Embed Size (px)
Citation preview

Intra-abdominal Infections
Resident’s Lecture
Edward L. Goodman, MD
May 1, 2006

Outline
• Pathogenesis of IAI
• Magnitude of problem
• Questions and Controversy
• Antimicrobial Regimens

Complicated Intra-Abdominal InfectionsDefinition
Extends beyond the hollow viscus of origin into the peritoneal space
Associated either with abscess formation or peritonitis
Requires either operative or percutaneous intervention to resolve
Solomkin J et al. Clin Infect Dis. 2003 Oct 15;37(8):997-1005.Mazuski J et al. Surgical Infections. 2002. 3(3):161-173.
Medical Illustration Copyright © 2005 Nucleus Medical Art,
All rights reserved. www.nucleusinc.com

Complicated Intra-Abdominal Infection Types
• Wide variety of conditions–Perforated gastroduodenal
ulcers–Biliary tract infections–Small bowel perforations–Complicated appendicitis
(with abscess or perforation) –Complicated diverticulitis
(with abscess or perforation)
Goldstein E. Clin Infect Dis 2002 Sep 1;35(Suppl 1):S106-11.
Medical Illustration Copyright © 2005 Nucleus Medical Art,
All rights reserved. www.nucleusinc.com

Complicated Intra-Abdominal Infections:Common PathogensFacultative and Aerobic Gram-Negatives
Escherichia coli Klebsiella spp Pseudomonas aeruginosa Proteus spp Enterobacter spp other gram-negatives
71.3% 14.3% 14.1% 5.2%5.1%
12.3%
Gram-Positive Organisms
Streptococcal spp Enterococcus faecalis Enterococcus faecium Enterococcus spp Staphylococcus aureus
38.0% 11.6% 3.4% 7.8% 3.5%
Solomkin J et al: Intra-abdominal infections. In: Schwartz SI, Shires GT, Spencer FC, et al: Principles of Surgery, 7th ed. New York: McGraw-Hill Book Co., 1999:1541-42.
Anaerobic organisms
Bacteroides fragilis other Bacteroides Clostridia spp Prevotella spp Peptostreptococcus spp Fusobacterium spp Eubacterium spp Others
34.5% 71.0% 29.2% 12.0% 16.7% 8.6%
16.5% 19.4%
Incidence of various bacteria in 702 patients with intra-abdominal infections

PathogenesisWeinstein, Onderdonk et al. JID 1975;132:282-286
• Animal models mimic clinical condition– Gelatin capsules with rat feces implanted in peritoneal
cavity of rat– Early peritonitis: 37% mortality– Late abscesses in survivors: 100% incidence
• Antimicrobial Probes– Gentamicin: acute mortality 4%; abscess in 98% of
survivors– Clindamycin: acute mortality 35%; abscess in 5% of
survivors – Combination: 7% mortality;6% abscess

Magnitude of ProblemBarie et al. Surg Infect 2004;5(4):365-73
• 465 patients 1991-2002 Major NYC Hosp– Viscus perforation– Peritonitis (78%) or abscess (22%)– Community acquired 72%, Hospital Acquired
28%
• 74% organ dysfunction
• 23% mortality

Which Patients Require Therapeutic Administration of ABX?
• Considered prophylactic and given <=24 hours– Bowel injuries that are repaired within 12
hours– Acute perforation of stomach, duodenum and
proximal jejunum in absence of antacid therapy or malignancy (is there anyone not on Protonix®?)
– Acute appendicitis without gangrene, perforation, abscess or peritonitis

Require ABX?
• Acute cholecystitis often not infected– If infection strongly suspected
• Empiric therapy directed against enteric GNR– Not necessary to cover enterococcus– Not necessary to cover anaerobes unless biliary-bowel
anastamosis
• Infected pancreatic necrosis = colonic flora– Prophylactic antibiotics for non infected
pancreatic necrosis are “controversial” (i.e., GI vs ID)

Identification of High Risk Patients (who need broader spectrum Rx)
• High risk of death/complications– High APACHE II score– Poor nutritional state– Significant cardiovascular disease– Inability to obtain source control– Immunosuppressive therapy or condition
• Certain acute and chronic diseases– e.,g, acute leukemia, dialysis
– Prolonged preop hospital stay– Prolonged preop (>2 days) antimicrobials

Duration of Therapy
• Until resolution of clinical signs– Normal temp and WBC (?CRP)– Return of GI tract function
• If persisting clinical evidence of infection at 5-7 days– Sono/CT
• If diagnostic, obtain source control by draining and continue ABX and modify based on abscess culture
• If negative for abscess, consider D/C ABX

When are Cultures Indicated?
• Uncomplicated, perforated or gangrenous appendix without abscess: no impact on outcome when cultures obtained
• Abscesses, peri-colonic infections: failure rates higher if empiric ABX don’t cover aerobic flora
• Community epidemiology differs• Anaerobic susceptibility:
– Unnecessary if predictably potent coverage with metronidazole, carbapenems, beta lactam inhibitors used
• Resistance a concern with clindamycin, cefamycins, piperacillin alone, most quinolones
– Indicated if persisting anaerobic isolates, bacteremias or prolonged therapy indicated

