoral head was removed fromthe femoral component. The acetabular component wasremoved. A 54-mm porous-coated revision acetabularcomponent (Zimmer, Warsaw, Ind) was implanted. Aneutral-offset trial liner with 36-mm inner diameter wasinserted. A 36 + 8.5–mm standard-offset trial femoralhead was placed on the femoral component, and the hipwas reduced. During this maneuver, the trial head cameoff and migrated deep into the wound.Immediately, the hip was brought into the dislocated
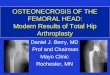
position. The head could not be visualized but waspalpable in the retroperitoneal space (Fig. 1). Differentinstruments including longKocher clamps, basket clamps,long curved clamps, and Cobb elevators were used inan effort to retrieve the head. All attempts to retrieve thehead failed and pushed it further into the cavity.Eventually, the head was found posterior to the
superior ramus. Although the head was palpated, itcould not be extracted. To restore soft tissue stability so asto facilitate retrieval of the trial femoral head, thefinal implants were assembled; and the hip was reduced.A 36-mm head with 8.5-mm offset was implanted.The intrapelvic space medial to the acetabulum could be
palpated through the anterior approach. We decided to
21
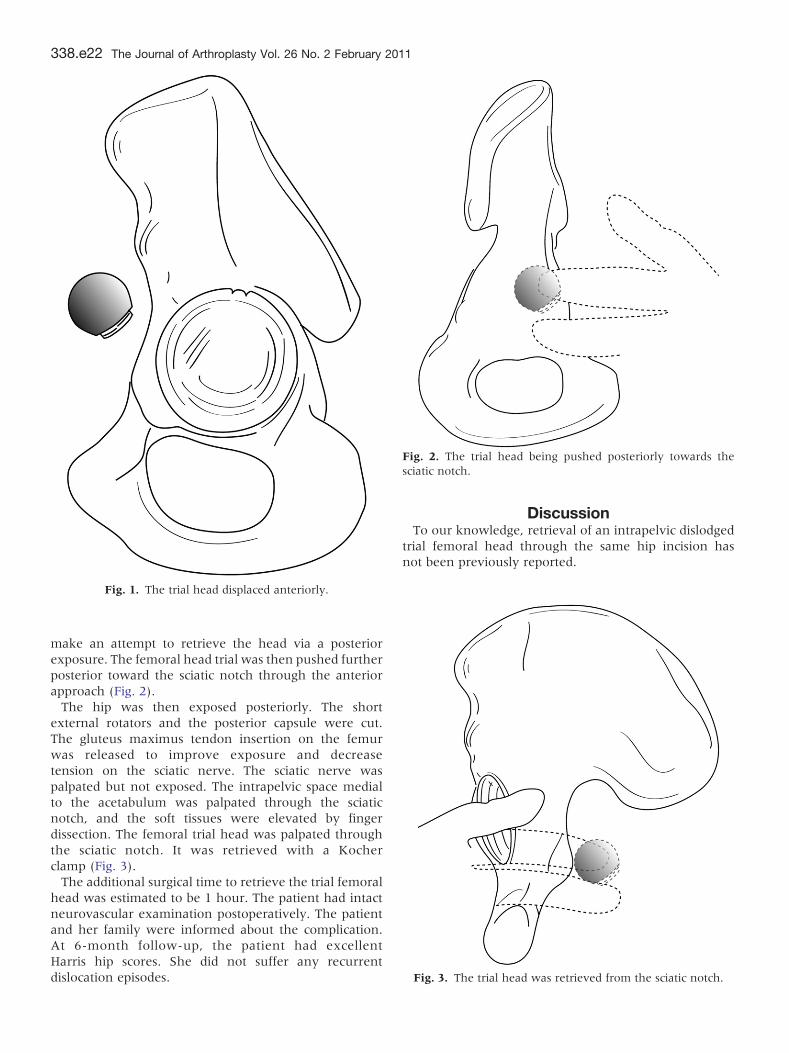
Fig. 1. The trial head displaced anteriorly.
Fig. 3. The trial head was retrieved from the sciatic notch.
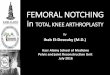
Fig. 2. The trial head being pushed posteriorly towards thesciatic notch.
338.e22 The Journal of Arthroplasty Vol. 26 No. 2 February 2011
make an attempt to retrieve the head via a posteriorexposure. The femoral head trial was then pushed furtherposterior toward the sciatic notch through the anteriorapproach (Fig. 2).The hip was then exposed posteriorly. The short
external rotators and the posterior capsule were cut.The gluteus maximus tendon insertion on the femurwas released to improve exposure and decreasetension on the sciatic nerve. The sciatic nerve waspalpated but not exposed. The intrapelvic space medialto the acetabulum was palpated through the sciaticnotch, and the soft tissues were elevated by fingerdissection. The femoral trial head was palpated throughthe sciatic notch. It was retrieved with a Kocherclamp (Fig. 3).The additional surgical time to retrieve the trial femoral
head was estimated to be 1 hour. The patient had intactneurovascular examination postoperatively. The patientand her family were informed about the complication.At 6-month follow-up, the patient had excellentHarris hip scores. She did not suffer any recurrentdislocation episodes.
DiscussionTo our knowledge, retrieval of an intrapelvic dislodged
trial femoral head through the same hip incision hasnot been previously reported.

Intrapelvic Displacement of a Trial Femoral Head During THA � Kalra et al 338.e23
By pushing the head with the finger, the implant couldbe brought down to a more accessible position. No specialinstruments were required. The intrapelvic medial wall ofthe acetabulum has several important structures in itsvicinity. Wasielewski et al [4] described the proximity ofthese nerves and vessels for optimal placement of screws.However, Harris et al [5] have described finger dissectionaround these structures; and no injury to these structureshas been reported in their series. The obturator internusmuscle and its overlying fascia cover the lateral wall of thepelvis, adjacent to the acetabulum [6]. This fasciacontinues over to the midline structures in the pelvisand perineum. Thus, the trial head is unlikely to migratedown into the lower pelvis and perineum. Furthermore,blunt dissection with a finger is unlikely to damage theneurovascular structures.In this case, going through the posterior approach
permitted retrieval of the femoral head trial while avoidingan additional incision and retroperitoneal exposure.
References1. Batouk O, Gilbart M, Jain R. Intraoperative dislocation of the
trial femoral head into the pelvis during total hip arthro-plasty: a case report. J Bone Joint Surg Am 2001;83:1549.
2. Callaghan JJ, McAndrew C, Boese CK, et al. Intrapelvicmigration of the trial femoral head during total hiparthroplasty: is retrieval necessary? A report of 4 cases.IOWA Orthop J 2006;26:60.
3. Ziv YB, Backstein D, Safir O, et al. Intraoperative dislocationof the trial femoral head into the pelvis during total hiparthroplasty. J Can Surg 2008;51.
4. Wasielewski RC, Cooperstein LA, Kruger MP, et al.Acetabular anatomy and the transacetabular fixation ofscrews in total hip arthroplasty. J Bone Joint Surg Am 1990;72A:501.
5. Harris WH, Crothers O, Oh I. Acetabular deficiency in adultstotal hip replacement and femoral-head bone-grafting forsevere. J Bone Joint Surg Am 1977;59:752.
6. Moore KL, Dalley AF. Clinically oriented anatomy. 5th ed.Baltimore: Lippincott Williams & Wilkins; 2005.