Embed Size (px)
Citation preview

Intraoperative Events Common to Videoscopic Preperitoneal Mesh Inguinal Herniorrhaphy
C. Daniel Smith, MD, Atlanta, Georgia, Greg Tiao, MD, Thomas Beebe, Cincinnati, Ohio
BACKGROUND: Videoscopic preperitoneal mesh (VPM) inguinal herniorrhaphy avoids the entry into the abdominal cavity, which is necessary with other videoscopic techniques. Despite this ad- vantage, surgeons have been slow to adopt this technique. We reviewed our experience with VPM inguinal hemiorrhaphy, specifically investigating the technical aspects of this approach.
METHODS: Data were collected prospectively. Op- erative notes were reviewed retrospectively de- tailing intraoperative events not "typical" with the VPM technique.
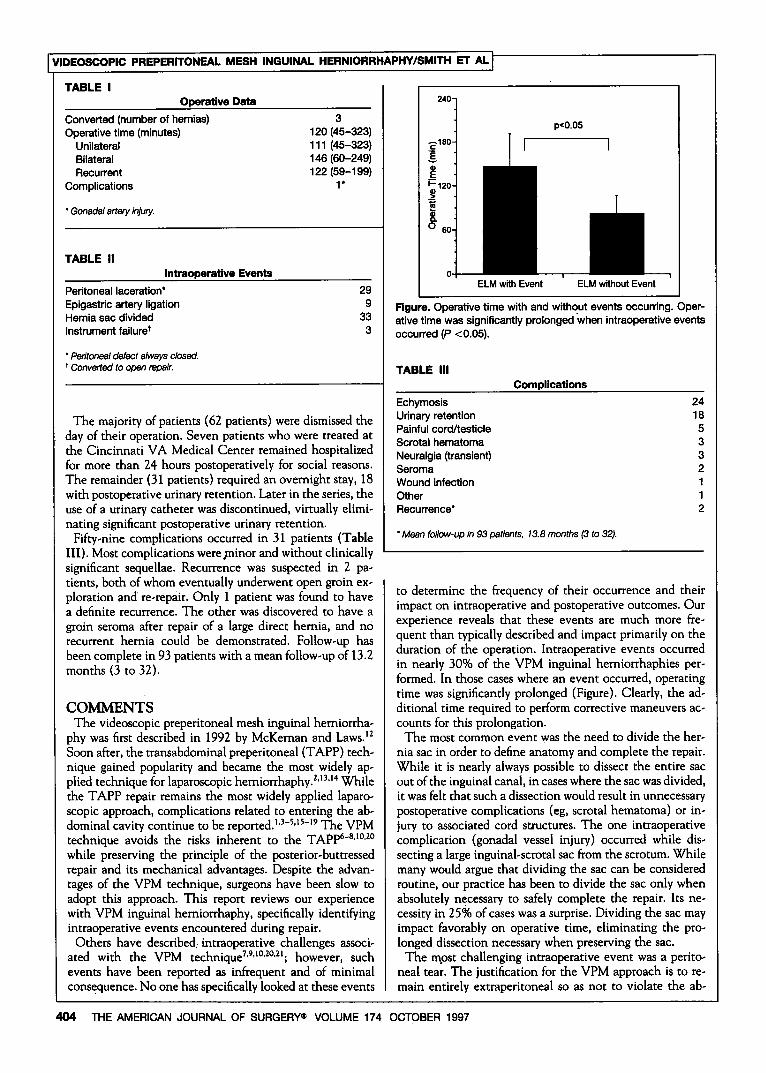
RESULTS: One hundred consecutive patients un- dergoing VPM repair of 127 hernias were studied. The repair was completed in all but 2 patients. Mean operating time was 120 minutes (60 to 146). In 36 repairs there were 59 intraoperative "events" requiring specific maneuvers to correct. Events identified were the need for transection of the hernia sac, creation and repair of a peritoneal tear, and need to divide the inferior epigastric vessels. No complications related to these events occurred. When events occurred, operative times were significantly longer (146 ___ 45 versus 83 ___ 23 minutes; P <0.05).
