Embed Size (px)
Citation preview

Catheterization and Cardiovascular Diagnosis 26:212-214 (1992)
lntracoronary Thrombus: Chronic Urokinase Infusion and Eva1 uat ion With I nt ravascu lar U It rasou nd
Ashit Jain, MD, Stephen R. Ramee, FAD, Juan Mesa, MD, Tyrone J. Collins, Christopher J. White, MD
MD, and
Percutaneous revascularization of coronary arteries with intraluminal thrombi is a clinical problem. We report a patient in whom we administered prolonged infusion of intracoro- nary urokinase and then assessed the stenosis with intravascular ultrasound before and after atherectomy. We found both angiography and intravascular ultrasound to be mis- leading in determining the presence of residual thrombus after thrombolysls. c 1992 Wl loy-L Ia~. Inc
Key words: thrornbolysis, atherectomy, coronary thrombus
INTRODUCTION
The optimal treatment of patients with unstable angina and large intraluminal thrombi has not been established. Options include prolonged anticoagulation, systemic or intracoronary thrombolysis, percutaneous transluminal angioplasty, and coronary artery bypass surgery. Balloon angioplasty is associated with an increased incidence of abrupt reocclusion in this setting, and is generally avoided unless the patient has ongoing ischemia [ 1,2]. Newer percutaneous interventions such as atherectomy and stenting are also not recommended in the presence of intracoronary thrombi. A prolonged urokinase infusion through an in-dwelling catheter has been shown to be an effective method of thrombolysis prior to mechanical in- tervention, but it has not been shown to decrease the incidence of complications or restenosis [3,4].
Intravascular ultrasound can quantitatively assess cor- onary artery stenoses after percutaneous interventions [5 ] and can qualitatively assess plaque, dissections, and the presence of calcium [6]. Thrombus on ultrasound has been described as having a homogeneous speckled ap- pearance [7,8]. Whether this intravascular ultrasound ap- pearance is specific enough to differentiate thrombus from soft atherosclerotic plaque is uncertain. The follow- ing case combines the use of a prolonged intracoronary urokinase infusion and evaluation of a lesion with sus- pected thrombus by an intravascular ultrasound.
CASE REPORT
CB is a 40-year-old male, referred for catheterization 5 days after an acute myocardial infarction with post- infarction angina. Angiography revealed a 95% stenosis of the proximal left circumflex artery with a large in-
0 1992 Wiley-Llss, Inc.
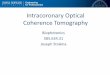
traluminal filling defect consistent with a thrombus ex- tending distal to the stenosis for 2 cm (Fig. 1A). He received intravenous heparin and 2,000 U/min of intra- coronary urokinase through a 6F Judkins left angio- graphic catheter (USCI, Boston, MA) for 16 h. Angiog- raphy performed at 16 h revealed complete resolution of the filling defect with an 80% residual stenosis (Fig. IB). This lesion was then studied with intravascular ultra- sound (Intertherapy, Inc., Anaheim, CA) using a 4.9F sheath. The ultrasound sheath was occlusive in the le- sion, representing a stenosis of more than 67% in diam- eter and 88% in area. By ultrasound, the lesion had a homogeneous speckled appearance, similar to what has been reported to represent thrombus [7,8] (Fig. ID). The lesion did not have dense fibrosis or calcification, mak- ing it feasible that it was all thrombus. Directional cor- onary atherectomy was then performed using a 7F device (Devices for Vascular Intervention, Redwood, CA). On gross inspection, the retrieved tissue consisted of soft, yellow plaque without thrombus (Fig. IF) and, micro- scopically, it was consistent with an atherosclerotic plaque (Fig. IG). By angiography the residual stenosis was 5% (Fig. 1C); however, intravascular ultrasound re- vealed the residual stenosis to be 33% by diameter and 6 1 % by area. After atherectomy the remaining lesion had the same speckled appearance as the initial lesion by ultrasound (Fig. 1E). The patient did not experience any complications and was discharged the day after atherec- From the Department of Internal Medicine, Section on Cardiology, Ochsner Medical Institutions, New Orleans, Louisiana.
Received June 24, 1991; revision accepted November 26, 1991.
Address reprint requests to Dr. Stephen R. Ramee, Section on Cardi- ology, Ochsner Medical Institutions, 15 14 Jefferson Highway, New Orleans, LA 70121.

A B C
D E
F G Fig. 1. A: Baseline angiogram with thrombus at the site of the lesion. B: Angiogram after thrombolysis. C: Final angiogram after atherectomy. D: lntravasculer ultrasound before atherectomy. E: lntravascular ultrasound after atherectomy. F: Gross specimens retrieved after atherectomy. G: Histology of the tissue retrieved by atherectomy.

