-
7/28/2019 Interview Psychosomatic
1/10
Cardiovascular Reactivity of Patients WithEssential and Renal
Hypertension inan Emotion-Triggering InterviewHans-Christian Deter,
M D; Angela Blecher, M D; Cora S. Weber, MD
Blood pressure reactivity to mental stress in hyperten.sives is
much higher thanin nornwtensives. The authors'aim in this study was
to examine whether dif-ferent cardiovascular responses can he
induced hy various stimuli in hyper-tensive subgroups. The authors
matched 10 essential hypertensives (EHs), 10renal hypertensives (RH
s). and 10 normotensives (Ns) according to age andgender, examined
them during an emotion-stimulating interx'iew. and mea-sured blood
pressure (B P) and heart rate (HR) during the pha.ses ofthe
inter-view. They observed differences in BP reactivity between
EHs/RHs and Nsunder some stimuli hut not between EHs and RHs. as
well as a marked dif-ference in the product of systolic BP (SBP)
and H R between both hypertensivegroups in the anger/rage phase fp
= .028) and the baseline 2 (p = .02). Thisshows a higher
cardiovascular activation under mental stress and a iowerrecovery
in EHs and more sensitivity to perturbation or higher central
tensioncompared with RHs.Index Terms: cardiovascular reactivity,
emotion, essential hypertension,interview, renal hypertension
Essential hypertension (EH) has received much attentionfor many
years. Genetic and environmental aspects play amajor role in this
context.''^ Menial and psychophysiologi-cal reactivity may both
contribute to the development ofEH.'''^ Results from psychosomatic
studies have empha-sized tbe role of cardiovascular reactivity to
mental stressand the social environment as a possible stressor as
well ascertain personality traits'' that may have a
particularlystrong influence on the stress experience.^
Substantiatedrisk factors for EH seem to be an increased reactivity
tomental stress and a positive family history of EH comparedwith
tbose without tbis genetic component.** Psychosomaticfindings bave
repeatedly indicated open or latent personali-
Drs D eter. Blecher. an d Weber are with fhe Department
ofPsycho-samalic Medicine ami Psychnlherapy. Chariite U
niversiidtsmedi-zin. Bfrlin. Germ any.Copyright 2007 H eldref
Publications
ty traits, such as increased aggression, anger, and bostili-ty'
iR and have sug gested that these traits are associated
withincreased cardiovascular reactivity during mental
stress.Researchers in various studies""'^ have demonstratedthat
certain emotions trigger blood pressure (BP) reactions.Addressing
this issue in tbe present study, we aimed to ana-lyze (I) wbetber
emotions, such as aggression and anger,represent a specific stress
stimulus for essential hyperten-sives (EHs), as assumed
earlier'*''*''' and (2) whether theseemotions are generally
observed c irculation-activating trig-
gers that occur with the same intensity in normotensives(Ns) and
subjects with otber types of hypertension and aretherefore not
specific in tbe etiopathogenesis of EH.'*Psychological tests to
identify anger traits or bostilitygroups can be done using
standardized questionnaires."''Tbese examinations can also be
performed under laborato-ry conditions by inducing anger and
frustration or by stim-ulating emotions via specific interviewing
tecbniques. such
117
-
7/28/2019 Interview Psychosomatic
2/10
PATIENTS' CARDIOVASCULAR REACTIVITY
as tbe anger-recall technique.'^ Tbe interviewing techniquebas a
long tradition'''-" but bad fallen into some disputebecause of
unethical arrangements; bowever, this emotion-triggering technique
has been revived in recent yearsbecause it is far superior to other
tecbniques witb regard tothe level of beart rate and BP
reactions.-'
This technique has become establisbed in the testing of 1or 2
emotions-^ but bas thus far not been able to cover thewhole range
of several emotional responses, because it isdifficult to provoke
tbem validly in a sbort time. Zander etal'*^ had attempted tbis in
a structured interview and foundinteresting specific reaction
patterns tbat seemed to confirman emotional reaction specificity in
EHs. Stemmler's^^ lab-oratory findings concerning reaction
specificity also indi-cate an emotional reaction specificity. An
earlier studyreported that, in contrast to psychosomatic inpatients
andcontrols. EHs had stronger BP reactions in a structuredinterview
w itb emotional exposure to rage and anger as w ellas to questions
concerning their occupational situation.^
The question was whether this applies to all hypertensivesor
only to the specific group of patients witb EH. We want-ed to make
a more precise analysis of the disease-reactivefactors of
hypertension by comparing EHs. in whicb envi-ronmental factors are
repeatedly held responsible for tbedevelopment of tbe disease, with
renal hypertensives (RHs),in whom BP increases bave a clearly
somatic (ie. nepbro-genic) cause. We speculated that tbis would
enable us to dif-ferentiate between factors of reactivity to
varying stimulideveloping from tbe high-pressure disease itself and
otberetiopatbological factors caused by tbe social environment
orpersonality. Our aim in tbis study was to examine
whetherdifferent affects would induce different cardiovascular
reac-tions in EHs and RHs during an emotion-stimulating inter-view.
