Embed Size (px)
Citation preview

4. Shentu X, Tang X, Yao K. Spherical aberration, visualperformance and pseudoaccommodation of eyesimplanted with different aspheric intraocular lens. ClinExperiment Ophthalmol 2008; 36: 620–4.
5. Yu AY, Wang QM, Sun J et al. Spherical aberration afterimplantation of an aspheric versus a spherical intraocu-lar lens in high myopia. Clin Experiment Ophthalmol 2009;37: 558–65.
Intraocular pressure elevation inisolated extraocular muscleinfiltration by leukaemia
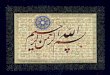
We report a 34-year-old man who presented with a1-month history of gradually increasing proptosis, ocularpain, blurring of vision, diplopia and redness in the righteye. He was diagnosed with acute myeloid leukaemia6 months ago and received two cycle of consolidationtherapy after the first remission induction chemotherapy.Ocular symptoms appeared approximately 1 month afterthe second consolidation course. Medical history revealedhyperthyroidism treated by iodine-131 radioisotopetherapy 4 years ago. External examination showed a rightproptosis (Hertel readings of 21 mm OD and 13 mm OS)(Fig. 1a,b). There were not orbital bruits or pulsation. In
the right eye, there was no abduction movement, and allother ductions were minimally limited in ocular motilityexamination (Fig. 1c).
Slit-lamp examination showed apparent dilation oflateral episcleral veins. On gonioscopy of the right eye,angles were open with blood in the Schlemm canal infe-riorly and temporally (Fig. 1d). Dilated funduscopyrevealed mild vascular tortuosity and disc oedema in theright eye. Goldmann applanation tonometry measure-ments were 42 mmHg OD and 14 mmHg OS. Visual acu-ities were 6/9 OD and 6/6 OS. Orbital magnetic resonanceimaging demonstrated diffuse enlargement of right lateralrectus muscle, and the adjacent orbital tissues were notinvolved (Fig. 1e). The magnetic resonance imaging ofbrain was normal, and there was no evidence of cavernoussinus involvement.
Based on these findings, isolated leukemic infiltrationof extraocular muscle and thyroid ophthalmopathyappeared to be most probable diagnoses. We decided toperform right lateral rectus muscle biopsy for differentialdiagnosis. An incisional biopsy with lateral limbal con-junctival approach was performed, and a specimen wasobtained from the margin of the right lateral rectus muscletendon and Tenon’s capsule. Histopathological evaluationof the specimen revealed diffuse infiltration of the rectustendon and Tenon’s capsule with mononuclear cells withhigh nucleocytoplasmic ratio (Fig. 1f). These cellsexpressed CD117 diffusely and myeloperoxidase focally inimmunohistochemical studies. These findings were sug-gestive of myelomonoblastic infiltration of isolated
Figure 1. (a,b) Patient’s facialphotograph on admission. Externalexamination showed a right prop-tosis (Hertel readings of 21 mm onthe right 13 mm on the left eye). (c)In ocular motility examination,abduction of the right eye wastotally limited. (d) Gonioscopyof the right eye revealed blood inthe Schlemm canal inferiorlyand temporally. (e) Fat-suppressedT2-weighted axial orbital magneticresonance imaging demonstrateda marked enlargement of the rightlateral rectus muscle. The rightlateral rectus muscle was slightlyhyperintense compared with unaf-fected muscles, and the adjacentorbital tissues were not involved.(f) Histopathological evaluation ofthe specimen obtained by inci-sional biopsy revealed diffuse infil-tration of the right rectus tendonand Tenon’s capsule by mono-nuclear blastic cells with highnucleocytoplasmic ratio (HE, origi-nal magnification ¥200).
Letters to the Editor 283
© 2011 The AuthorsClinical and Experimental Ophthalmology © 2011 Royal Australian and New Zealand College of Ophthalmologists

