Embed Size (px)
Citation preview
Intracellular bacterial communities ofuropathogenic Escherichia coli inurinary tract pathogenesisGregory G. Anderson1, Karen W. Dodson1, Thomas M. Hooton2 and Scott J. Hultgren1
1Department of Molecular Microbiology, Washington University School of Medicine, Box 8230, 660 S. Euclid Ave., St Louis, MO
63110, USA2Department of Medicine, Division of Allergy and Infectious Diseases, University of Washington School of Medicine, Box 359930,
Harborview Medical Center, 325 Ninth Ave., 2WC-516, Seattle, WA 98104, USA
Urinary tract infections in young, healthy women
frequently recur, despite their traditional classification
as acute infections. Conventional wisdom dictates that
uropathogens causing recurrent infections in such
individuals come from the fecal or vaginal flora, in the
same manner as the initial infection. However, recent
studies of uropathogenic Escherichia coli have found
that it can carry out a complex developmental program
within the superficial epithelial cells of the mouse
bladder, forming intracellular bacterial communities
with many biofilm-like properties. These intracellular
biofilms allow the bacteria to outlast a strong host
immune response to establish a dormant reservoir of
pathogens inside the bladder cells. Re-emergence of
bacteria from this reservoir might be the source
of recurrent infection.
Urinary tract infections (UTIs), considered among themost common of bacterial diseases, afflict a large pro-portion of the world population [1]. A majority of theseinfections occur in young, healthy women. In a largeprospective study of young, sexually active women, theincidence of UTI was w0.5 per person-year [2]. Morerecently, a population-based survey estimated that asmany as 11 million women in the United States had atleast one presumed UTI treated with an antibiotic in 1995,and that the cost for evaluation and management of UTIswas 1.6 billion dollars [1]. In this survey, the self-reportedincidence of UTI in women 18 years and older was 10.8%,and the cumulative lifetime risk of UTI was 60%. Evenepisodes of acute, uncomplicated UTI are associated withconsiderable morbidity, including 6.1 days of symptoms,2.4 days of restricted activity and 0.4 bed days [1]. Giventhat an estimated 130–175 million cases of UTI occurannually worldwide [3], the societal costs associated withUTI are huge. Themost common isolates from patients areuropathogenic Escherichia coli (UPEC), accounting forw80% of all acute, community-acquired UTIs [4]. Asidefrom UPEC, several other microorganisms can also causeUTI, most notably Staphylococcus saprophyticus, impli-cated inmost of the remaining UTI cases [5]. Patients with
Corresponding author: Scott J. Hultgren ([email protected]).Available online 24 July 2004
www.sciencedirect.com 0966-842X/$ - see front matter Q 2004 Elsevier Ltd. All rights reserve
complicating factors, such as diabetes, spinal cord inju-ries, urinary catheters, or hospitalization, can also presentwith UTI caused by Klebsiella pneumoniae, Proteusmirabilis, Enterococcus faecalis, Pseudomonas aerugi-nosa, Serratia marcescens and group B streptococci [4].Although traditionally thought of as acute and self-limiting, 27–44% of women with an initial UTI willexperience at least one recurrence of symptoms withinsix months, despite antibiotic therapy [5,6]. Althoughthese recurrent infections might occasionally be due to apersistent focus of infection, the majority have beenthought to be reinfections caused by the initially infectingstrain persisting in the fecal flora [7]. The bacteriaassociated with recurrent UTI often appear to be pheno-typically or genetically identical to the bacterial strainthat caused the initial infection, suggesting that selectedE. coli strains might become uniquely adapted forcolonizing and infecting their respective hosts [7]. Thesteady increase of antibiotic resistance [8] and occurrencesof clonal outbreaks of UPEC-associated UTIs [9] highlightthe need for greater understanding of the mechanisms ofUPEC pathogenesis.
UPEC have proven to be quite stealthy in its patho-genesis of the urinary tract, using a complex pathway tomediate infection and persistence in the face of a stronginnate host immune response. One of the most studiedabilities of UPEC is binding host tissues and particularorgan niches. UPEC accomplish this binding by assem-bling several different adhesive organelles on their sur-face, the most understood comprising P pili and type 1 pili[10]. These pili, assembled by the chaperone–usher path-way, display an adhesin molecule at their distal end [11].P pili display the PapG adhesin, which has been shown tobe required for pyelonephritic pathogenesis by binding togloboside present on human kidney cells [12]. By contrast,type 1 pili have been found to be vital for attachment to thebladder epithelium. The FimH adhesin on type 1 pili bindsmannose, and in the bladder FimH recognizes mannosy-lated residues present on uroplakin proteins that line theluminal surface of the bladder superficial epithelial cells[13]. FimH-mediated binding of the bladder epithelium isthe initial step in an intricate cascade of events leading to
Review TRENDS in Microbiology Vol.12 No.9 September 2004
d. doi:10.1016/j.tim.2004.07.005

Review TRENDS in Microbiology Vol.12 No.9 September 2004 425
the myriad of symptoms associated with acute UTI andpossible long-term residence of UPEC in the urinary tract.
