Embed Size (px)
Citation preview

??Original Contribution
INTRACRANIAL METASTASES: BEHAVIORAL PATTERNS RELATED TO PRIMARY SITE AND RESULTS OF TREATMENT BY WHOLE BRAIN
IRRADIATION
JOHN WEST, M.D.* and MOSHE MAOR, M.D.
Department of Radiotherapy, The University of Texas System Cancer Center, M. D. .4nderson Hospital and Tumor Institute. Houston. Texas 77030
Three hundred and fifty cases of tumors that metastasized to the brain and treated by radiotherapy were reviewed. The majority of patients bad either lung (46% ) or breast (42% ) primaries. Eighty percent of the patients had other sites of metastatic involvement. Seventy-five percent of the patients improved after cranial irradiation. The median survival was less than 6 months, regardless of the primary disease or the dose employed. No subgroup could be identified that might benefit from a more aggressive treatment regimen. Radiation treatment in the range of 2,000 rad in one week or 3.000 rad in two weeks is recommended for palliation of metastatic cancer to the brain.
Brain metastases. Brain irradiation
INTRODUCTION The optimal treatment of brain metastases by irradiation has been the subject of numerous publications with different conclusions.‘~4.0-” Part of the difficulty arises because metastatic cancer to the brain is not one single entity but rather a spectrum of disease with differing natural histories relating to site and aggressiveness of the primary tumor. Also. the clinical course of brain metas- tases is greatly dependent on the general condition of the patient, results of treatment of the primary tumor. complications, intercurrent disease, and the presence or absence of other distant metastases. In this paper, we will examine the clinical behavior of intracranial metastases according to a number of parameters.
METHODS AND MATERIAL Between January 1957 and December 1975 350
patients were treated for brain metastases at M. D. Anderson Hospital and Tumor Institute. All patients received one course of whole brain irradiation through lateral parallel opposed portals with megavoltage thera- py. Most patients (83%:) were between the ages of 40 to 70 years. Females comprised 60% and males, 40%. Eighty-six percent of the entire group was Caucasian. Lung cancer was the most frequent primary site (162 patients, 46%). followed by breast cancer (147 patients,
42%~); other primaries such as cervix. kidney, bladder, colon, bone, soft tissue, and endocrine glands comprised the remaining 12% Malignant melanoma metastatic to the brain was excluded from this series becasue this entity has been analyzed in a separate study at this institution.13 Because of the preponderance of lung and breast primaries. these were analyzed separately in addi- tion to the entire group. Twenty-eight patients (8%) underwent surgical excision of the metastases prior to the irradiation; three had biopsy alone, and five had malig- nant cells in their cerebrospinal fluid.
Two thirds of the primary tumors were controlled according to clinical examination, laboratory, and x-rab studies at the time that irradiation for brain metastases was begun. Four fifths of the patients had other distant metastases when their brain metastases were irradiated. Sites of other metastases, in order of frequency were bone, lung or pleura. neck or supraclavicular nodes, and liver or other intra-abdominal metastases. About one half of the patients had been on some form of chemotherapy prior to development of intracranial metastases, and two thirds received chemotherapy subsequent to irradiation.
The majority of patients (90%‘) had neurologic deficits or clinical. signs and symptoms of their brain metastases at the time of irradiation. Diagnosis was made by brain scan alone or in combination with electroencephalogra-
Reprint request to: Moshe Maor. M.D.. Assistant Radiother- apist and Assistant Professor of Radiotherapy, Department of Radiotherapy, M. D. Anderson Hospital and Tumor Institute. Houston, Texas 77030 Acknowledgemenr-This investigation was supported in part by Grants CA06294 and CA05654 awarded by the National
Cancer Institute, Department of Health. Education. and Welfare.
Accepted for publication 27 April 1979. *Present Address: Fred Woods Radiotherapy Center. St.
Joseph Hospital, Tampa. Florida.

80
E 60
3 t a 40
1 ___
Radiation Oncology 0 Biology 0 Physics January 1980, Volume 6, No. I
??Lung Primaries A Breast Primaries
p=0.001
I 2 3 4 5 6 7 8 Years
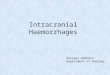
Fig. I. Interval between diagnosis of primary tumor and development of intracranial metastases.
phy in most cases (82%); angiography, pneumonencepha- lography. ventriculography, and plain radiographs made up the remainder. Computerized axial tomography (CAT) scans were not available at the time these patients were treated. The location of metastases within the brain was analyzed. The parietal lobe was the most common site, followed by multiple sites, frontal lobe, temporal lobe, occipital lobe, and cerebellum, in that order. Other locations with occassional metastases were midbrain. hypothalamus, and ventricles. In another 8% location was not specified.