Health Care Associated (HCA) Infections (Nosocomial)
• Infections occurring after initial surgery are HCA and may harbor resistant flora
• If empiric therapy does not include coverage against subsequently recovered resistant flora, morbidity higher
• Often require empiric combination therapy– To cover MRSA, (VRE), MDR GNR

Complicated IA Infections Infecting Flora by Onset Location• Community-acquired infections
• Enteric GNB, facultative bacilli, and β-lactam-susceptible GPC, obligate anaerobic bacilli (distal small-bowel and colon-derived infections and for more proximal perforations when obstruction is present)
– E coli, B fragilis
• Healthcare-associated infections (post-op/nosocomial)
• Prolonged pre-op LOS or > 2 days pre-op antibiotics
• Usually more resistant flora
– Pseudomonas, Enterobacter and Proteus spp, MRSA, Enterococci, and Candida spp
• Knowledge of local susceptibility patterns critical
Solomkin J et al. IDSA Guidelines Clin Infect Dis. 2003 Oct 15;37(8):997-1005.
GNB=gram-negative bacilliGPC=gram-positive cocciLOS=length of stay

What Should be Cultured?
• Blood cultures often no benefit in community acquired IAI (CA-IAI)
• Intra-abdominal specimens– Should be representative of the process– Rarely need more than one or two– Should always be sent for anaerobic as well
as routine• Anaerobic transport system• SWABS ARE NEVER APPROPRIATE

When Should Gram Stain be Done?
• CA-IAI: not indicated
• HCA-IAI: indicated to help guide empiric coverage– If GPC clusters seen, cover for MRSA

Indication for Anti-fungal Rx
• Candida species isolated in 20% of acute perforations of GI tract
• Anti-fungal therapy not indicated in most except:– Recent immunosuppressive therapy– Postop or recurrent IAI
• Choice of therapy– C albicans – fluconzole– Non albicans – caspofungin, voriconazole, AMB

Indications for Enterococcal Coverage
• Not indicated for enterococci as part of mixed flora in CA-IAI– Numerous comparative trials have shown no
benefit from covering enterococcus
• Indicated in– HCA-IAI– Pure culture of enterococci– Bacteremia with enterococci

Antimicrobial Regimens
• IDSA Practice Guidelines 2003
• Newer regimens– Tigecycline CID 2006– Moxifloxacin (FDA) 2005

Recommended Regimens: 2003 IDSA cIAI Guidelines
Adapted from Solomkin J et al. IDSA Guidelines. Clin Infect Dis. 2003 Oct 15;37(8):997-1005.
Mild-to-moderate Infections
High-severity Infections
Single agent regimen• Ampicillin/sulbactama
• Ticarcillin/clavulanic acid• Ertapenem
• Piperacillin/tazobactam• Imipenem/cilastatin• Meropenem
Combination regimen• Cefazolin or cefuroxime +
metronidazole• Fluoroquinolone (FQ)-
based therapy + metronidazole
• Cefotaxime, ceftriaxone, ceftizoxime, ceftazidime, cefepime + metronidazole
• Aztreonam + metronidazole• FQ + metronidazole
a

StudyMoxifloxacin IV/PO vs. Piperacillin/Tazobactam (PIP/TZO) IV Amoxicillin/Clavulanate (AMOX/CLA) PO
DesignProspective, randomized, multi-center, multinational, double-blind, active control, Phase III trials in patients with complicated intra-abdominal infection (cIAI)
ComparatorMoxifloxacin 400 mg sequential IV/PO versus PIP/TAZ 3.375 gm IV q6h AMOX/CL 800/114 mg PO q12h
Location [years]
71 centers: in the US (62), Canada (7) and Israel (2); [2000-2003]
Definition
cIAI
Requiring operative procedure or percutaneous drainage. Purulence/ exudate, inflamed or necrotic tissue confirmed at time of surgery.
Treatment 5-14 days
10 OutcomeClinical response at test-of-cure (TOC) (-10%) 25-50 after entry into the study
Moxifloxacin Study Design
Data on File, Schering Corporation. Study #100272.Malangoni M et al. ICAAC 2004. Washington DC. Abstract #L-990.

Moxifloxacin Study in cIAIPatient Populations (N=681)
PopulationMoxifloxacin
IV/POn (%)
PIP/TAZ IV AMOX/CL PO
n (%)
Randomized 339 342
Safety 329 (97%) 327 (96%)
Efficacy Valid 183 (54%) 196 (57%)
Microbiologically Evaluable Patients (MBE)
150 (44%) 163 (48%)
Data on File, Schering Corporation. Study #100272.Malangoni M et al. ICAAC 2004. Washington DC. Abstract #L-990.