UPEC virulence determinants
Other than type 1 and P pili, UPEC produce additionalfactors that influence disease progression (Table 1). Someof these virulence determinants are located on one ofseveral UPEC specific pathogenicity-associated islands[14]. A recent genomic analysis of a UPEC strain revealedthe presence of genes for ten putative chaperone–usherpilus systems, two putative type IV pili and at least sevenputative autotransporter proteins [15]. The large reper-toire of pilus systems might confer upon UPEC multiplebinding specificities and the capacity to colonize varioussites throughout the urinary tract and other environ-ments. Autotransporter proteins can also have adhesiveproperties or they might fill other roles, such as toxins,proteases, invasins, serum resistance factors and motilitymediators [16]. One UPEC specific autotransporter, Sat,appears to exert a toxic effect upon urinary tract cellsin vitro [17]. Incubation of bladder and kidney cells withSat-producing UPEC leads to extreme vacuolation in thecytoplasm of the host cells and possible loosening ofcellular junctions. In a mouse model of UTI, Sat alsoinduces cytoplasmic vacuolation and severe histologicaldamage in kidneys of infected laboratory animals [18].Two other UPEC-expressed autotransporter proteins, Picand Tsh, appear to have serine protease activity [19].These two proteins are expressed during infection inlaboratory mice and appear to be generally associatedwith pyelonephritis strains. UPEC also express an RTX(repeat in toxin) toxin called a-hemolysin (HlyA), oftenlinked with the P pilus operon [20]. HlyA forms pores in avariety of host cell membranes and can induce calciumoscillations in proximal tubule cells of infected rat kidneys[21]. These fluctuations might serve as second messengersduring immune activation of the host. Another toxinproduced by UPEC, cytotoxic necrotizing factor 1 (CNF-1),influences the host cell cytoskeleton by targeting the Rhofamily of GTP-binding proteins [22]. CNF-1 has beenshown to kill human bladder epithelial cells in vitro andinhibit phagocytosis of bacteria by human polymorpho-nuclear leukocytes (PMNs) [23]. In addition to proteasesand toxins, UPEC produce several iron acquisition
Table 1. Virulence determinants of uropathogenic Escherichia
coli
Factor Refs
Adhesins P pili [10]
Type 1 pili [10]
S pili [10]
Dr adhesins [10]
Toxins HlyA [20]
CNF-1 [23]
Sat [18]
Siderophores Aerobactin [24]
IroN [26]
IreA [24]
Proteases Pic [19]
Tsh [19]
Other Capsule [24]
LPS [24]
www.sciencedirect.com
systems, including aerobactin [24] and the more recentlydescribed IroN system [25,26]. These iron siderophoresscavenge available iron and enhance UPEC survival in thenutrient-limiting bladder environment. Finally, mostUPEC strains produce an acidic polysaccharide capsule,which protects the bacteria from phagocytosis by humanPMNs and inhibits activation of complement [24].
Host response to UPEC infection
The host counters the actions of UPEC upon the bladderby mounting a robust and dramatic response. Bladdersuperficial epithelial cells express Toll-like receptor 4(TLR-4) on their membrane, which, along with CD14,recognizes lipopolysaccharide from the bacteria andactivates an innate immune response [27,28]. A burst ofinflammatory cytokines leads to a massive infiltration ofneutrophils to fight the infection [29,30]. Further,increased transcription of inducible nitric oxide synthaseby PMNs and the bladder epithelium results in high levelsof nitric oxide and related breakdown products, whichcould have toxic effects on the bacteria [31,32]. Uponinfection, the bladder epithelium is triggered to exfoliatesuperficial facet cells [33]. This aids clearance of anytissue-associated bacteria [34]. The underlying epi-thelium, normally extremely inert [35], rapidly undergoesa renewal process wherein underlying epithelial cellsproliferate and differentiate to replace the superficiallayer of cells [36]. Despite the defensive immune arsenaland rapid epithelial turnover, UPEC are able to colonizethe bladder and establish a persistent reservoir which canlast at least several months after infection in laboratorymice [37]. Bacteria persist in the bladder notwithstandingantibiotic treatment [38], and, periodically, bacteriaarising from this reservoir are shed in the urine of thesemice. Human patients have also been shown to shedbacteria in the urine, even in the absence of active UTIsymptoms [39,40]. Therefore, UPEC appear to be quiteadept at establishing a protective niche for themselves inthe bladder and persisting for extended periods of time.