CONCLUSION: Intraoperative events are common with VPM herniorrhaphy. These events signifi- cantly prolong operating time. A surgeon's lack of familiarity with such events and how to deal with them may in part explain the reluc- tance to widely apply the VPM technique. Am J Surg. 1997;174:403-405. © 1997 by Excerpta Med- ica, Inc.
T he transabdominal preperitoneal (TAPP) inguinal herniorrhaphy is the most commonly performed technique of laparoscopic hernia repair. Because this
technique requires entry into the abdomen, significant com- plications related to violating the abdominal cavity have been reported. ~-6 The videoscopic preperitoneal mesh (VPM) technique of inguinal hernia repair avoids entry
From the Department of Surgery, (CDS), Emory University School of Medicine, Atlanta, Georgia, and the Department of Sur- gery, (GT, TB), University of Cincinnati, Cincinnati, Ohio.
Supported in part by a grant from Ethicon Endosurgery Inc., Cin- cinnati, Ohio.
Correspondence should be addressed to C. Daniel Smith, MD, Crawford Long Hospital of Emory University, 550 Peachtree Street, NE, Atlanta, Georgia 30365-2225.
Manuscript submitted March 3, 1997 and accepted in revised form June 10, 1997.
into the abdominal cavity and thereby eliminates the risks and complications inherent to the TAPP repair. The VPM technique has become the preferred "laparoscopic" ap- proach to inguinal hernia repair. 6-~° Despite its advantages, adoption of the VPM technique by surgeons performing other laparoscopic repairs has been slow. Our experience with the VPM hemiorrhaphy has been that it is accompa- nied by frequent intraoperative "events," which make it more challenging to perform than typically described. We have reviewed our experience with the first 100 patients undergoing VPM inguinal herniorrhaphy, specifically studying the technical aspects of this procedure and iden- tifying intraoperative deviations from what has been de- scribed as the typical procedure.
M E T H O D S Data on all patients undergoing VPM inguinal hernior-
rhaphy were collected prospectively. Additionally, charts were reviewed retrospectively to verify data. All operative procedures were performed in a University/Medical School based practice where general surgery residents participate in all operative procedures. Videoscopic preperitoneal mesh inguinal hemiorrhaphy was offered to all patients referred for inguinal herniorrhaphy except those with large inguinal- scrotal hernia, lower midline operative scar, t~ or suspected sliding hernia. Follow-up was by physician examination or phone call. The first 100 consecutive uses of the VPM tech- nique are reported. Results are shown as the mean +_ SEM. Comparisons were made using analysis of variance (ANOVA) with significant difference when P <0.05.
R E S U L T S Between February 1994 and April 1996, 100 consecutive
patients underwent videoscopic preperitoneal mesh repair of 127 hernias. Patients were predominately male (M:F 93:7) and of average age (mean age 45 years) and body size (mean weight 78 kg). There were 73 unilateral hernias and 27 bilateral hernias. Only 18 hernias were recurrent.
The VPM technique was completed in all but 2 patients. In these 2 patients, 3 videoscopic repairs were converted to open repairs because of instrument problems (Table I). There was one intraoperative complication (gonadal vessels avulsed during dissection of the hernia sac requiring ligation of the gonadal artery and subsequent testicular devascular- ization). Operative times ranged from 60 to 146 minutes (Table I). In 36 repairs, there were 59 intraoperative "events" that required performance of specific maneuvers to address or correct the event (Table II). An event was defined as any occurrence requiring a specific maneuver that would not be considered part of a typical VPM repair. In cases where events occurred, operative times were signifi- cantly longer than in those where no event occurred (146 -+ 45 minutes versus 83 + 23 minutes; P <0.05) (Figure).