Figure I shows the time from diagnosis of the primary tumor to onset of intracranial metastases for lung and breast primaries. The interval of all percentage levels is much shorter for lung primaries than for breast primar- ies; the median time from diagnosis of the primary to diagnosis of intracranial metastases is 6 months for lung cancer and 30 months for breast cancer.
When intracranial metastases from lung cancer were analyzed according to histology, it was found that squa- mous carcinoma comprised 36%, adenocarcinoma 32% oat cell carcinoma 25% and unknown or unclassified carcinomas 7%. For all patients with lung cancer who were seen at M. D. Anderson Hospital, squamous carci- noma comprised 49%. oat cell carcinoma comprised 18%. and all others comprised 33%. (H.T. Barkley, oral. personal communication, June 1978) Thus, it appears that oat cell carcinoma exhibits a greater propensity to metastasize to the brain than does squamous cell carcino- ma.
Treatment Technique: Treatment consisted of entire cranial cavity irradiation with parallel opposing lateral fields. The lower border of the field extended from the eye brow to the mastoid; there it slanted backward to include the posterior cranial fossa (Figare 2). One held was treated each day to the desired tumor dose taken at the midline. In order to analyze the results of different
Fig. 2. Fields used for whole brain irradiation.
treatment plans, it was necessary to group the patients according to easily recognizable dose and time values. Cross tabulation of the most frequent dose time treat- ment plans were identified for detailed evaluation (Tables I and 2).
Almost all patients (90%) were treated with Co? the rest were treated with 22-25 MeV x-rays or a combina- tion of energies. Ninety-seven percent of the patients received a continuous fractionated course, and the other 3% received a single fraction or interrupted courses. Ninety-nine percent were treated with the conventional five fractions per week. Thus, this series was comprised of standard and uniform treatment schemes. and very few unorthodox regimens. Ninety-five percent of the patients received oral steroids during the time of irradiation.
Table I. Dose and time factors in treatment of 147 patients with metastatic breast cancer to brain*
Time (weeks)
Dose (rad) <I 1 2 3 4 5
Less than 2000 3 2000 20 I 2500 2 I I 3000 I 70 ’ 3 500 14 ; 4000 4 21 I Over 4500 I 2
*For instance, 3.000 rad delivered in 2 weeks (the most prevelent treatment regimen in this series) was defined as 2,750-3,249 rad. in I l-l 7 days.

lntracramal metastases ??J. WEST and M. MAOR 13
Table 2. Dose and time factors in treatment of 162 patients Table 4. Symptomatic control of intracranial metastases at with metastatic lung cancer to the brain* last follow-up
Time (weeks)
Dose (rad I I 2 3 4 5
Less than 2000 I ‘000 15 2500 6 1 I 3000 I 121 9 1 3500 1 4000 I 4
*See footnote. Table I.
Symptoms controlled Symptoms persist Unknown
I\jumber Of
patients
5.’ 1x7 108
Relative frequency
(9)
15.1 53.4 30.9
RESULTS
Follow-up generally ranged from a maximum of 234 months to a minimum of 18 months. Since 94% of these patients had expired at the time of evaluation. even the minimum follow-up appears more than adequate for the evaluation of palliative benefits.
The results were analyzed according to the Karnofsky performance scale (Table 3) prior to and after whole brain irradiation and according to length of survival after irradiation. It was felt that the disabilities reflected in the Karnofsky scale were caused predominately by the intra- cranial metastases in this series, and, therefore, any shift from one group to a higher one would be a reflection of treatment effectiveness. Karnofsky ratings before and after irradiation were done by the same physician.
if there was any information regarding this parameter; if not, they are listed as unknown. At best, they are crude estimates because there was so little factual information. One hundred and four patients underwent repeat brain scans or radiographic studies subsequent to treatment. Of this group. 27% showed complete resolution of the abnor- malities.
Changes in Karnofsky scale effected by different radiation schedules appear in Table 5. For the purpose of palliation, a relatively short course of therapy. such as 2.000 rad/week was as effective as higher doses delivered over longer periods of time. This is a measure of maxi- mum functional improvement of the patient after treat- ment: however, it says nothing about the duration of response.
Table 3. Karnofsky performance scale
10% 20%
30%
40%
SO%
60%
70%
80% 90%
100%
Moribund Very sick, hospitalization necessary, active
supportive treatment necessary. Severely disabled. hospitalization indicated
but death not imminent. Disabled. requires special care and
assistance. Requires considerable assistance and
frequent medical care. Requires occasional assistance, unable to
care for most needs. Cares for self, unable IO carry out normal
activity or active work. hormal activity with effort. Normal activity with minor signs and
symptoms of disease. Normal. no complaints.