extraocular muscle. The high intraocular pressure (IOP)was reduced to 23 mmHg with topical timolol-dorzolamide fixed combination, brimonidine and oralacetozolamide.
The leukaemic infiltration of isolated lateral rectusmuscle was treated with external beam radiotherapy aloneover 10 days. Within 4 days a marked decrease in proptosisand episcleral venous dilation was noted, and IOP wasreduced to 10 mmHg. Thus, anti-glaucomatous therapywas stopped. On day 10 after the completion of radio-therapy, proptosis, diplopia and dilation of episcleral veinsresolved completely and ocular motility returned to normal(Fig. 2a–c). The blood in the Schlemm canal was no longervisualized on gonioscopy (Fig. 2d). On orbital magneticresonance imaging images, the enlargement of right lateralrectus muscle was evidently reduced (Fig. 2e). In the righteye, IOP was 12 mmHg without treatment and visualacuity was 6/6.
Acute myeloid leukaemia can involve the extramedul-lary tissues including skin, mucosa, central nervoussystem, eye and orbita.1 Leukaemic orbital infiltrationmay present most commonly with proptosis, eyelidoedema, blepharoptosis, visual impairment, ocular motil-ity disturbances, chemosis and infrequently with eleva-tion in IOP.2 Although there are many reported casesof secondary glaucoma or IOP elevation by intraocularleukaemic infiltration, the cases with orbital infiltrationare few in the literature. In one of these publications,Tumuluri et al.3 reported a case of leukaemia present-ing with proptosis and bilateral glaucoma. In this case
report, a patient of acute myeloid leukaemia developedbilateral orbital leukaemic infiltration, ocular compres-sion and aqueous misdirection resulting in angle-closureglaucoma.
In our patient, we found blood in the Schlemm canaland dilation of episcleral veins, which were suggestive ofaffected vascular drainage pathway and high episcleralvenous pressure. The episcleral venous system mainlydrains into the superior ophthalmic vein (SOV), whicheventually empties into the cavernous sinus.4 SOV followsa lateral trajectory at the midorbit behind the globe,between superior and lateral rectus muscles. At this loca-tion, the diameter of the SOV may reach 5–6 mm, servingas blood reservoir and altering orbital and ocularhaemodynamics.4 Then, it leaves the orbit through theupper part of superior orbital fissure, above the lateralrectus muscle, to join the cavernous sinus.5 We assume thatthe markedly enlarged lateral rectus muscle compressedthe SOV at retrobulbar locations described in the preced-ing text, thereby caused IOP elevation in our patient. Thepatient’s dramatic response to radiotherapy also supportsthis explanation.
In conclusion, we present clinicopathologically a well-documented case of isolated extraocular muscle infiltrationby leukaemia. Although extremely rare, IOP elevationshould be taken into account if a patient with leukaemiahas orbital infiltration, especially lateral rectus muscleinvolvement. External beam irradiation is an effectivemanagement choice to lower persistent IOP elevation insuch cases.
Figure 2. Ten days after thecompletion of radiotherapy, rightproptosis resolved completely andocular motility returned to normal(a–c). The blood in the Schlemmcanal disappeared on gonioscopy(d). On fat-suppressed T2-weightedaxial orbital magnetic resonanceimaging, the enlargement of rightlateral rectus muscle was evidentlyreduced (e).
284 Letters to the Editor
© 2011 The AuthorsClinical and Experimental Ophthalmology © 2011 Royal Australian and New Zealand College of Ophthalmologists

Ali Aydin MD FEBO,1 Akin Çakir MD,1
Ozkan Sayan MD,2 Aptullah Haholu MD,3
Murat Velioglu MD4 and Dilaver Ersanli MD1
Departments of 1Ophthalmology, 2Haematology, 3Pathology,and 4Radiology, Haydarpasa Training Hospital, Gulhane
Military Medical Academy, Istanbul, TurkeyReceived 20 September 2010; accepted 25 September 2010.
REFERENCES
1. Reinhardt D, Creutzig U. Isolated myelosarcoma inchildren- update and review. Leuk Lyphoma 2002; 43:565–74.
2. Reddy SC, Jackson N, Menon BS. Ocular involvementin leukemia-a study of 288 cases. Ophthalmologica 2003;217: 441–5.
3. Tumuluri K, Woo T, Crowston J, Healey PR, Gottlieb D,Maloof AJ. Bilateral leukemic orbital infiltration pre-senting as proptosis and narrow-angle glaucoma.Ophthal Plast Reconstr Surg 2004; 20: 248–50.
4. Nassr MA, Morris CL, Netland PA, Karcioglu ZA.Intraocular pressure change in orbital diseases. SurvOphthalmol 2009; 54: 519–44.
5. Snell RS, Lemp MA, eds. Clinical Anatomy of the Eye, 2ndedn. Malden, MA: Blackwell Science, Inc., 1998; 286–9.
Letters to the Editor 285
© 2011 The AuthorsClinical and Experimental Ophthalmology © 2011 Royal Australian and New Zealand College of Ophthalmologists