In accordance with earlier psycbosomatic literature.^'''we expected
that EHs would bave (I) stronger BP reactionsthan RHs and
normotensive (N) controls to the rage andanger affect (HI), (2)
stronger reactions in a psycbosocialsituation triggering negative
emotions (H2). and (3) strongerreactions to thoughts about tbeir
occupational situation (H3).In a descriptive analysis, we wanted to
exam ine if emotionssucb as anxiety, envy, and grief were effective
in triggeringa bigber cardiovascular reaction in EHs.METHODS
SubjectsWe conducted tbis study in the Departments of
Psycboso-matic Medicine and Nephrology at tbe Charite
CampusBenjamin Franklin. Universitatsmedizin Berlin.
Tbe study included hypertensive and N patients aged 20to 60
years; wbo bad a good command of the German lan-
guage; and had no neurological or psychiatric diseases,
car-diovascular diseases, otber independent severe organic
dis-eases, or alcohol or drug abu.se.We recruited the RHs from the
nephrology consultationservice with the following diagnoses;
fibromuscular renalarterial steno sis {n = 2) and polycystic kidney
disease (n = 8)We selected 10 age- and sex-matcbed EHs from 18 EHs
oftbe bypertension clinic at our hospital. We matched 10 of 22Ns
for age and sex recruited through intemal blackboardnotices to be
included in this study.We obtained tbe internal examination data
from tbepatients' medical records, from consultation with the
fami-ly pbysician, and from anamnestic questionnaires filled outby
all patients.The 3 groups consisted of 3 x 7 men and 3 x 3
womenwitb no significant differences between groups regardingage.
body mass index (BMI), and occupational status (Table
1) or smoking and sports activities. Compared witb the RHgroup,
tbe EH group reported stronger subjective stressreactions, more
frequent occupational activities, and longerdurations of
hypertension. RHs smoked more frequently,participated in more
sports, and possessed more family his-tories of cardiovascular
diseases than did tbe EHs. Meanserum creatinine and target organ
damage were comparablebetween EHs and RHs.None of tbe patients had
taken any medication 24 hoursbefore the test. Seven in eacb hy
pertensive group took anti-bypertensive drugs before tbe test,
wbich were: EH group calcium antagonists (4), diuretics (2). and
ACE (angioten-
sion converting enzyme) inhibitors (5) and RHgroupcalcium
antagonists (6), diuretics (2), and ACEinhibitors (2). A Ionger
interruption of drug administrationwould have been ethically
unjustifiable. Thus, we per-formed tbe study despite
antihypertensive tberapy becausethe 2 groups received comparable
medication, witb tbeexception of ACE inhibitors. It was not
expected tbat reac-tions to the provoked affects would be
systematically dis-torted by possible side effects of the
drugs.Study DesignAfter filling out psycbological questionnaires,
we per-formed a first baseline and a standardized mental
stressexamination (results not reported here). After a
15-minuteresting period and measurement of initial baseline
values,we subjected patients to a structured .'iO-minute
interviewtbat addressed the following areas in a random order:
com-plaints, occupational situation, life situation in which
angerand rage were experienced, partnership, life situation inwhicb
anxiety was experienced , life situation in wbicb envywas
experienced, life situation in which grief was experi-
118 Behavioral Medicine
-
7/28/2019 Interview Psychosomatic
3/10
DETER. BLECHER. & WEBER
enced, life situation with a strong feeling of well-being,
andthe most important negative affect triggered by a
stressfulpsycbosocial situation. Tbe second resting period,
duration3 minutes, started after tbe end of the interview.