214 Jain et al.
tomy on aspirin and metoprolol, without prolonged oral or intravenous anticoagulation. He has been asymptom- atic and did not have ischemia on his treadmill test 2 months after atherectomy.
DISCUSSION
Previous studies have shown that mechanical interven- tion in the presence of thrombus is associated with in- creased incidence of abrupt reocclusion and embolization [1,2]. In our patient the initial angiogram revealed a large intracoronary thrombus with a critical stenosis of the circumflex artery. The prolonged infusion of uroki- nase through an angiographic catheter achieved complete thrombolysis angiographically , with a persistent residual stenosis of 80% in the patient’s left circumflex artery. The potential benefits of this mode of therapy are a rel- atively rapid thrombolysis with the possibility of earlier mechanical intervention and, theoretically, a decreased risk of abrupt reocclusion or embolization. This may also shorten the hospital stay when compared to conventional treatment with prolonged anticoagulation prior to percu- taneous transluminal coronary angioplasty (PTCA).
We used intravascular ultrasound to ascertain the se- verity of the stenosis and to determine whether the per- sistent stenosis following the thrombolytic infusion was due to thrombus or atherosclerotic plaque. By intravas- cular ultrasound the lesion had a homogeneous speckled appearance, which has been previously described as be- ing consistent with the presence of a thrombus [7,8]. The clinical presentation, filling defect seen on angiography , and response to thrombolysis all confirmed that throm- bosis was playing a major role in the pathologic process. The presence of a homogeneous speckled appearance after thrombolysis in an artery that appeared to be free of thrombus angiographically left us with a dilemma re- garding further management. We chose to use an atherectomy device to debulk and biopsy the lesion. The pathology results revealed the lesion to be an atheroscle- rotic plaque and not thrombus. Although the intravascu- lar ultrasound study helped in assessing the severity of residual stenosis, it was unable to distinguish soft plaque from thrombus by the present criteria. The distinction of thrombus from a plaque by intravascular ultrasound is not yet established and, until more data is available, we caution the use of this modality for determining the pres- ence of intracoronary thrombi.
CONCLUSIONS
This case demonstrates the successful use of pro- longed intracoronary thrombolysis for treating intracor- onary thrombi prior to mechanical intervention. It also suggests that soft plaque can have the same appearance by intravascular ultrasound as that reported to be char- acteristic of intravascular thrombus, making the differ- entiation of these two entities by intravascular ultrasound difficult.
ACKNOWLEDGMENTS
The authors wish to express their sincere appreciation to Leda L. Lupo for editing and preparing the rnanu- script.
REFERENCES
1. Mabin TA, Holmes Jr DR, Smith HC, Vlietstra RE, Bove AA, Reeder GS, Chesebro JH, Bresnahan JF, Orszulak TA: Intracoro- nary thrombus: Role in coronary occlusion complicating percuta- neous transluminal coronary angioplasty. J Am Coll Cardiol 5:
2. Sugrue DD, Holmes Jr DR, Smith HC, Reeder GS, Lane GE, Vlietstra RE, Bresnahan JF, Hammes LN, Piehler JM: Coronary artery thrombus as a risk factor for acute vessel occlusion during percutaneous transluminal coronary angioplasty: Improving re- sults. Br Heart J 5662-66, 1986.
3. HaNnann J , McKeever L, Teran J, Bufalino V, Marek J, Brown A, Goodwin M, Amirparviz F, Motarjeme A: Prolonged infusion of urokinase for recanalization of chronically occluded aortocoro- nary bypass grafts. Am J Cardiol 61:189-191, 1988.
4. Chapekis A, George B, Candela R: Rapid thrombus dissolution by continuous infusion of urokinase through an intracoronary perfu- sion wire prior to PTCA: Results in native coronaries and patent saphenous vein grafts. J Am Coll Cardiol 15:154A, 1990.
5 . Davidson CJ, Shiekh KH, Kisslo K, Miller MJ, Newman GE, Phillips HR, Stack RS: Intravascular ultrasound evaluation of cor- onary and peripheral interventional technologies. J Am Coll Car- diol 2:93A, 1991.
6. Tobis JM, Mallery J, Mahon D, Lehmann K, Zelesky P, Griffth J, Gessert J, Moriuchi M, McRae M, Dwyer M, Greep N, Henry WL: Intravascular ultrasound imaging of human coronary arteries in vivo: Analysis of tissue characterization with comparison to in vitro histologic specimens. Circulation 83:913-926, 1991.
7. Pandian NG, Kreis A, Brockway B: Detection of intra-arterial thrombus by intravascular high frequency two-dimensional ultra- sound imaging in vitro and in vivo studies. Am J Cardiol 65:
8. Ferguson JJ, Ober JC, Edelman SK, Willerson JT. Documentation of experimentally induced thrombus formation using intravascular ultrasound. J Am Coll Cardiol 2:217A, 1991.
198-202, 1985.
1280-1283,1990.