Intracellular bacterial communities
Recently, it was discovered that UPEC activate a complexdevelopmental cascade upon their entry into superficialbladder cells [41,42]. This cascade was elucidated usingstate of the art microscopy, including scanning andtransmission electron microscopy, immunohistochemistryand time-lapse videomicroscopy. For videomicroscopy,mouse bladders infected with green fluorescence protein-expressing UPEC were stretched on an incubationchamber and placed on an epifluorescence microscope[42]. Images were captured every 30 seconds to twominutes, and multiple overlapping time frames wereexamined to piece together a timeline of UTI progression.Using these techniques, it was found that, in the earlystages, the bacteria invade the superficial cells and rapidlydivide. As the bacteria grow, dramatic phenotypicswitches result in the establishment of intracellularbacterial communities (IBCs) (Figure 1). IBCs progressthrough several stages, culminating in the formation ofbiofilm-like communities inside the superficial cells.Eventually, bacteria detach from the biofilm and burst
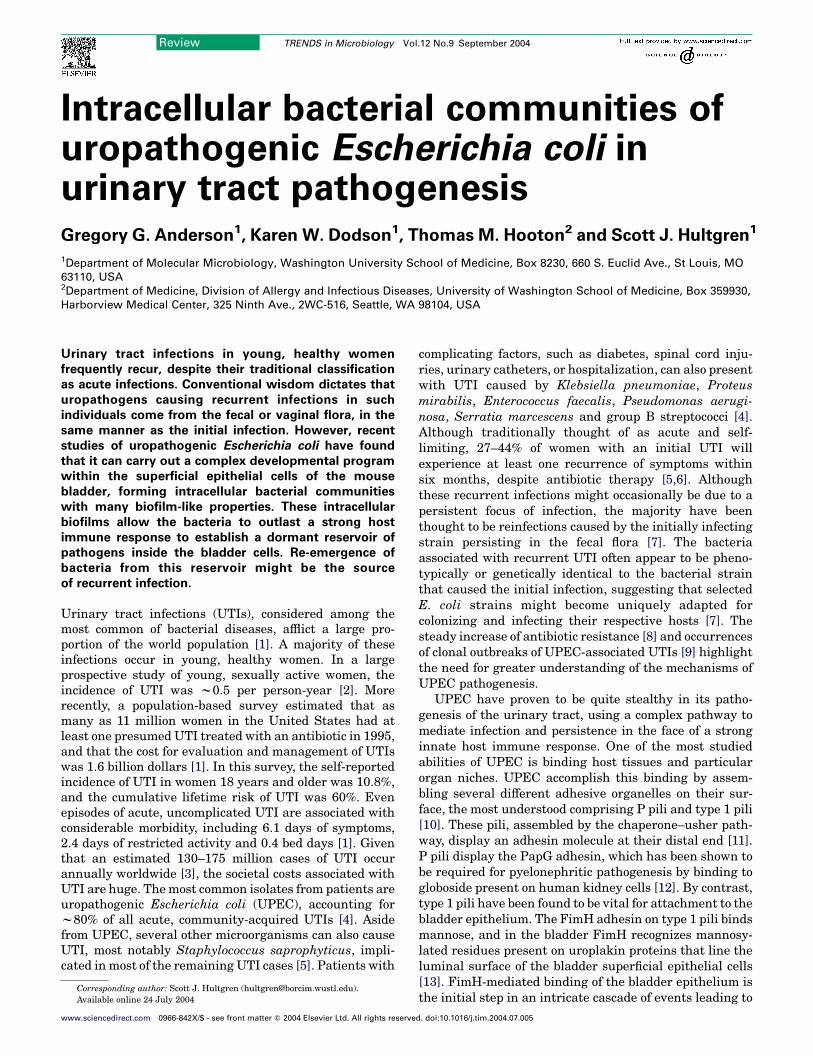
Figure 1. Middle intracellular bacterial communities (IBCs) are seen as ‘pods’ on the
surface of infected mouse bladder epithelium. (a) Numerous pods cover the
bladder surface in this scanning electron micrograph. Formation of biofilm-like
pods protects the bacteria from immune clearance, thus allowing uropathogenic
Escherichia coli (UPEC) to build up to extremely high levels in the bladder. Scale
bar, 50 mm. (b) Magnification of a pod reveals a smooth shell which is the uroplakin-
coated luminal membrane of the bladder superficial epithelial cell. The pod consists
of one cell that is completely filled with intracellular bacteria. Scale bar, 5 mm. (c) An
IBC is visible inside the bladder epithelium by fluorescent microscopy. Scale bar,
20 mm. The green fluorescence protien-expressing bacteria form a dense sphere
within the bladder cell. IBC progression can be monitored by time-lapse
videomicroscopy, in which time-lapse images are captured by epifluorescence
microscopy [42].
Review TRENDS in Microbiology Vol.12 No.9 September 2004426
out into the bladder lumen. These escaped bacteria thenrebind to the epithelium and initiate another round of IBCformation. The downstream effects of this cascade mightpermit UPEC to evade the host immune response andpersist in the urinary tract.
Binding and early IBC formation
Type 1 pili, with the FimH adhesin at the distal tip, arecrucial for UPEC attachment to the bladder epithelium[43]. Two lines of evidence confirm the vital role of FimHfor bacterial attachment to the epithelium. First, isogenicfimHmutants are defective for binding and colonization ofthe bladder [33]. Second, polystyrene latex beads coatedwith FimH readily associate with, and are internalized by,human bladder epithelial cells in vitro [44]. FimH binds tomannosylated uroplakins on the bladder epithelium via adeep acidic pocket formed at the tip of the lectin-bindingdomain [13]. Four different uroplakin molecules associateinto hexameric rings, which are arrayed in crystallineplaques on the luminal membrane of the bladder super-ficial epithelial cells. This uroplakin plaque provides apermeability barrier to prevent toxic molecules concen-trated in theurine fromdiffusing into deeper tissues [35,45].High resolution freeze-fracture electron microscopy hasrevealed that the tips of type 1 pili, which contain theadhesin, are buried in the central cavity of the uroplakinhexamers, tethering the bacteria to the epithelium [33]. Itwas recently shown that shear force enhances FimH-mediated binding [46], and such forces when encountered
www.sciencedirect.com
in the bladder might increase the ability of type 1 piliatedorganisms to attach and colonize the urinary tract.