HCD. an experienced scientist and physician trained indepth
psychology, conducted tbe interview, recorded it onsound carrier,
and transcribed it. We tben blinded the tran-scripts (without
knowledge of the physiological data). Tworaters, members of tbe
research group, independently defmedtbe 9 sections in the
transcripts and we discussed and coordi-nated the differences. We
subsequently assessed the individ-ual sections of the transcripts
witb respect to BP and HR.Measuring InstrumentsDuring the
interview, we recorded HRs using a bipolarextremity lead in a
.standard electrocardiogram (ECG). Wemeasured BP at 1-minute
intervals using an automaticallyinflatable cuff placed over tbe
bracbial artery of tbe left arm.We recorded BP witb Bosomat 11
(Boscb and Son. Jungingen.Germany, wbicb were validated and used in
former studies');we recorded the ECG with an amplifier (Scbwarz:
Munich.Germany) on registration paper and with an electronic
evalu-ation program (Par Electronics: Berlin, Germany).Statistical
MethodsBecause of the low sample size in this first pilot study
inwhich we examined cardiovascular reactivity in EH andRH, we did
not apply multivariate testing but insteadfocused on tbe bypotbesis
derived from tbe literature.
We calculated tbe BP differences between tbe 3 groupswith tbe H
test (Kruskal-Wallis test) for tbe tbree samples.We caicuiated the
differences in mm Hg between baseline
systolic BP (SBP) and diastolic BP (DBP) and SBP andDBP in tbe
individual phases of tbe interview. We recordedBP as well as HR and
tbe product of HR and SBP We cal-culated tbe differences between 2
unrelated samples withMann-Whitney's V test. Tbe significance level
was p < .05for the 3 hypotheses and, as adjustment for multiple
com-parisons (Bonferroni), p< .02 for tbe 3 fields of tbe
descrip-tive analysis and p < .01 for the other variables.
RESULTSEH compared witb RH had higher initial SBP, but
compa-rable DBP before the experiment (difference not
signifi-cant). We obtained these initial baseline values. Baseline
1SBP: EH = 156.5; RH = 143.9; N = 125.6; DBP: EH =103.3; RH = 98.3;
N = 84.9 mm Hg, (Table 1), prior to com-pleting tbe standardized
mental stress examination (data notreported bere). The BP values
did not return to this level intbe subsequent interview. Wben
starting tbe interview, BPlevels for EHs and RHs were not
statistically different,SBP: EHs = 165.5: RHs = 164.3; Ns = 129.9;
DBP: EHs =108.4; RHs = 110.2; Ns = 87.8 mm Hg. SBP and DBPincreased
strongly during the interview. The mean maximalSBP increase per
phase was 30.2 mm Hg for EHs, as bigbas 44.7 mm Hg for RHs, and
28.6 mm Hg in Ns (Table 2).DBP increased by 23.9 mm Hg in EHs. by
26.1 mm Hg inRHs. and by 19.0 mm Hg in Ns. Tbe intragroup
comparisonof values in the interview situation and the initial
baselineyielded significant to highly significant values for all
groupsin each interview pbase.
As we had assumed, there were no statistically signifi-cant
differences in SBP and DBP behavior between RHsand EHs witb respect
to anger/rage (HI), psychosocial sit-
TABLE 1. General Patient Characteristics
CharacteristicAg eBody Mass IndexSexMale
FemaleOccupationWorkerEmployee/civil
servantUnemployed/student/reiiree
Essentialhypertensives
{n = 10)n M SD
44.8 9.725.9 2.6
73172
Renalhypertensionn
7305
(n = 10)M SD
41.6 9.824.6 3.5
Normotensivesn
73064
(n = 10)M SD
43.0 10.224.5 2.4
Vol 32. Winter 2 007 119
-
7/28/2019 Interview Psychosomatic
4/10
P A T I E N T S ' C A R D I O V A S C U L A R R E A C T I V I T
Y
TABLE 2. Blood Pressure in Essential(RHs), and Normotensives
Interview phase
Initial baselineStart of
interviewComplaintsOccupationAnger/ragePartnershipAnxietyEnvyGriefWell-beingStrong
negative emotionEnd baseline
initial baselineStart of
interviewComplaintsOccupationAnger/ragePartnershipAnxietyEnvyGriefWell-beingStrong
negative emotionEnd baseline
Initial baselineStart of
interviewComplaintsOccupationAnger/ragePartnershipAnxietyEnvyGriefWell-beingStrong
negative emotionEnd baselineNote. EUs: n = iO;RHs:n=]O;
Hypertensives (EHs), Renal H ypertensives(Ns) During the
Individual Phases of the Interview
EHsM
156.5165.6180.4180.6188.8180.2181.1184.5188.3183.4182.8174.6
103.3108.4119.4120.1127.0120.6120.8126.3128.1123.8125.6113.4
84.788.692.993.693.692.391.090.490.188.091.983.5
N s : n = 1 0 .