© 1997 by Excerpta Medica, Inc. 0002-9610/97/$17.00 403 All rights reserved. PII S0002-9610(97)00127-X
VIDEOSCOPIC PREPERITONEAL MESH INGUINAL HERNIORRHAPHY/SMITH ET AL I
Operative Data TABLE I
Converted (number of hemias) 3 Operative time (minutes) 120 (45-323)
Unilateral 111 (45-323) Bilateral 146 (60-249) Recurrent 122 (59-199)
Complications 1"
Intraoperative Events
"Gonadal artery injury.
TABLE II
Peritoneal laceration* 29 Epigastric artery ligation 9 Hernia sac divided 33 Instrument failure t 3
"Peritoneal defect always closed. t Converted to open repair.
The majority of patients (62 patients) were dismissed the day of their operation. Seven patients who were treated at the Cincinnati VA Medical Center remained hospitalized for more than 24 hours postoperatively for social reasons. The remainder (31 patients) required an overnight stay, 18 with postoperative urinary retention. Later in the series, the use of a urinary catheter was discontinued, virtually elimi- nating significant postoperative urinary retention.
Fifty-nine complications occurred in 31 patients (Table III). Most complications were.minor and without clinically significant sequellae. Recurrence was suspected in 2 pa- tients, both of whom eventually underwent open groin ex- ploration and re-repair. Only 1 patient was found to have a definite recurrence. The other was discovered to have a groin seroma after repair of a large direct hernia, and no recurrent hernia could be demonstrated. Follow-up has been complete in 93 patients with a mean follow-up of 13.2 months (3 to 32).
C O M M E N T S The videoscopic preperitoneal mesh inguinal herniortha-
phy was first described in 1992 by McKernan and Laws. 12 Soon after, the transabdominal preperitoneal (TAPP) tech- nique gained popularity and became the most widely ap- plied technique for laparoscopic herniorrhaphy. 2a3'L4 While the TAPP repair remains the most widely applied laparo- scopic approach, complications related to entering the ab- dominal cavity continue to be reported. ~'3-s'~5-19 The VPM technique avoids the risks inherent to the TAPP 6-sa°'2° while preserving the principle of the posterior-buttressed repair and its mechanical advantages. Despite the advan- tages of the VPM technique, surgeons have been slow to adopt this approach. This report reviews our experience with VPM inguinal hemiorrhaphy, specifically identifying intraoperative events encountered during repair.
Others have described, intraoperative challenges associ- ated with the VPM techniqueT'9'l°'z°'zl; however, such events have been reported as infrequent and of minimal consequence. No one has specifically looked at these events
k= >=
o
40
80
20
6O
¢
ol
p<0.05
[
e m l ELM with Event ELM without Event
Figure. Operative time with and without events occurring. Oper- ative time was significantly prolonged when intraoperative events occurred (P <0.05).
TABLE III Complications
Echymosis 24 Urinary retention 18 Painful cord/testicle 5 Scrotal hematoma 3 Neuralgia (transient) 3 Seroma 2 Wound infection 1 Other 1 Recurrence* 2
"Mean follow-up in 93 patients, 13.8 months (3 to 32).
to determine the frequency of their occurrence and their impact on intraoperative and postoperative outcomes. Our experience reveals that these events are much more fre- quent than typically described and impact primarily on the duration of the operation. Intraoperative events occurred in nearly 30% of the VPM inguinal herniorrhaphies per- formed. In those cases where an event occurred, operating time was significantly prolonged (Figure). Clearly, the ad- ditional time required to perform corrective maneuvers ac- counts for this prolongation.
The most common event Was the need to divide the her- nia sac in order to define anatomy and complete the repair. While it is nearly always possible to dissect the entire sac out of the inguinal canal, in cases where the sac was divided, it was felt that such a dissection would result in unnecessary postoperative complications (eg, scrotal hematoma) or in- jury to associated cord structures. The one intraoperative complication (gonadal vessel injury) occurred while dis- secting a large inguinal-scrotal sac from the scrotum. While many would argue that dividing the sac can be considered routine, our practice has been to divide the sac only when absolutely necessary to safely complete the repair. Its ne- cessity in 25% of cases was a surprise. Dividing the sac may impact favorably on operative time, eliminating the pro- longed dissection necessary when preserving the sac.