After bacterial attachment, UPEC quickly invade thebound epithelial cell [44,47]. This key event occurs one tothree hours after initial inoculation. It has been shownusing tissue culture models that binding activates the Rhofamily of small GTP-binding proteins, specifically RhoA,Cdc42 and Rac1, which then activate focal adhesin kinase,phosphoinositide 3-kinase, a-actinin and vinculin. Theseprocesses result in localized actin rearrangements andmembrane extensions around the bacteria [47]. Themembrane engulfs the bacteria, leading to UPEC intern-alization via zipper-like phagocytosis.
Once intracellular, UPEC rapidly grow and divide,forming small clusters of bacteria, termed ‘early IBCs’[42]. Early IBCs have previously been called ‘bacterialfactories’ owing to the ability of UPEC to usurp thesuperficial bladder cells and convert them into factoriesfor bacterial growth [37]. A major benefit that invasionand establishment of an intracellular community confersupon UPEC is protection from killing by antibiotics, whichhas been shown both in vitro and in vivo [37,38]. In thisway, UPEC form a protective niche in the bladder wherethey can hide and survive. The bacteria within the earlyIBC divide rapidly during the first six to eight hours afterinoculation, with a doubling time of w30 to 35 minutes.The bacteria at this stage orient themselves randomly inthe cytoplasm of the host cell, such that they form anamorphous, loosely associated bacterial clump [42].During this period of quick expansion, UPEC maintaintheir typical rod morphology, with an average length of3 mm. This fast growth leads to a surge of microorganismswithin the bladder early in infection.
IBC maturation and middle IBCs
Between six to eight hours postinoculation, early IBCsexperience a dramatic phenotypic switch [42]. A remark-able drop in bacterial growth rate, resulting in doublingtimes greater than 60 minutes, takes place concurrentwith a significant shortening of bacterial morphology to anaverage 0.7 mm. At the same time, the amorphous clumpappears to come together to form a tight, highly organizedsphere inside the host cell. These events represent amaturation of the early IBC into a middle IBC stage withmany biofilm-like properties [41].
Bacterial biofilms are often associated with long-termpersistence of organisms in various environments. Bio-films are collections of bacteria that are attached to asurface, or to each other, and that display communitybehavior [48]. Initial events in biofilm formation involvebinding of planktonic bacteria to a surface and formationof small bacterial clusters called microcolonies. As thesemicrocolonies grow into mature biofilms, the bacteriadifferentiate, undergo dramatic phenotypic changes andencase themselves in an extracellular polysaccharidematrix [49,50]. These actions result in a large three-dimensional structure, with subpopulations of bacteria atdifferent regions of this structure displaying altered genetranscriptional patterns [48]. It is thought that thesesubpopulations represent a division of labor, where eachgroup performs certain specialized functions that benefit

Review TRENDS in Microbiology Vol.12 No.9 September 2004 427
the whole community [51]. As the biofilm ages, a subset ofbacteria detach from the biofilm and revert to a planktonicstate, which allows for spread of organisms to other niches[48]. A biofilm lifestyle benefits the bacteria by providingprotection from environmental insults and changes [49].Bacteria in biofilms display dramatically increased resist-ance to antibiotics because of the inability of antibiotics topenetrate the biofilm matrix, the slow growth-rate of thebacteria in the biofilm, physiological changes in thebacteria and biofilm-state expression of factors thatdirectly inhibit antibiotic activity [48,52]. In addition,biofilms confer increased resistance to host immune effectsupon their constituent bacteria by concealing the bacteriainside the biofilm matrix. For instance, bacteria inbiofilms are protected from opsonizing antibodies [48].Phenotypic variation and differentiation might alsoenhance bacterial resistance to PMNs and immuneeffector molecules [48]. Antibiotic and immune resistancesfacilitate bacterial biofilm survival in vivo during manydisease conditions, including native valve endocarditis,otitis media, chronic bacterial prostatitis, periodontitisand cystic fibrosis. Bacterial biofilms have also beendescribed on inert medical devices, such as prostheticheart valves, central venous catheters, contact lenses,intrauterine devices, urinary catheters and dental unitwater lines [48]. The presence of biofilms in disease or onmedical devices leads to chronic symptoms, owing topersistence of bacteria, despite antimicrobial therapy.
An important factor inE. coli biofilm formation is type 1pili, which aids stable attachment of the bacteria to asurface [53]. Flagella also assist biofilm formation bymediating initial weak surface contact and influencingexpansion of biofilms across a surface [53]. Antigen 43, anouter membrane autotransporter protein, promotes auto-aggregation of E. coli and can assist interbacterialinteractions during microcolony formation [54]. Thismight also be the function of secreted amyloid fiberscalled curli [55,56]. The regulator of the curli operon,CsgD, might also regulate several metabolic and otherfactors that influence formation of mature biofilms [57].A key process during biofilm maturation, followingattachment and microcolony formation, is secretion ofcolanic acid, an exopolysaccharide that creates a poly-saccharide matrix consisting of a complex three-dimen-sional architecture [58].