SDRH s
M SDNs
M
Systolic blood pressure (mm
Hg)20.527.224.117.822.718.817.827.923.325.619.616.2
143.9164.3173.5179.5182.7183.5183.9186.2184.2188.6184.0168.8
11.610.615.713.618.421.319.725.318.315.717.516.2
125.6129.9141.3150.8154.2154.4150.3149.0149.8151.9184.0140.9Dialostic
blood pre.ssure (mm
Hg)11.914.113.510.812.110.113.514.1n.o13.112.110.7
17.316.5U . I11.611.211.210.112.39.911.710.810.7
98.3110.2119.2121.3119.8123.5119.8119.8120.5125.4122.7110.2
11.614.510.511.813.313.810.814.516.419.015.510.9Heart rate
(bpm)
76.072.480.680.180.879,477.478.178.079.779.971.2
15.912.415.016.314.613.514.714.712.912.115.912.2
84.987.897.7101.4101.2104.8102.199.7103.3103.9102.992.9
72.872.774.175.975.275.274.876.476.973.374.869.8
SD
15.420.919.416.220.023.420.721.918.920.517.517.0
12.3II.311.512.312.612,211.710.78.815.39.18.9
12.210.713.313.612.712.712.210.814.711.912.811.5
uation tr igger ing negative emotions (H2) , and occupationals i
tuation (H3) . In these areas , mean reactions comparedwith
baseline I were higher in RHs than in EHs.
In contras t to our expectat ions , RHs had s tronger
SBPreactions than did EHs at the start of the interview {p =.046)
and in the situations that stimulate anxiety (p = .052)
120 Behavioral Medicine
-
7/28/2019 Interview Psychosomatic
5/10
D E T E R , B L E C H E R , & W E B E R
and well-being (p = .08), DBP reactivity did not differ
sig-nificuntly between the 3 groups; EHs reacted (as a
statistictendency) stronger than did Ns in the phase focusing
onfeelings of anger /rage. EHs versus Ns, p = .09] (Table 3).
EHs had the highest and RHs the second highest initialHR va lues
{Table 2). We found this suc cession in all inter-view phases
except the starting one. in which Ns had slight-ly higher values
than did RHs. As anticipated, EHs had thehighest values for
anger/rage and occupation but not for thepsychosocial s i tuation
tr igger ing negative emotions . Like-wis e , RHs had also the
strongest reaction (on a lower level)to anger/rage, whereas Ns had
the highest values for envyand grief. In all 3 groups, the HR
dropped below the initiallevel at the end of the interview, with
the least markeddecrease for EHs.
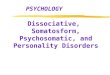
We also examined whether the product on SBP and HRinduced by the
items discussed in the interview (anger/rage,psychosocial s i
tuation tr igger ing negative emotions , andoccupation) w as s
tronger in EHs than i t was in RHs (Figure1) . Th e 3 sam ples
could be clearly differentiated by theabsolute values of this
variable. EHs had the highest initialand final values, which
clearly exceeded those of the other2 groups during the entire
interview. RH had higher initialand final values than did Ns in all
interview phases. In con-trast to Ns, EHs and RHs had clearly
increa.sed values in thecourse of the in terv iew and a s teep
decline thereaf ter . How-ever, the values in all 3 groups remained
above the initiallevel . We found s ignif icant d if ferences betwe
en the 3groups in all interview areas including initial and the
base-line after the interview. The differences between the 2
TABI.K 3, Systolic and D iastulic Blood Pressure
DifferencesHyperten.sives (RHs), and Normotensives (Ns;
Controls)
Interview phase
Start ai interviewComplaintsH3: OccupationH I:
Anger/ragePartnershipAnxietyEnvyGriefWell-beingH2 : Strong negative
emotionEnd baseline
Start (tf
interviewComplaintsOccupationAnger/ragePartnershipAnxietyEnvyGriefWell-beingStrong
negative emotionEnd baselineNole. NS = not significant.*Witcoxon's
rank sum test.