The most challenging intraoperative event was a perito- neal tear. The justification for the VPM approach is to re- main entirely extraperitoneal so as not to violate the ab-
404 THE AMERICAN JOURNAL OF SURGERY ® VOLUME 174 OCTOBER 1997
I VIDEOSCOPIC PREPERITONEAL MESH INGUINAL HERNIORRHAPHY/SMITH ET AL
dominal cavity. Such violation potentially negates this advantage and risks bowel injury and potential intraabdom- inal adhesion formation with bowel obstruction. ~'3-5'15-~9 When dissecting the peritoneum away from the ventral ab- dominal wall and cord structures to expose the myopecti- neal orifice posteriorly, tears in the peritoneum can occur. Typically, these are small and easily repaired by closing the defect with a ligature (eg, endoloop). Failure to recognize and close such a defect immediately may result in the ab- dominal cavity filling with gas, thereby reducing the pre- peritoneal operative field and making completion of the repair extremely difficult. Early recognition and repair of such a tear minimizes the inconvenience of intraperitoneal insufflation. When recognized late, it may be necessary to insert a veress needle into the abdominal cavity to decom- press the pneumoperitoneum and facilitate repair of the peri- toneal defect and completion of the herniorrhaphy. Com- pleting the herniorrhaphy and leaving a peritoneal tear un- repaired may allow the bowel to come in contact with the mesh leading to subsequent problems (eg, adhesive bowel obstruction). When repairing peritoneal defects, care must be taken that intraabdominal content is not incorporated into the ligature closing the peritoneal tear. Overall, dealing with these tears requires considerable patience and a thoughtful approach to correcting the problem.
Finally, during the initial balloon facilitated dissection of the preperitoneal space, the epigastric vessels may become dissected away from the ventral abdominal wall and hang in the operative field. The resulting encroachment of the vessels on the operative field makes completing the repair extremely difficult. In 9 cases, the epigastric vessels required ligation and transection to clear the operative field and complete the repair.
Non~ of these events appeared to impact on outcome, including hospitalization or complications. The two pre- sumed (one confirmed) recurrences occurred early in the series and were due to technical errors in mesh placement (mesh too small resulting in inadequate lateral coverage): It had been our routine in all patients to use an indwelling urinary catheter during the operation, with removal before transport to the recovery room. Our high rate of urinary retention and resulting overnight hospitalization prompted a reevaluation of this routine. We now minimize intrave- nous fluids and no longer use a urinary catheter. Urinary retention has been virtually eliminated by these changes. The remaining complications have been transient and are consistent with reported complications with both open and laparoscopic repairs, l'6'zl • Overall, our experience reveals that intraoperative events are common during VPM inguinal herniorrhaphy. Such events can jeopardize the successful completion of the planned laparoscopic repair. Even when dealt with, such events prolong operative time and can introduce significant frustration for the surgeon and operating team. While com- mon, these events can easily be dealt with intraoperatively. Anticipation of such events and the ability to deal with them is critical to completing these procedures without compromising outcome, while at the same time minimizing
the anxiety and frustrations felt before, during, and after the operative procedure.