The incredible organization and structure produced byUPEC in the middle IBC are highly reminiscent ofbacterial biofilms [49]. As middle IBCs grow, the bacterialmass pushes against the epithelial cell membrane,creating a podlike protrusion on the surface of infectedbladder epithelium (Figure 1) [41]. Pods correspond to amiddle IBC. The bacteria in the middle IBC, although freein the cytoplasm, stay together as a spherical community,filling up much of the intracellular volume of a superficialumbrella cell. The surface of the pod is the luminalmembrane of the bladder cell, which is stretched tight,appearing smooth by scanning electron microscopy, and iscoated with an impermeable shell of uroplakin. Thebacteria inside the pod are highly organized and sur-rounded by numerous fibers emanating from the bacterialsurface. These fibers make extensive contacts with the
www.sciencedirect.com
surrounding matrix, creating individualized compart-ments for each bacterium that establish a spatialorientation of microorganisms inside the IBC. UPECexpress several factors in the middle IBC which areimportant for in vitro biofilm formation, including type1 pili and antigen 43 [41]. Similar to biofilms,expression of these factors is heterogeneous, with thebacteria setting up subpopulations with differentialgene expression. Polysaccharides are also presentthroughout the middle IBC.
By differentiating into an intracellular biofilm, UPECconstruct a safe haven where they can hide and wait outthe tide of the host immune attack. PMNs recruited to thebladder are targeted to the IBCs and attempt to clear thebacteria [29,42]. However, the IBC remains largelyunaffected. The uroplakin shell covering the IBC appearsto protect UPEC by denying the PMNs access to thebacteria. The structural organization of the pod might alsoprotect the bacteria from antibiotic susceptibility. Thematrix surrounding the bacteria inside the cell might alsoadd an additional layer of protection from antibiotics andthe immune system. It is interesting that in vitro biofilm-state UPEC have been found to be resistant, even whenantibiotics reach the bacteria [59], suggesting that thephysiological state of the microbes in biofilms enhancesbacterial survival. In this manner, UPEC are able toreplicate to large numbers, unperturbed by the host andother insults.
Late IBCs and fluxing
Eventually, the IBC progresses to a late stage [42].Starting around 12 hours postinoculation, bacteria onthe edge of the intracellular biofilm detach from the groupand differentiate into a typical rod morphology, with anaverage length of 2 mm. At this stage of the maturationcycle, the bacteria become highly motile. These motilebacteria swim toward the edge of the cell, burst out intothe bladder lumen in a process termed ‘fluxing’ and spreadout over the epithelium. Fluxing bacteria have also beenobserved erupting en masse from the epithelial cell, theentire community simultaneously emerging from itsintracellular hiding place [37]. It is possible that fluxinginitiates with a few bacteria, and as the host cellmembrane integrity decreases, some signal leads to theconcomitant bursting of the entire IBC. From the volumeof mature IBCs and the size of the bacteria, it is estimatedthat an average IBC contains in the order of 105
organisms. Fluxing of multiple IBCs, therefore, mightresult in the release of hundreds of thousands or millionsof UPEC back into the bladder lumen, leading to spreadwithin the bladder as well as dissemination back into theenvironment [42]. Escaped bacteria often filament, reach-ing up to 70 mm or greater in length [37,42]. Although themechanisms and purpose behind filamentation remainunclear, PMNs appear to have little effect upon thefilaments [42]. This allows UPEC to survive long enoughin the inflamed bladder to reattach to the epithelium.
UPEC persistence in the bladder
A second round of IBC formation occurs as escapedbacteria rebind and reinvade the superficial cells [42].

TRENDS in Microbiology
Binding and invasion Early IBC Middle IBC Late IBC
Figure 2. Schematic representation of the intracellular bacterial community (IBC) maturation program of uropathogenic Escherichia coli (UPEC) within the superficial
epithelium of the mouse bladder. Soon after inoculation, UPEC (green) bind and invade the superficial epithelial cells of the bladder in a process mediated by type 1 pili (red).
Rapid multiplication leads to formation of a disorganized bacterial clump within the cell cytoplasm, known as an ‘early IBC’. Activation of developmental cascades results in
maturation to a biofilm-like middle IBC. An impermeable uroplakin shell and the biofilm-like environment protect UPEC in the middle IBC from immune attack. Eventually,
UPEC detach from the intracellular biofilm, become motile (yellow flagella) and flux out of the cell into the bladder lumen. This presumably facilitates bacterial persistence
within the host and transmission to the environment. Fluxed UPEC can rebind to the epithelium to form additional generations of IBCs. The time scale for IBC progression is
dependent upon the bacterial strain and the host strain used. During infection with UPEC strain UTI89 in C3H/HeN mice, the first round of IBC development generally
completes within 24 hours after inoculation [42]. After several days, a quiescent bacterial reservoir develops in the bladder, which could be a seed for urinary tract infection
recurrence. Reproduced, with permission, from Ref. [42].
Review TRENDS in Microbiology Vol.12 No.9 September 2004428
However, this second round takes much longer toprogress, with doubling times in the early IBC of greaterthan 60 minutes. Multiple IBC cycles probably occur butafter several days, only a quiescent reservoir of smallintracellular bacterial clusters (doublets, quadruplets,small groups) remains in the bladder. The bladderepithelium is intact at this stage, with the bacteriaresiding inside superficial cells which appear smallerthan normal. These smaller superficial cells might resultfrom growth and differentiation of the underlying epi-thelial cells following exfoliation of the original superficialcells. As infection progresses, a greater number of fluxedUPEC might bind and invade the underlying epithelium,exposed during exfoliation. Physiological differencesbetween the superficial and underlying cells influencewhether IBCs form. Indeed, IBCs have never been seenwithin the underlying bladder cells. During this reservoirstage, no apparent actions are taken either by the host orthe bacteria, and UPEC can persist in this state in thebladder for months after an initial infection [37,38].Periodically during this persistent stretch, large numbersof organisms are seen in the urine [38]. It is thought thatreactivation of UPEC from their dormant reservoir state,and subsequent multiplication inside the bladder epi-thelium to re-form IBCs, lead to this bacterial spikein the urine.