79.878.2
50
55
60
65
70
75
80
85
Moxifloxacin Study in cIAIClinical Response (TOC)†
Clin
ica
l Re
sp
on
se
(T
OC
) (%
Pa
tien
ts)
n=153/196 n=146/183
Moxifloxacin IV/PO PIP/TZO IV AMOX/CLA PO
p=NS; 95% Confidence Interval (‑7.6, 9.2)
Efficacy-valid population
†Primary endpointMalangoni M et al. ICAAC 2004. Washington DC. Abstract #L-990.

78.0 77.3
0
10
20
30
40
50
60
70
80
90
100
Microbiologic response includes eradication and presumed eradication at TOC in the MBE population (N=313)
Bac
teri
olo
gic
al R
esp
on
seat
TO
C (
% P
atie
nts
)
p=NS; 95% Confidence Interval (-9.9%, 8.7%).
Moxifloxacin IV/PO
117/150 126/163n =
PIP/TZO IV AMOX/CLA PO
Data on File, Schering Corporation. Study #100272.Malangoni M et al. ICAAC 2004. Washington DC. Abstract #L-990.
Moxifloxacin IV/PO
PIP/TZO IV AMOX/CLA PO
Moxifloxacin Study in cIAI Bacteriological Response

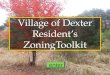
77.0
85.4
76.772
0
10
20
30
40
50
60
70
80
90
Moxifloxacin Study in cIAIMicrobiologic Success
Mic
ro S
ucc
ess
(TO
C)
(% P
atie
nts
)
69/9067/87 36/5035/41
E coli B fragilis
Microbiologic success includes eradication and presumed eradication at TOC in the MBE population (N=313)
n =
Data on File, Schering Corporation. Study #100272.Malangoni M et al. ICAAC 2004. Washington DC. Abstract #L-990.
Moxifloxacin IV/PO
PIP/TZO IV AMOX/CLA PO
p=NS

Adverse EventMoxifloxacin
(N=329)n (%)
PIP/TZO IV AMOX/CLA PO
(N=327)n (%)
Any treatment-emergent adverse event (AE)
276 (83.9) 271 (82.9)
Died 6 (1.8) 7 (2.1)
Serious AE 63 (19.1) 66 (20.2)
Premature discontinuation due to AE 34 (10.3) 28 (8.6)
Any drug-related adverse AE (≥2%) 82 (24.9) 90 (27.5)
Diarrhea 16 (5) 26 (8)
Nausea 16 (5) 13 (4)
Gamma glutamyl transferase increase
8 (2) 5 (2)
Data on File, Schering Corporation. Study #100272.Malangoni M et al. ICAAC 2004. Washington DC. Abstract #L-990.Safety Population
Moxifloxacin Study in cIAI Overall Safety Profile

Tigecycline for Complicated IAI
• Pooled date from 2 phase 3 studies comparing Tigecycline to Imipenem-cilastatin in 1642 adults




Caveats on Newer Regimens
• Moxifloxacin– Anaerobic resistance to FQ may emerge– Limited experience– Nothing published yet
• Tigecycline– Nausea/vomiting limiting factor in our
experience – Literature: 44%

2003 IDSA cIAI Guidelines
Overall Antimicrobial Management • Fluid resuscitation required prior to initiating antibiotic to
restore adequate visceral perfusion and ensure drug distribution
• Empirical coverage initiated upon suspicion of cIAI• Duration of therapy should be continued until resolution of
clinical signs of infection:– Afebrile– Normalization of WBC count– Return of gastrointestinal function
• If infection persists beyond 5-7 days:
– Diagnostic investigation required (CT or ultrasound) and/or additional intervention for source control
– Ensure treatment regimen provides appropriate coverage
Solomkin J et al. IDSA Guidelines Clin Infect Dis. 2003 Oct 15;37(8):997-1005.

Bibliography
• Babinchak T, Ellis-Grosse E et al. The Efficacy and Safety of Tigecycline for the Treatment of Complicated Intra-Abdominal Infections: Analysis of Pooled Clinical Trial Data. Clin Inf Dis 2005;41 (Suppl 5):S354-67
• Barie PS, Hydo LJ, Eachempati. Longitudinal Outcomes of Intra-Abdominal Infection Complicated by Critical Illness. Surg Infect 2004;5(4):365-73
• Goldstein EJC. Intra-Abdominal Anaerobic Infections. Clin Inf Dis 2002;35(Suppl ):S106-11

Bibliography
• Schering-Plough Company Data on File (personal communication)
• Solomkin JS, Mazuski JE, Baron EJ et al. Guidelines for the Selection of Anti-Infective Agents for Complicated Intra-abdominal Infections. Clin Infect Dis 2003;37:997-1005 Access on ID Society.org. Practice Guidelines
• Weinstein WM, Onderdonk AB, Bartlett JG, Louie TJ, Gorbach SL. Antimicrobial therapy of experimental intraabdominal sepsis. J Infect Dis 1975;132:282-6