Embed Size (px)
Citation preview

Volume 127, Number 2 American Heart Journal Suriani, Lansnm, and Konstadt 463
Fig. 2. Nuclear magnetic resonance imaging of heart. Sagittal long-axis view showing four chambers. Thrombus (arrow) located along posterior wall of left atrium.
changes, the capability to visualize may be decreased or even lost.5 In the present case the massive calcification of the atrium prevented the visualization of the atria, the left atria1 appendage, and the atria1 septum. We are not aware of previous reports of left atria1 calcification as a limitation of transesophageal echocardiography. Although magnetic resonance imaging cannot be considered an alternative technique to two-dimensional echocardiography in the routine assessment of patients with mitral stenosis, it can be of clinical relevance in patients who have poor echocar- diographic windows.6
REFERENCES
1.
2.
3.
4.
5.
6.
Aschenberg W, Schliiter M, Kremer P, Schriider E, Siglow V, Bleifeld W. Transesophageal two-dimensional echocardiogra- phy for the detection of left atria1 appendage thrombus. J Am Co11 Cardiol 1986;7:163-6. Leonard JJ, Katz S, Nelson D. Calcification of the left atrium. Its anatomic location, diagnostic significance and roentgeno- logic demonstration. N Ens1 J Med 1957:256:629-33. Matsuyama S, Watabe T, Kuribayashi S, botaki M, Suzuki Y, Sugihara M, Kawada S, Koide S, Shontsu A, Tomoda H. Plain radiographic diagnosis of thrombosis of left atria1 appendage in mitral valve disease. Radiology 1983;146:15-20. Lin SL, Hsu TL, Liou JY, Chen CH, Chang MS, Chiang HT, Chen CY. Usefulness of transesophageal echocardiography for the detection of left atria1 thrombi in patients with rheumatic heart disease. Echocardiography 1992;9:161-8. Freedberg RS, Weinreb J, Gluck M, Kronzon I. Paraesoph- ageal hernia may prevent cardiac imaging by transesophageal echocardiography. J Am Sot Echo 1989;2:202-3. Casolo GC, Zampa V, Rega L, Berti L, Filice M, Picchione N, Poggesi L. Evaluation of mitral stenosis by tine magnetic res- onance imaging. AM HEART J 1992;123:1252-60.
Intracardiac rheumatoid nodule presenting as a left atrial mass
Robert J. Suriani, MD, Steven Lansman, and Steven Konstadt, MD New York, N. Y.
Cardiac involvement with rheumatoid nodules is a com- plication of rheumatoid arthritis.’ When they are iden- tified, granulomas are most commonly observed within the cusps, along the bases of all four cardiac valves and, microscopically, within the myocardium and pericardi- um.‘, 2 We report on a case illustrating an unusual presen- tation of a rheumatoid nodule on the lateral wall of the left atrium (LA) in a patient undergoing aortic valve replace- ment.
A 78-year-old woman with progressive shortness of breath, chest heaviness, and syncope from severe aortic stenosis was seen for aortic valve replacement. Her medi- cal history was significant for hypertension and steroid- dependent rheumatoid arthritis for 10 years. At the time of surgery her medications were hydrochlorothiazide 25 mg
From the Departments of Anesthesiology and Surgery, Mount Sinai Med- ical Center. Reprint requests: Robert J. Suriani, MD, Department of Anesthesiology, Box 1010, Mount Sinai Medical Center, New York, NY 10029.
AM HEART J 1994;127:463-5 Copyright Z’ 1994 by Mosby-Year Book, Inc. OOOZ-8703/94/$1.00 + .lO 4/4/50672