Box 1. Intriguing questions for future study
† Do intracellular bacterial communities (IBCs) form in human
patients with cystitis?
† What genetic mechanisms do uropathogenic Escherichia coli
(UPEC) use to form IBCs?
† What accounts for polymorphonuclear leukocyte resistance by the
filaments?
† Why do IBCs form only in the superficial epithelial cells of the
bladder?
† What induces UPEC to become quiescent?
† Can stimulation of the dormant reservoir lead to a urinary tract
infection recurrence?
† What signals activate the dormant reservoir?
† How and when do known virulence determinants influence the IBC
cascade?
† What bacterial and/or host signals regulate IBC processes?
† How do IBCs relate to the chronic phase of infection?
† Are IBCs formed in other chronic recurrent infections?
Clinical impact
The discovery of the IBC maturation cascade suggeststhat UPEC possess a program that enables the bacteria toevade early innate immune defenses. Considering thatextracellular bacteria are readily cleared by PMNs [42],the formation of intracellular communities of bacteriainside the superficial cells of the bladder appears key tothe survival of UPEC in the urinary tract during the acutephases of infection (Figure 2). IBCs appear to permitUPEC to survive the immune onslaught that occurs atthese early stages. In this haven, the bacteria can safelymultiply, creating an overpowering legion which thenescapes into the bladder lumen. Presumably, the sheernumbers of bacteria that escape overwhelm the immunesystem, leading to several potential downstream effects:
www.sciencedirect.com
transmission back into the environment, subsequent IBCcycles and establishment of a chronic bacterial reservoir.Alternatively, formation of the reservoir might occurthrough an entirely separate route. Continuing studieswill provide answers to this and other fundamentalquestions relating to UPEC pathogenesis and persistence(Box 1). The elucidation of the IBC program was carriedout using a mouse model of infection. However, UPEC alsobind, invade and replicate inside human epithelial cellsin vitro [37,44,47], and it will be vital for future studies toestablish whether IBCs and quiescent reservoirs ofbacteria form in human patients. As more is understoodabout the factors that are expressed during UTI, and theirregulation, it will be essential to determine their role inthe IBC program. Such knowledge will provide a compre-hensive understanding of UTI progression and lead to newclues about how to abrogate UPEC infection. Further,because many different microorganisms invade hosttissues and multiply inside host cells, it is possible thatan IBC-like developmental program is important duringvarious stages of other chronic recurrent infections.A greater understanding of the nature of intracellularbacterial communities in chronic or recurrent infectionswill aid the development of new and more effectivetreatments for these problematic diseases.
Review TRENDS in Microbiology Vol.12 No.9 September 2004 429
Acknowledgements
We thank S. Justice, C. Hung and J. Palermo for helpful discussions. Thiswork was supported by National Institutes of Health grants AI29549,DK51406 and AI48689, and by ORWH SCOR grant DK64540 inpartnership with DHHS, NIDDK and the FDA.
References
1 Foxman, B. (2002) Epidemiology of urinary tract infections: incidence,morbidity, and economic costs. Am. J. Med. 113(Suppl. 1), 5S–13S
2 Hooton, T.M. et al. (1996) A prospective study of risk factors forsymptomatic urinary tract infection in young women.N. Engl. J. Med.335, 468–474
3 Russo, T.A. and Johnson, J.R. (2003) Medical and economic impact ofextraintestinal infections due to Escherichia coli: focus on anincreasingly important endemic problem. Microbes Infect. 5, 449–456
4 Ronald, A. (2002) The etiology of urinary tract infection: traditionaland emerging pathogens. Am. J. Med. 113(Suppl. 1), 14S–19S
5 Hooton, T.M. and Stamm, W.E. (1997) Diagnosis and treatment ofuncomplicated urinary tract infection. Infect. Dis. Clin. North Am. 11,551–581
6 Ikaheimo, R. et al. (1996) Recurrence of urinary tract infection in aprimary care setting: analysis of a 1-year follow-up of 179 women.Clin. Infect. Dis. 22, 91–99
7 Stapleton, A. and Stamm, W.E. (1997) Prevention of urinary tractinfection. Infect. Dis. Clin. North Am. 11, 719–733
8 Stamm, W.E. (2002) Scientific and clinical challenges in the manage-ment of urinary tract infections. Am. J. Med. 113(Suppl. 1), 1S–4S
9 Manges, A.R. et al. (2001) Widespread distribution of urinary tractinfections caused by a multidrug-resistant Escherichia coli clonalgroup. N. Engl. J. Med. 345, 1007–1013