("M
4.615.725.228.627.124.724.324.226.326.2\5.:i
3.312.816.516.316.917.215.118.419.018.48.0
Ns= iO)SD
10.813,310.613.114.616.215.714.813.613.110.8
4. 77.67.28.99.79.25.78.69.010.46.9
(nM
to Initial Baseline in
EHs= 10)SD
Essential
RH s(n
M= 10)
SD
Hypertensivei
Ns/EHsp *
Systolic blood pressure differences (nun
Hg)9.123.925.328.524.824.628.430.229.226.318.1
12.512.615.418.015.114.717.815.517.013.914.7
14.429.635.638.839.640.042.340.344.739.924.9
8.98.06.89.812.612.120.018.513.313.78.8
NSNSNSNSNSNSNSNSNSNSNSDiastolic blood pressure differences (mm
Hg)5.717.520.521.920.418.4
21.923.020.522.29.8
4.56.910.25.66.38.73.22.86.14.35.9
6.919.621.420.622.920.221.322.326.121.610.4
6.88.08.39.49.27.99.012.611.812.312.2
NSNSNS.091NSNS.028NSNSNSNS
(KHs),
Ns/RHsp *
NS.028.019NSNS.041.066.046.019.085.083
NS.085NSNSNSNS.042NSNSNSNS
Renal
EHs/RHsp *
.046NSNSNS.080.052NSNS.080NSNS
NSNSNSNSNSNSNSNSNSNSNS
Vol 32, Winter 20 07 121
-
7/28/2019 Interview Psychosomatic
6/10
PATIENTS' CARDIOVASCULAR REACTIVITY
Essential hypertensivesRenal hypertensivesNomiotensives
16 -
6 14-12 -
10 -
^ Ititerview Phases -v"FIGURE 1. Medians of the product from
sy.stolic bloodpressure (SBP) and heart rate (HK) in the
individualinterview phases with essential hypertensives,
nor-motensives, and renal hypertensives.
hypertensive groups were highly significant in the
categoryanger/rage in terms of our expectations (p = .028) but
notfor the other prognosed categories (occupation and psy-chosocial
situation with negative emotions). The grief phase(p = .011) and
the second resting phase after the interview(p < .02) were also
different between the 2 hypertensivegroups (Table 4).C O M M E N
T
As anticipated, both hypertensive groups had stronger meanSBP
and DBP reactions to the stress interview than did theN controls.
The hypertensive groups differed in their initialSBP (EH > RH)
on the day of the experiment, but not in theprevious ciinical
examination. The BP differences becameles.s pronounced during the
interview. The varying initialconditions led to a maximal SBP
increase of 29.2 mm Hg inEHs and 44.7 mm Hg in RHs in the highest
phase (well-being). Thus, our resting values may have already
beenchanged by the behavior of EHs who had a higher level ofstress
anticipation accompanied by an increased HR thandid other groups.
This must be kept in mind when inter-
preting the calculations of differences between baselinevalue
and various values ofthe interview p hases. Interestingdifferences
between the hypertensive groups are the higherreaction values of
RHs at the start of the interview and dur-ing the phase in which
the test subjects had to recall an anx-iety situation; however,
these differences were not withinthe anticipated range with respect
to anger/rage, occupa-tion, and the negative emotion phase. C
omparing BP valueswithin groups, both Ns and tbe 2 hypertensive
groups hadsignificantly higher levels during the individual
interviewphases than at baseline.Analysis of HR showed that already
in the resting phase,EHs had 12 more beats/min than Ns had and 8
more
beats/min than RHs had. In the psychodiagnostic study ofthese
patients, we did not detect any differences betweenEHs and RHs in
anxiety and depression (Deter et a!). EHshad a total maximum
increase of 9 beats/min (occupation,anger phases) and RHs had a
maximum increase of 4beats/min (anger phases). Ns only had a m
aximum increaseof 4 beats/min (grief phase). Even though these
differencesare not significant, they demonstrate that EH s could be
acti-
122 Behavioral Medicine
-
7/28/2019 Interview Psychosomatic
7/10
DETER, BLECHER, & WEBER
TABLE 4. Differences Between Normotensivesand Renal
Hypertensives (RHs) inHeart Kate (HRl in the Individual the
Product(Ns), Essential Hypertensives (EHs),of Systolic Blood
Pressure (SBP) andPhases of the Interview (Absolute Values)
Ns/EHs/RHs*Interview phasesInitial baselineStart of
interviewComplaintsH3: OccupationH1 :
Anger/ragePartnershipAnxietyEnvyGriefH2 ; Strong negative
emotionEnd baseline
P
.018.040.004.007.011.018.003.002.(X)l.007
.001
Ns/EHstP
.006.018.007.007.011.018.005.011.011.007
.005
Ns/RHstP
.028.046.010.066.020.028.015.011.028.017
.015
EHs/RHstP
.085.079.068NS.028NS.066NS.011NS
.020Note. NS = nol significant. Tlie p values represent the
differences between groups product of SBP x HR.Friedman
test.tWilcoxon's test.