Unlike cancer of the breast, which is comprised of adenocarcinoma and its subtypes. cancer of the lung includes several histologies that may exhibit different behavior or response when metastatic to the brain. There- fore we analyzed metastatic lung cancer according to the classification of squamous cell carcinoma, adenocarcino- ma. and oat cell carcinoma. Large cell anaplastic carci- noma was grouped with adenocarcinoma. and a small group of unclassifiable carcinoma was analyzed separate- ly. When Karnofsky scores before and after treatment for the above histologies were evaluated. all histoiogies were identified as being improved by, about one Karnofsky rating; the majority entered at 70’3 and emerged at 80%. Therefore, except for the unclassifiable group. which contained too few patients for evaluation, the response among patients with various histologies was about the same. However, the median survival, of adenocarcinoma of the lung ( 16 mo) is somewhat higher than that of oat
Table 5. Change in Karnofsky scale by dose-time factors
Based on the information provided in the hospital charts. it is difficult to state whether irradiation has achieved control of intracranial metastases. The main difficulty is that many patients expire at home or in an outside hospital. and information concerning the cause of demise and the status of intracranial disease is sketchy. However. we submit the following as estimates of symp- tomatic control of intracranial metastases (Table 4). These values were for the entire scheme used, and were assessed at the last follow-up entry in the hospital chart,
% Patients Change in Karnofsky 2000 rad 3000 rad 3500 rad 4000 rad
scale 1 week 2 weeks 2 weeks 4 weeks (No. of pts.) (36) (219) (14) (26)
- 1 or worse 0 4.1 0 0 0 36.1 31.5 28.5 Il.4
+I 36.1 43.9 64.2 34.6 +’ 16.7 I I.9 7.1 15.3 +3 5.6 2.9 0 26.8 +4 5.6 2.3 0 1 I.5 + 5 or better 0 3.2 0 0

14 Radiation Oncology ??Biology 0 Physics January 1980, Volume 6. No. I
Table 6. Survival after whole brain irradiation, by primary site and dose
3 .cquomous Cell corcrnomo ., Aden~corcmomo . Oat Cdl Corcrnomo
p= 0006
z 60; \\ al 0 1 \4
-
ii
a 40
1
20 1
1 0 i : !kk% Q,
0123456789
Years
Fig. 3. Overall survival in patients with lung cancer metastatic to brain by histology.
cell carcinoma and squamous cell carcinoma, (both around IO months) (Figure 3).
If all patients in this series, regardless of primary site, histology, or treatment fractionation, are analyzed according to Karnofsky scale scores before and after treatment, the results can be displayed graphically (Fig- ure 4). Once again, a shift to the right (favorable response) of about one interval (10%) is demonstrated. The relative frequency of patients at the higher end of the performance status scale has been increased.
80 - Before Irradiation ----- After lrrodiotion
Karnofsky Score
Fig. 4. Change in Karnovsky scale after whole brain irradia- tion.
The survival of patients from treatment of intracranial Because of scarce information in the hospital charts. metastases to last follow-up according to the dose and evaluation of duration of response or length of remission time factors used was tabulated comparing those who was extremely difficult, if not impossible. in this series, as received 3,500 rad or more to those who received 3,000 well as in others.” lo Nonetheless, from the data one can rad or less (Table 6). After whole brain irradiation, the suggest the following for consideration: (I) The rnedian
53000 rad* 23500 rad* months months
Primary site (no. pts.) (no. pts.) P value
Lung 1.19 8.75 ,212 (Ijjj (6)
Breast 5.78 5.68 ,976
(101) (45)
*See Tables I and 2 for details of fractionation employed for these doses.
survival of 75 patients who had no other evidence of distant metastases when they presented for irradiation was not significantly longer compared with the remainder of the patients in this series.
DISCUSSION Cancer that metastasizes to the brain is usually multi-
focal even though diagnostic tests may not demonstrate multiplicity. It has been stated that approximately 80% of cases actually involve multiple metastases.” Raskind” et al have demonstrated a majority of lesions in the distribution of the middle cerebral artery.