10 Mulvey, M.A. (2002) Adhesion and entry of uropathogenic Escherichiacoli. Cell. Microbiol. 4, 257–271
11 Sauer, F.G. et al. (2000) Chaperone-assisted pilus assembly andbacterial attachment. Curr. Opin. Struct. Biol. 10, 548–556
12 Dodson, K.W. et al. (2001) Structural basis of the interaction of thepyelonephritic E. coli adhesin to its human kidney receptor. Cell 105,733–743
13 Hung, C.S. et al. (2002) Structural basis of tropism of Escherichiacoli to the bladder during urinary tract infection. Mol. Microbiol.44, 903–915
14 Hacker, J. et al. (1999) Pathogenicity islands of extraintestinalEscherichia coli. In Pathogenicity Islands and Other Mobile VirulenceElements (Kaper, J.B. and Hacker, J. eds), pp. 59–75, AmericanSociety for Microbiology
15 Welch, R.A. et al. (2002) Extensive mosaic structure revealed by thecomplete genome sequence of uropathogenic Escherichia coli. Proc.Natl. Acad. Sci. U. S. A. 99, 17020–17024
16 Henderson, I.R. and Nataro, J.P. (2001) Virulence functions ofautotransporter proteins. Infect. Immun. 69, 1231–1243
17 Guyer, D.M. et al. (2000) Identification of sat, an autotransporter toxinproduced by uropathogenic Escherichia coli.Mol. Microbiol. 38, 53–66
18 Guyer, D.M. et al. (2002) Sat, the secreted autotransporter toxin ofuropathogenic Escherichia coli, is a vacuolating cytotoxin for bladderand kidney epithelial cells. Infect. Immun. 70, 4539–4546
19 Heimer, S.R. et al. (2004) Autotransporter genes pic and tsh areassociated with Escherichia coli strains that cause acute pyelone-phritis and are expressed during urinary tract infection. Infect.Immun. 72, 593–597
20 Stanley, P. et al. (1998) Acylation of Escherichia coli hemolysin: aunique protein lipidation mechanism underlying toxin function.Microbiol. Mol. Biol. Rev. 62, 309–333
21 Uhlen, P. et al. (2000) Alpha-haemolysin of uropathogenic E. coliinduces Ca2C oscillations in renal epithelial cells. Nature 405,694–697
22 Mills, M. et al. (2000) Cytotoxic necrotizing factor type 1 ofuropathogenic Escherichia coli kills cultured human uroepithelial5637 cells by an apoptotic mechanism. Infect. Immun. 68, 5869–5880
23 Hofman, P. et al. (2000) Escherichia coli cytotoxic necrotizing factor-1(CNF-1) increases the adherence to epithelia and the oxidative burstof human polymorphonuclear leukocytes but decreases bacteriaphagocytosis. J. Leukoc. Biol. 68, 522–528
www.sciencedirect.com
24 Johnson, J.R. (2003) Microbial virulence determinants and thepathogenesis of urinary tract infection. Infect. Dis. Clin. North Am.17, 261–278
25 Russo, T.A. et al. (1999) Identification of genes in an extraintestinalisolate of Escherichia coli with increased expression after exposure tohuman urine. Infect. Immun. 67, 5306–5314
26 Sorsa, L.J. et al. (2003) Characterization of an iroBCDEN gene clusteron a transmissible plasmid of uropathogenic Escherichia coli:evidence for horizontal transfer of a chromosomal virulence factor.Infect. Immun. 71, 3285–3293
27 Schilling, J.D. et al. (2003) Toll-like receptor 4 on stromal andhematopoietic cells mediates innate resistance to uropathogenicEscherichia coli. Proc. Natl. Acad. Sci. U. S. A. 100, 4203–4208
28 Schilling, J.D. et al. (2003) CD14- and Toll-like receptor-dependentactivation of bladder epithelial cells by lipopolysaccharide and type 1piliated Escherichia coli. Infect. Immun. 71, 1470–1480
29 Schilling, J.D. et al. (2001) Bacterial invasion augments epithelialcytokine responses to Escherichia coli through a lipopolysaccharide-dependent mechanism. J. Immunol. 166, 1148–1155
30 Haraoka, M. et al. (1999) Neutrophil recruitment and resistance tourinary tract infection. J. Infect. Dis. 180, 1220–1229
31 Poljakovic, M. and Persson, K. (2003) Urinary tract infection in iNOS-deficient mice with focus on bacterial sensitivity to nitric oxide. Am.J. Physiol. Renal Physiol. 284, F22–F31
32 Poljakovic, M. et al. (2001) Escherichia coli-induced inducible nitricoxide synthase and cyclooxygenase expression in the mouse bladderand kidney. Kidney Int. 59, 893–904
33 Mulvey, M.A. et al. (2000) Bad bugs and beleaguered bladders:interplay between uropathogenic Escherichia coli and innate hostdefenses. Proc. Natl. Acad. Sci. U. S. A. 97, 8829–8835
34 Gunther, N.W.T. et al. (2001) In vivo dynamics of type 1 fimbriaregulation in uropathogenic Escherichia coli during experimentalurinary tract infection. Infect. Immun. 69, 2838–2846
35 Southgate, J. et al. (1999) Urothelial tissue regulation. Unraveling therole of the stroma. Adv. Exp. Med. Biol. 462, 19–30
36 Mysorekar, I.U. et al. (2002) Molecular regulation of urothelialrenewal and host defenses during infection with uropathogenicEscherichia coli. J. Biol. Chem. 277, 7412–7419