vated to a higher degree than could the other 2 groups.
ThisfiniJing can be statistically confirmed by the product of
SBPand HR. There were significant differences between EHsand RHs
with respect to the interview phases in which westimulated
anger/rage and grief. As anticipated, emotionalstimulation of
anger/rage produced cardiovascular activa-tion that was stronger in
EHs than il was in RHs and extend-ed beyond the interview period in
EHs but not in RHs.The findings obtained in the present study have
to be con-sidered in the light ofthe disproving of our initial
hypothe-ses (SBP and DBP reactivity to anger/rage provocation
isenhanced in EHs compiu-ed with RHs). Both RHs and nor-mal
controls have similar BP reactions as do E Hs to specif-ic
interpersonal conditions (feelings of anger/rage, experi-ence of
the occupational situation, and psychosocialsituations triggering
strong negative emotions). On the onehand, we were unable to
confirm our hypothesis formulatedin agreement with the specificity
hypothesis of Alexander^
and a number of other authors"''^^* that EHs react in a
spe-cific manner to defined emotional conditions or
con-flicts.-^-'' On the other hand, our study clearly confirmedthe
previously reported finding of increased cardiovasculartension
being more evident in EHs-^** than in RHs (measuredby the product
of SBP and HR).The findings in this pilot study that included RHs
in astress experiment also have to be carefully considered in
the
light of the relatively small number of test subjects. EHsand RH
s were representative for a clinical study populationwith
hypertensive grade I and II with comparable BP levelsin a clinical
examination. W e recruited the Ns from hospitalpersonnel without
any disease. We matched groups accord-ing to sex and age, but other
possibly influencing factorscouid not be evaluated.'" The main
hypotheses (reaginicresponse to recalled emotional topics) seemed
to be compa-rable between the 3 groups.The results may have been
influenced by antihyperten-sive drug intake some days before the
experiment. A lon gerinterruption of drug administration would have
been ethi-cally unjustifiable and was therefore not possible in the
2hypertensive groups; however, this possible effect may nothave
been very strong because the test subjects withoutmedication had
essentially the same subevaluation findingsas did those with
medication.The structured interview, in which we addressed
different
topics within 50 minutes, has to be critically examinedbecause
individual situations or emotional states may havebeen too strongly
related or not experienced intensivelyenough in the interview
situation.^' A provocation with 2 or3 emotional areas in the
experiment might have provided abetter control for these
conditions; however, this pilot studyaimed particularly at
determining whether the various possi-ble emotions and life
situations would yield different find-
Vol 32, Winter 2007 123
-
7/28/2019 Interview Psychosomatic
8/10
PATIENTS' CARDIOVASCULAR REACTIVITY
ings. Thus, it was very interesting that grief and
anxietyelicited, in part, the same strong BP reactions as
anger/rage.tt seemed to be a limiting factor to focus
hypertensionresearch only on the aggression-anger-hostility
complex,and the results confirm earlier studies relating EH to
theeffects of grief or anxiety. - After all, SBP reactions of upto
40 mm Hg per phase in RHs and maximal reactions of upto 60 mm Hg in
individual patients have demonstrated thatemotion-triggering
interviews have a considerably strongereffect than do standardized
stress situations, with clearlylower mean SBP reactions of 15-20 mm
Hg.-' A possiblesource of bias in the study could be the
interviewer, whoknew the diagnosis at the time of the interview.