As previously mentioned, many other factors influence the course and survival of patients who develop brain metastases. In this group of patients we found that approximately 17% developed lethal complications from other treatments sometime after whole brain irradiation, in another 53% it could not be determined from the chart if complications were present. Complications included entities such as myelosuppression with or without sepsis and pulmonary and cardiac injuries and their ramifica- tions. These complications appeared to result from chemotherapy damage to tissues and organ systems. It was also interesting that control of the primary tumor had decreased from 65% at the time of diagnosis of intracranial metastases to 47% at the time of the last follow-up. The implications of this finding relate more to evaluation of patient survival than to etfectiveness of whole brain irradiation in terms of symptomatic improve- ment.
In a group of 376 evaluable patients, Nisce et al’ showed improvement in 80% after irradiation. Mean duration was five months, and median duration was three months. There was no difference among patients who were treated with 3,000 rad in 3 to 4 weeks and those who were treated with 3,500 to 4,000 rad in 3 to 4 weeks. Other authors’.‘.J.7.“,‘0 agree with those findings. Patients who underwent craniotomy for their metastatic disease did not fare better.“,”

Intracranial metastases 0 J. WEST and M. MAOR 15
survival for all patients is in the order of 5 to 6 months, for a lengthy survival are very limited, even though the
after brain irradiation. regardless of the primary tumor. patient may not die directly as a result of the intracranial
in this and other studies, and (2) one is unable to disease. Development of brain metastases may reflect an demonstrate a statistically significant difference in increased aggressiveness and virulence of the disease that survival with higher versus lower dose techniques. This will soon lead to demise of the host. It seems unlikely that was true even among those patients with breast primar- more extensive and aggressive treatment to the brain ies, who have a longer survival (Table 6). This suggests would benefit the overall group. Individual considera- that once a patient develops brain metastases, prospects tions. of course. might modif) this approach.
REFERENCES I.
2.
3.
4.
5.
6.
7.
8.
Bowen. R.. Jr., Knapp. J.R., Collins, V.P.: Radiotherapy of cerebral metastases. Texas J. Med. 61: 894-898, 1965. Chu. F.C.H., Hilaris, B.B.: Value of radiation therapy in the management of intracranial metastases. Cancer 14: 577-581. 1961. Deutsch. M.. Parsons. .I.. Mercado, R.: Radiotherapy for intracranial metastases. Cancer 34: 1607-l 6 I I. 1974. Horton, J.. Baxter. D.H.. Olson. K.B.. and The Eastern Cooperative Oncology Groups: The management of metas- tases to the brain by irradiation and corticosteroids. Am. J. Roenrgenology. 111: 334-336. 1976. Karnofsky, D.A., Abelmann. W.H., Craver, L.F., Burche- ma]. J.H.: The use of nitrogen mustards in the palliative treatment of Carcinoma. Cancer 1: 634-656, 1948. Lang. E.F.. Slater. J.: Metastatic brain tumors: Results of surgical and nonsurgical treatment. Surg. Clin. North Am. 44: 86-s-872. 1964. Lokick. J.J.: The management of cerebral metastases. J.A.M.A. 234: 748-751. 1975. Montana, G.S.. Meacham. W.F.. Caldwell. W.1.: Brain
9.
IO.
II.
12.
13.
irradiation for metastatic disease of lung origin. Cancer 29: 1477-1480. 1972. Nisce. I.Z.. Hilaris. B.S.. Chu. F.C.H.: A review of experi- ence with irradiation of brain metastases. Am. J. Roenrge- nol. 111: 329-333. 1971. Order, S.E., Hellman. S.. Von Essen. C.F.. Kligerman, M.M.: Improvement in quality of survival followinp whole brain irradiation for brain metastases. Radio1og.r 91: 149- 153. 1968. Raskind. R.. Weiss, S.R.. Manning. J.J.. Wermuth. R.E.: Survival after surgical excision of single metastatic brain tumors. Am. J. Roentgenol. 3: 323-328. 197 I. Perese. D.: Prognosis in metastatic tumors of the brain and skull: An analysis of 16 operative and I62 autopsied cases. Cancer 12: 609-613, 1959. Withers, H.R.. Harter. D.: Radiotherapy in the manage- ment of malignant melanoma. In Neoplasms of rhe Skin and Mulignunr Melanoma, The University of Texas System Cancer Center 20th Annual Clinical Conference. 1975. Chicago. Year Book Medical Publishers. Inc. 1976. pp 453-459.







![Index [rd.springer.com]978-1-59259-094-0/1.pdfIndex Brain (cont.), metastases, see Intracranial metastases parietal lobe tumors, 209 seizures and, 3-4 temporal lobe, see Temporal lobe](https://img.pdfslide.us/doc/110x75/5e70048b4c9c17787c3b4c70/index-rd-978-1-59259-094-01pdf-index-brain-cont-metastases-see-intracranial.jpg)