37 Mulvey, M.A. et al. (2001) Establishment of a persistent Escherichiacoli reservoir during the acute phase of a bladder infection. Infect.Immun. 69, 4572–4579
38 Schilling, J.D. et al. (2002) Effect of trimethoprim-sulfamethoxazoleon recurrent bacteriuria and bacterial persistence in mice infectedwith uropathogenic Escherichia coli. Infect. Immun. 70, 7042–7049
39 Anderson, M. et al. (2004) Viable but nonculturable bacteria arepresent in mouse and human urine specimens. J. Clin. Microbiol. 42,753–758
40 Hooton, T.M. et al. (2000) A prospective study of asymptomaticbacteriuria in sexually active young women. N. Engl. J. Med. 343,992–997
41 Anderson, G.G. et al. (2003) Intracellular bacterial biofilm-like pods inurinary tract infections. Science 301, 105–107
42 Justice, S.S. et al. (2004) Differentiation and developmental pathwaysof uropathogenic Escherichia coli in urinary tract pathogenesis. Proc.Natl. Acad. Sci. U. S. A. 101, 1333–1338
43 Gunther, I.N. et al. (2002) Assessment of virulence of uropathogenicEscherichia coli type 1 fimbrial mutants in which the invertibleelement is phase-locked on or off. Infect. Immun. 70, 3344–3354
44 Martinez, J.J. et al. (2000) Type 1 pilus-mediated bacterial invasion ofbladder epithelial cells. EMBO J. 19, 2803–2812
45 Lewis, S.A. (2000) Everything you wanted to know about the bladderepithelium but were afraid to ask. Am. J. Physiol. Renal Physiol. 278,F867–F874
46 Thomas, W.E. et al. (2002) Bacterial adhesion to target cells enhancedby shear force. Cell 109, 913–923
47 Martinez, J.J. and Hultgren, S.J. (2002) Requirement of Rho-familyGTPases in the invasion of Type 1-piliated uropathogenic Escherichiacoli. Cell. Microbiol. 4, 19–28
48 Donlan, R.M. and Costerton, J.W. (2002) Biofilms: survival mechan-isms of clinically relevant microorganisms. Clin. Microbiol. Rev. 15,167–193
49 Dunne, W.M., Jr. (2002) Bacterial adhesion: seen any good biofilmslately? Clin. Microbiol. Rev. 15, 155–166
Review TRENDS in Microbiology Vol.12 No.9 September 2004430
50 O’Toole, G. et al. (2000) Biofilm formation as microbial development.Annu. Rev. Microbiol. 54, 49–79
51 Webb, J.S. et al. (2003) Bacterial biofilms: prokaryotic adventures inmulticellularity. Curr. Opin. Microbiol. 6, 578–585
52 Mah, T.F. et al. (2003) A genetic basis for Pseudomonas aeruginosabiofilm antibiotic resistance. Nature 426, 306–310
53 Pratt, L.A. and Kolter, R. (1998) Genetic analysis of Escherichia colibiofilm formation: roles of flagella, motility, chemotaxis and type I pili.Mol. Microbiol. 30, 285–293
54 Danese, P.N. et al. (2000) The outer membrane protein, antigen 43,mediates cell-to-cell interactions within Escherichia coli biofilms.Mol.Microbiol. 37, 424–432
55 Prigent-Combaret, C. et al. (2001) Complex regulatory networkcontrols initial adhesion and biofilm formation in Escherichia colivia regulation of the csgD gene. J. Bacteriol. 183, 7213–7223
Have you contributed to a
Did you know that you are entitle
A 30% discount is available to ALL Elsevier book and journal contr
from us.
To take advantage of your discount:
1. Choose your book(s) from www.elsevier.com or www.books.elsev
2. Place your order
Americas:
TEL: +1 800 782 4927 for US customers
TEL: +1 800 460 3110 for Canada, South & Central America cu
FAX: +1 314 453 4898
E-MAIL: [email protected]
All other countries:
TEL: +44 1865 474 010
FAX: +44 1865 474 011
E-MAIL: [email protected]
You’ll need to provide the name of the Elsevier book or journa
orders within the US, Canada, and the UK.
If you are faxing your order, please enclose a copy of this pag
3. Make your payment
This discount is only available on prepaid orders. Please note
Elsevier Health Sciences products.
www.books.el
www.sciencedirect.com
56 Chapman, M.R. et al. (2002) Role of Escherichia coli curli operons indirecting amyloid fiber formation. Science 295, 851–855
57 Brombacher, E. et al. (2003) The curli biosynthesis regulator CsgDco-ordinates the expression of both positive and negative determi-nants for biofilm formation in Escherichia coli. Microbiol. 149,2847–2857
58 Danese, P.N. et al. (2000) Exopolysaccharide production is required for
development of Escherichia coli K-12 biofilm architecture.J. Bacteriol. 182, 3593–3596
59 Stone, G. et al. (2002) Tetracycline rapidly reaches all the constituentcells of uropathogenic Escherichia coli biofilms. Antimicrob. Agents
Chemother. 46, 2458–2461
n Elsevier publication?
d to a 30% discount on books?
ibutors when ordering books or stand-alone CD-ROMs directly
ier.com
stomers
l to which you have contributed. Shipping is FREE on pre-paid
e.
that this offer does not apply to multi-volume reference works or
sevier.com





