R E F E R E N C E S 1. Phillips EH, Arregui M, Carroll BJ, et al. Incidence of compli- cations following laparoscopic hemioplasty. Surg Endosc. 1995; 9:16-21. 2. Fitzgibbons RJ, Jr., Camps J, Comet DA, et al. Laparoscopic in- guinal hemiorrhaphy. Results of a multicenter trial. Ann Surg. 1995;221:3-13. 3. Petersen TI, Qvist N, Wara P. Intestinal obstruction--a proce- dure-related complication of laparoscopic inguinal hernia repair. Surg Laparosc Endosc. 1995q5:214-216. 4. Attwood SE, Caldwell MT, Marks P, et al. Adhesions after lap- aroscopic inguinal hernia repair. A comparison of extra versus intra peritoneal placement of a polypropylene mesh in an animal model. Surg Endosc. 1994;8:777-780. 5. Sioris T, Perhoniemi V, Schroder T. Peritoneal herniation and intestinal obstruction: a complication of laparoscopic inguinal her- niorrhapy. Eur J Surg. 1995;161:533-534. 6. Ramshaw BJ, Tucker JG, Conner T, et al. A comparison of the approaches to laparoscopic hemiorrhaphy. Surg Endosc. 1996; 10:29-32. 7. Ramshaw BJ, Tucker JG, Duncan TD, et al. Technical consid- erations of the different approaches to laparoscopic hemiorrhaphy: an analysis of 500 cases. Am Surg. 1996;62:69-72. 8. Ramshaw BJ, Tucker JG, Mason EM, et al. A comparison of tmnsabdominal preperitoneal (TAPP) and total extraperitoneal ap- proach (TEPA) laparoscopic hemiorrhaphies. Am Surg. 1995; 61:279-283. 9. Ferzli G, Kiel T. Evolving techniques in endoscopic extraperi- toneal hemiorrhaphy. Surg Endosc. 1995;9:928-930. 10. Felix EL, Michas CA, Gonzalez MH, Jr. Laparoscopic hemio- plasty. TAPP vs TEP. Surg Endosc. 1995;9:984-989. 11. Ramshaw BJ, Tucker J, Duncan T, et al. The effect of previous lower abdominal surgery on performing the total extraperitoneal approach to laparoscopic hemiorrhaphy. Am Surg. 1996;62:292- 294. 12. McKeman BJ, Laws HL. Laparoscopic preperitoneal prosthetic repair of inguinal hernias. Surg Rounds. 1992;15:579-610. 13. Corbitt JD, Jr. Transabdominal preperitoneal hemiorrhaphy. Surg Laparosc Endosc. 1993;3:328-332. 14. Arregui ME, Navarrete J, Davis CJ, et al. Laparoscopic inguinal hemiorrhaphy. Techniques and controversies. Surg Clin North Am. 1993;73:513-527. 15. Durstein-Decker C, Brick WG, Gadacz TR, et al. Comparison of adhesion formation in transperitoneal laparoscopic hemiorrha- phy techniques. Am Surg. 1994;60:157-159. 16. Eller R, Twaddell C, Poulos E, et al. Abdominal adhesions in laparoscopic hernia repair. An experimental study. Surg Enclose. 1994;8:181-184. 17. Milencoff S, DeGara CJ, Gagic N. Intestinal obstruction fol- lowing laparoscopic inguinal hernia repair. Br] Surg. 1994;81:471- 472. 18. Milkins R, Wedgwood K. Intestinal obstruction following lap- aroscopic inguinal hernia repair. BrJ Surg. 1994;81:471. 19. Tsang S, Normand R, Karlin R. Small bowel obstruction: a morbid complication after laparoscopic hemiorrhaphy. Am Surg. 1994;60:332-334. 20. Voeller GR, Mangiante EC Jr. Totally preperitoneal laparo- scopic inguinal hemiorrhaphy using balloon distention. ScandJ Gas- troenterol Suppl. 1995;208:67-73. 21. Liem MS, van Steensel SCJ, Boelhouwer RU, et al. The learn- ing curve for totally extraperitoneal laparoscopic inguinal hernia repair. Am] Surg. 1996;171:281-285.
THE AMERICAN JOURNAL OF SURGERY ® VOLUME 174 OCTOBER 1997 405












![Seroma following transabdominal preperitoneal patch plasty ......after laparoendoscopic inguinal hernia repair [13]. Like-wise, while in one observational study comparison of mesh](https://img.pdfslide.us/doc/110x75/60856af68b068522726ea0ff/seroma-following-transabdominal-preperitoneal-patch-plasty-after-laparoendoscopic.jpg)