Embed Size (px)
Citation preview

IntracoronaryThrombolyticTherapyinaPatientwithSTElevationMyocardialInfarctionintheSettingofCarbonMonoxidePoisoning.
IlianaHurtadoRendón MD,AhmadAbdin MD,Yesha PatelMD,WilliamBaumanMD,KevinSilverMD,MBS,FACC,FSCAI,FASNC
SummaHealthSystem,AkronCityHospital,Akron,OH
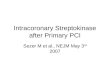
Figure1:EKGonPresentation Results/ReviewofLiterature• Thepatientdidnotsufferlongtermcomplicationandwas
followedupintheoutpatientsetting.• ThreemonthrepeatTTErevealedimprovementintheinferior
wallmotionabnormality.Apicalmyocardialakinesis remained.Ejectionfractionwasnormalat58%.
• IntracoronarythrombusisararecomplicationofCOpoisoningwithonly7reportedcasesintheliterature.
• Includingourpatient,5/8(62.5%)reportedweremen;agerange30-70yearsoldwithamean48.5years.
• Allpatientscomplainedofchestpain,exhibitedEKGchanges,andwerediagnosedatcardiaccatheterization.
• 3/8(37.5%)weretreatedbyballoonangioplasty,1/8(12.5%)wasnottreatedduetoconditionbeingfoundonpost-mortemautopsy,1/8(12.5%)treatedwithdrug-elutingstentplacement,1/8(12.5%)viahyperbaricchamber,1/8(12.5%)withsystemicthrombolytic,and1/8(12.5%)withcombinationofintracoronarythrombolytic,aspirationthrombectomy,andsystemicanticoagulation.[Figure7]
• All8(100%)werefoundtohaveathrombusintheLADartery.• 5/8(62.5%)hadcardiovascularriskfactorsorpreviouscardiac
events.• 7/8(87.5%)ofpatientssurvived.• Ourcaseinvolvestheyoungestpatientandisthefirsttobe
treatedwith acombinationofunfractionatedheparin,glycoprotein2b/3ainhibitor,intracoronarythrombolytic,aspirationthrombectomy,andoralanticoagulation.
Conclusions1. IntracoronarythrombusisararecomplicationofCOpoisoning.2. 100%ofpatientsreportedpresentedwithchestpain.3. PatientswereevaluatedwithserialEKG’s,cardiacbiomarkers,
andaTTE.Coronaryangiographyshouldbeconsideredwhenthereisevidenceofmyocardialinjury.
4. Theleftanteriordescendingarteryisthemostcommonlocationforthrombusformation.
5. Anti-thrombotictreatmentiscriticalwhenmyocardialinfarctionissuspected.
CaseRelevance• CarbonMonoxide(CO)isacolorlessandodorlesschemical
asphyxiantthatcausestissuehypoxiaresultinginmanifestationsinmultiplemajororgansincludingtheheart.
• Themechanismofmyocardialinjuryinvolves demandischemiawithorwithoutunderlyingcoronaryatherosclerosis.Fibrinolyticpathwayactivation duetoendothelialdamagefromoxygen-freeradicalsmayalsocontribute.
• WereportacaseofSTelevationmyocardialinfarctionduetoaleftanteriordescendingarterythrombusasararecomplicationfromacuteCOpoisoningandreviewallpatientsreportedintheliteratureinthe21st century.
PresentingHistory• History:32yearoldmalesummonedEMSforcomplaintsof
chestdiscomfort,headache,andnausea.Chestdiscomfortwasdescribedasaconstant,anteriorchestachewithoutradiationandassociatedwithnausea.Durationwas5hours.
• Itwasdiscoveredthatthepatientwasheatinghisapartmentbyleavingthedoorofhisgasovenopen.
• PastMedicalHistory: Hypertension• PhysicalExam.VS:BP=143/79;P=92/min.;R=22/min.
