Embed Size (px)
Citation preview

Intracranial Dermoid Cyst Haemorrhage – an unusual cause of 6th Cranial Nerve Palsy
Dr N Tyagi, Dr K Zukhurova, Dr L Naidu
CASE REPORT A 28 year old previously fit and well man was admi6ed under our care with a 3 week history of ongoing severe band-‐like headaches and sudden onset of horizontal binocular diplopia worst on le@ lateral gaze. He took no regular medicaCons and had no known allergies. There was no family history of note.
Clinical findings On physical examinaCon he was unable to abduct the le@ eye on le@ lateral gaze. There was no nystagmus. Pupils were equal and reacCve to light, and there was no relaCve afferent pupillary defect. There was an associated le@ sided upper motor neurone 7th cranial nerve palsy. There was no further focal neurological deficit. Systemic examinaCon was normal. On orthopCc assessment he had 0.5 prism dioptres of diplopia on le@ lateral gaze. Hess chart has shown le@ lateral rectus muscle weakness as a result of a le@ abducens nerve palsy of recent onset. On ophthalmic examinaCon his visual acuiCes were 6/6 unaided in both eyes. There was no evidence of abnormal head posturing. Intraocular pressures were 12 mmHg in each eye . Fundoscopy was normal, with no evidence of papilloedema.
Radiological findings
Fig 2. Computed tomography (CT) scan demonstrates a well-‐defined low density brainstem lesion measuring -‐6 Hounsfield units (HU) consistent with fat
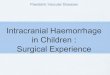
Fig 3. MRI Head T1 weighted sagi6al image: 10mm hyperintense lesion of two different signals. Hyperintensites consistent with fat on top and blood at bo6om . Lesion located in brainstem at the level of the le@ 6th cranial nerve nucleus
Fig 4. MRI head T2 weighted axial image: Evidence of hyperintense fat level superiorly and hypointense blood level inferiorly within the cyst
Fig 5. MRI head with gadolinium axial image: bright but lost differenCaCon of levels in keeping with haemorrhage.
Fig 7. Diffusion Weighted Imaging: No restricCon of diffusion. No evidence of infarct or abscess.
Fig 8. MRA head and neck: no relaCon of lesion to any major vessels.
Management PaCent was referred for neurosurgical opinion. Unfortunately, a@er much mulC-‐disciplinary team (MDT) discussion, it was decided he was not a good surgical candidate due to locaCon of lesion in brainstem. He was managed conservaCvely with an occluding eye patch iniCally, then with glasses fi6ed with prisms. He had no symptomaCc improvement a@er 6 months, and repeat MRI has shown an enlargement of the dermoid cyst. There is ongoing neurology and ophthalmology input.
Learning Points -‐Dermoid cysts are rare intracranial tumours -‐Complica7ons are related to size and loca7on -‐Haemorrhage into dermoid cyst is an extremely rare complica7on -‐Dermoid cysts appear hyperintense on T1 and T2 weighted MRI -‐Surgical management is ideal but depends on its loca7on
References (1) Azarmina M, Azarmina H. The Six Syndromes of the Sixth Cranial Nerve. J Ophthalmic Vis Res 2013 April 2013;8(2):160-‐171. (2) Orakcioglu B, Halatsch ME, FortunaC M, Unterberg A, Yonekawa Y. Intracranial dermoid cysts: variaCons of radiological and clinical features. Acta Neurochir (Wien) 2008 Dec;150(12):1227-‐34; discussion 1234. (3) Chen JC, Chen Y, Lin SM, Tseng SH. Sylvian fissure dermoid cyst with intratumoral hemorrhage: case report. Clin Neurol Neurosurg 2005 Dec;108(1):63-‐66. (4) Sanchez-‐Mejia RO, Limbo M, Tihan T, Galvez MG, Woodward MV, Gupta N. Intracranial dermoid cyst mimicking hemorrhage. Case report and review of the literature. J Neurosurg 2006 Oct;105(4 Suppl):311-‐314. (5) Alam K, Varshney M, Aziz M, Maheshwari V, Haider N, Gaur K, et al. Dermoid cyst in brain. BMJ Case reports 2011. (6) Triple6 TM, Griffith A, Hatanpaa KJ, Barne6 SL. Dermoid Cyst of the Infratemporal Fossa: Case Report and Review of the Literature. J Neurol Surg Rep 2013 12th December 2013;75(1):e33-‐e37. (7) Mamata H, Matsumae M, Yanagimachi N, Matsuyama S, Takamiya Y, Tsugane R. Parasellar dermoid tumor with intra-‐tumoral hemorrhage. Eur Radiol 1998;8(9):1594-‐1597. (8) Luan Y, Wang H, Zhone Y, Bian X, Luo Y, Ge P. TraumaCc Hemorrhage within a Cerebellar Dermoid Cyst . Int J Med Sci 2011 5th November 2011;9(1):11-‐13.
BACKGROUND
Intracranial dermoid cysts are rare benign congenital tumours that account for less than 1% of all brain neoplasms. They occur as a developmental anomaly in which embryonic ectoderm is trapped in the closing neural tube between the 5th-‐6th weeks of gestaCon. Throughout life they enlarge by desquamaCon of normal cells and secreCon of dermal elements such as fat and hair into a cysCc cavity, rather than cell division. Dermoids have epidermal contents such as hair follicles, sweat and sebaceous glands. The sebaceous glands handle the secreCon of sebum that imparts the characterisCc appearance of these lesions on CT and MRI, as shown in this case report. Intracranial dermoid cysts are mostly asymptomaCc , but can present in first 3 decades of life due to their mass effect (e.g. compression of adjacent structures) or their rupture with leakage of sebum into subarachnoid space resulCng in asepCc meningiCs. Dermoid cysts are poorly vascularised structures, and a haemorrhage into a dermoid cyst is a very rare event. This case report describes a le@ sixth nerve palsy caused by a haemorrhage into an intracranial dermoid cyst. The CT and MRI images show the characterisCc appearances of an intracranial dermoid -‐ they have low a6enuaCon (fat density) on CT, high signal on T1-‐ and T2-‐weighted MRI images and typically they do not enhance a@er contrast administraCon.
Fig 1. Hess Chart
DISCUSSION -‐CT and MRI imaging are consistent with haemorrhage within an intracranial dermoid cyst at the level of 6th cranial nerve nucleus. This is the site where the 7th cranial nerve fibres wrap around the abducens nucleus, explaining the cause of the associated le@ facial nerve palsy in this paCent. -‐Imaging demonstrates a fluid level (blood) inferiorly. This is a rare event due to poor vascularisaCon of dermoid cysts -‐Surgical resecCon remains treatment of choice and histopathology would be diagnosCc. However, due to the locaCon, in this case it was not amenable for this. If surgically excised, recurrence is uncommon. The risk of malignant transformaCon is rare, but development of squamous cell carcinoma has been reported.
Fig 6. T2 Gradient Echo Image demonstraCng signal dropout at the base of lesion. Consistent with blood products (haemosiderin)