464 Suriani, Lansman, and Konstadt February 1994
American Heart Journal
Fig. 1. Long-axis, two-chamber view demonstrating left atrium (LA) and left ventricle (Lb’). Note echodense mass (arrow) protruding from lateral wall of LA.
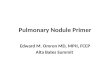
daily and prednisone 5 mg daily. The preoperative electro- cardiogram demonstrated sinus rhythm with left atria1 en- largement and left ventricular hypertrophy. A chest radio- graph was normal. Transthoracic echocardiography (TTE) demonstrated severe aortic stenosis and no evidence of a left atria1 mass. Cardiac catheterization revealed normal mitral valvular function, 3+ aortic insufficiency, and an aortic valve area of 0.9 to 1.0 cm3 with a 40 mm Hg gradi- ent. The left atrium appeared normal in size with no intraatrial masses. Surgical replacement of the aortic valve was planned. After induction of general anesthesia, intra- operative monoplane transesophageal echocardiography (TEE) was performed. A long-axis, two-chamber view showed the left atrium, the mitral valve, and the left ven- tricle. A 1 X 1 cm mass was noted on the lateral wall of the left atrium near the entrances of the left pulmonary veins (Fig. 1). The echo density of the mass was clearly different from the rest of the left atrium. It did not involve the mi- tral valve or the left atria1 appendage. Doppler color flow mapping demonstrated blood flow around the mass; pulsed- wave Doppler echocardiography revealed a typical pulmo- nary venous flow pattern. The differential diagnosis in- cluded abscess, clot, and tumor. Because of the potential complications of implanting a prosthetic valve in a patient with an intracardiac abscess, the surgeon decided to ex- plore the left atrium once cardiopulmonary bypass with aortic cross-clamping was instituted. The surgeon con- firmed the findings of a mass adherent to the lateral wall of the left atrium. The excised yellowish gray tissue mea- sured 1.2 X 1 x 0.3 cm and bad a soft consistency. Micro- scopic examination (Fig. 2) revealed basophilic, granular tissue with central necrosis, palisading histiocytes, and a fragment of thickened endocardium which, pathologically,
represent the contents of a rheumatoid nodule. Special stains for organisms and cultures were negative. Surgery was completed uneventfully, and the patient made an un- remarkable recovery. She was discharged from the hospi- tal on postoperative day 11.
The overall prevalence of cardiac abnormalities in pa- tients with rheumatoid arthritis has been reported to be 30% to 50%, with clinically detectable disease noted in only 2 sb to 10 % of cases.” Chronic pericarditis is the most common cardiac lesion.5 Demonstrable rheumatoid granu- lomas are rare, but granulomas have been reported in all parts of the heart: pericardium, epicardium, myocardium, endocardium, atrium, interventricular septum, and all valve cusps and rings (predominantly mitral and aortic).5 Most rheumatoid granulomas are of microscopic size; how- ever, well-formed macroscopic granulomas that are micro- scopically indistinguishable from classic subcutaneous nod- ules can develop within the aortic valve cusps and mitral valve leaflets. These granulomas characteristically involve the core of the valve, with sparing of the endocardium.6 In this case, the patient had no preoperative clinical or radio- graphic evidence of a left atria1 mass. Pathologic examina- tion of the excised left atria1 mass confirmed the diagnosis of a rheumatoid nodule. Furthermore, microscopic exam- ination of the aortic valve specimen revealed a fibrotic, calcified valve with a palisading granuloma exhibiting cen- tral calcified, necrotic material. In conclusion, we report the first TEE-diagnosed case of an intracardiac rheumatoid nodule. Echo densities commonly observed within the left atrium include clot, tumor, foreign body, abscess, or ana- tomic variant. Furthermore, this case showed that TEE is superior to transthoracic echocardiography in detecting left atria1 disease. Although the appearance of a rheuma-

Volume 127, Number 2
American Heart Journal Dingerkus et al. 465
Fig. 2. A, Rheumatoid nodule within atria1 wall (hematoxylin and eosin; x40). B, Note central necrosis and palisading histiocytes (hematoxylin and eosin; ~2001.
toid granuloma as a left atria1 mass is extremely rare, it must be considered in the differential diagnosis of a left atrial mass in aI1 patients with classic rheumatoid arthri- tis.
REFERENCES
1. Lebowitz WB. The heart in rheumatoid arthritis (rheumatoid disease). Ann Intern Med 1963;58:102-23.
2. Goehrs HR, Baggenstoss AH, Slocumb CH. Cardiac lesions in rheumatoid arthritis. Arthritis Rheum 1960;3:298-308.
3. Alam M, Sun I. Transesophageal echocardiographic evalua- tion of left atria1 mass lesions. J Am Sot Echocardiogr 1991;4:323-30.
4. Mody GM, Stevens JE, Meyers OL. The heart in rheumatoid arthritis-a clinical and echocardiographic study. Q J Med 1987;65:921-8.
5. Bonfiglio T, Atwater EC. Heart disease in patients with seropositive rheumatoid arthritis: a controlled autopsy study and review. Arch Intern Med 1969;124:714-9.
6. Reimer KA, Rodgers RF, Oyasu R. Rheumatoid arthritis with rheumatoid heart disease and granulomatous aortitis. JAMA 1976;235:2510-2.
Mediastinal chloroma affecting the right heart with superior vena cava syndrome
H. Dingerkus, MD,” H. Wller, MD,a A. Albrecht, MD, L. Hennig, MD,” H. Stein, MD,b and R. Schrader, MD”, Berlin, Germany
Superior vena cava syndrome (SVCS) may be a life- threatening event. Symptoms may include plethora, edema of the upper body, dilated neck veins, dyspnea, and dry
From the aDepartment of Medicine, Division of Cardiology/Pulmonology, and ‘Department of Pathology, Steglitz Medical Center, Free University of Berlin.
Reprint requests: Dr.med. Hanso Dingerkus, Medizinische Klinik und Po- liklinik, Kardiopulmologische Abteilung, Klinikum Steglitz, FU Berlin, Hindenburgdamm 30, D-1000 Berlin 45, Germany.
AM HEARTJ 1994;12'7:465-8 Copyright @ 1994 by Mosby-Year Book, Inc. 0002.8703/94/51.00 + .lO 4/4/506’75