Patientwasnotinacutedistressonnon-rebreathermaskandmentationwasnormal.Lungswerecleartoauscultation.Cardiacexaminationrevealednormalrateandrhythmwithoutmurmurs,rubs,orgallops.Bedsidetransthoracicechocardiogramwasnotsignificantforpericardialeffusionorwallmotionabnormality.
• Lab.Carboxyhemoglobin:13.8.TroponinI:0.126.CKMB:115.CKMBIndex:4.5.Electrolytes:withinnormallimits
• Electrocardiogram(EKG):Normalsinusrhythm.ProlongedPRinterval.DiffuseSTelevations.[Figure1]
HospitalCourse• Patientwasadmittedtotelemetryandremainedwithout
furtherepisodesofchestpain.Overnight,TroponinIincreasedto10.7.CK-MBpeakedat168.
• Imaging:Transthoracicechocardiogram(TTE)wassignificantforwallmotionabnormalitiesintheapex,apical-inferior,septal,andapical-anteriormyocardialwalls.Ejectionfraction(EF)wasestimatedtobe55%.[Figure2,3]
• Telemetry:Multiplerunsofnon-sustainedventriculartachycardia- longestof5beats.
• CardiacCatheterization:Proximalleftanteriordescending(LAD)arterythrombuswith70%stenosisanddistalLADocclusion.Patientwastreatedwithunfractionatedheparinandglycoprotein2b/3ainhibitor(Tirofiban).[Figure4]
• Second Catheterization: Onthefollowingday,residualLADthrombuswasidentifiedwiththehelpofFractionalFlowReserveprocedure.Itwastreatedwithacombinationofintracoronarythrombolytic(Alteplase)andanaspirationthrombectomy.[Figure5]
• Hypercoagulabilitypaneldidnotrevealunderlyingpathologythatmayhavecontributedtothrombusformation.
• Patientwasultimatelydischargedonoralanticoagulation(Rivaroxaban)forthreemonths.
Figure4.InitialCardiacCatheterization
Figure2.TTEdepictingsystole
SelectedReferences1. Selcuk Oetal.VeryLateStentThrombosisinaPatientPresentingwithAcuteCarbonMonoxidePoisoning.JEmerg MedCaseRep2017;8:37-39.
2.Unlu Metal.Thrombolytictherapyinapatientwithinferolateralmyocardialinfarctionaftercarbonmonoxidepoisoning.SageJournals2015.
3.MarilouCCetal.Intracoronarythrombusformationfollowingcarbonmonoxidepoisoning.JForensicSciences2017;
4. Dziewierz Aetal.PrimaryangioplastyinpatientwithST-segmentelevationmyocardialinfarctioninthesettingofintentionalcarbonmonoxidepoisoning.JEmerg Med2013;45(6)831-834.
5. Soohyun Ketal.AcaseofacutecarbonmonoxidepoisoningresultinginanSTelevationmyocardialinfarction.KoreanCirc J2012;42(2)133-135.
6.Gonullu Hetal.STelevationmyocardialinfarctionduetocarbonmonoxidepoisoning.EurasianJMed2011;43(2):125-128.
7.Marius-NunezA.Myocardialinfarctionwithnormalcoronaryarteriesafteracuteexposuretocarbonmonoxide.Chest1990;97(2);491-494.
8. Satran etal.Cardiovascularmanifestationsofmoderatetoseverecarbonmonoxidepoisoning.JAmCollCardiology2005;45(9);1513-1516.
9.GandiniCetal.Carbonmonoxidecardiotoxicity.JToxicol Clin Toxicol 2001;39:35-44.
Figure7LADThrombusInterventions
Number Percent
BalloonAngioplasty 3 37.5%
NotTreated 1 12.5%
DrugElutingStent 1 12.5%
HyperbaricOxygenChamber 1 12.5%
SystemicThrombolytic 1 12.5%
CombinationofGlycoprotein2b/3ainhibitor,Intracoronarythrombolytic,AspirationThrombectomy
1 12.5%
Total 8 100%
Figure3.TTEdepictingdiastole
Figure5.SecondLookCardiacCatheterization