The differ-ences observed between EHs and RHs indicate that high
BPalone is not responsible for all the reactions under stress
inthese patient populations. But the results presented here donot
confirm the specificity hypothesis'-" that certain emotionstrigger
higher BP reactions in EHs. The EHs evidenced non-specific
characteristics indicative of higher cardiovascularactivity"" and
perhaps higher neurogenic tension; however,we showed that social
environment and mental stress areimportant factors in both EHs and
RHs. There is evidencethat these are conditions for worsening of
the disease and fordeveloping EH-'*- " in the long run, in addition
to biologicalrisk factors,^' certain personality traits (eg, anger
or copingbehavior), and social mechanisms (eg, life events or
socialsupport' ). Further analyses in high-risk Ns and other
hyper-tensive groups are needed to gain a better understanding
ofthe etiopathogenesis and long-term outcome of EH.
NOTEFor comment or further information, please address
correspon-dence to H. C. Deter. MD. Department of Psychosomatic
Medi-cine and Psychotherapy. Charite Universitatsmedizin.
CampusBenjamin Franklin. Hindenburgdamm 30, 12200 Berlin,
Germany(e-mail: [email protected]).
REFERENCES1. Baxendale-Cox LM. Anoverview of essential
hypertension inAmericans as a multifactodal phenometion:
interaction ofbio-logic and environmental factors. Prog Cardiova.sc
Nurs.2(X)O;15(2):43-39.2. Pickering. TG. Th e effects of
environmental and lifestyle fac-tors on biood pressure and the
intermediary role of the sympa-thetic nervous system. J Hum
Hypertens. 1997;1 l(l):9-18.3. Deter HC , Klepper A. Schulte KH.
Preliminary resultsof a dif-ferentiated emotion-stimulating
interview in patients withessential hypertension as compared with
inpatients of a psy-chosomatic unit and normal controls. Fsychother
Psvchosom.1996;65(5):262-27I.4. Folkow B. Physiological aspects of
primary hypertension.PhysiolRev. 1982;62:347-503.
5. Julius S. Changing role of the autonomic nervous system
inhuman hypertension. J Hypertens. 1990;8:59-65.6. Jorgensen RS,
Johnson BT, Kolodzlej ME. Schreer GE. Ele-vated blood pressure and
personality: a meta-analytic review.Psydwl Bull.
l996:l20f2):293-320.7. Dimsdale JE. Pierce B, Schoenfeld D, Brown
A, Zusman R,Graham R. Suppressed anger and blood pressu re: the
effects ofrace, sex, social class, obesity, and age. Psvchosom
Med.1986:48:430-436.8. Frederikson M, Matthews K. Cardiovascular
responses tobehavioral stress and hypertension: a meta-analytic
review.Ann Behav Med. 1990; 12:30-39.9. Alexander F. Psvchosom Med.
New York: Grune and Stratton;
10. Linden W, Chambers W, Maurice J. Lenz J. Sex differences
insocial support, self deception , hostility and ambulatory
cardio-vascular activity. Heallh P.sychol. I993;13:376-380.11 . Lai
JY. Linden W. Gender, anger expression style, and oppor-
tunity for anger release determine cardiovascular reaction toand
recovery from anger provocation. Psxchosom Med.!992;54:297-310.12.
Christensen AJ, Smith TW. Cynical hostility and cardiovascu-lar
reactivity during self disclosure. Psychosom
Med.1993:55:193-202.13. Everson SA. Goldberg DE. Kaplan GA,
Julkunen J. SalonenJT. Anger expression and incident hypertension.
PsvchosomMed. 1998;60(6):730-735.14. Weiner H. Psychobiology and
Human Disease. New York;Elsevier: 1977.15. Zander W. Engel RR,
Kitscher M. Wiedemann G. Psy-chophysiologische
Korrelationsuntersuchungen wahrend eineshalbstandardisierten
Interviews hei Patienten mil Ulcus duo-
deni und Hyperwnie. In: Zander W. ed.
ExperimentelleForschungsergebnisse in der psychosomatischen
Medizin.Gbttingen, Germany: Vandenhoeck & Ruprecht;
1981;120-128.16. Noll G. Wenzel RR, Schneider M. et al. Increased
activation ofsympathetic nervous system and endothelin by mental
stress innormotensive offspring of hypertensive parents.
Circulation.1996:93(5):866-869.17. Haeri SL, Mills PJ, Nelesen RA.
el al. Acute psychologicstress reactivity in blacks versus whites:
relationship to psy-chologic characteristics. Blood P ress Monit.
1996; 1:27-32.18. Ironson G,Taylor CB, Boltwood M, et al. Effects
of anger onleft ventricular ejection fraction in coronary artery
disease. AmJCardiol. l992;7O:281-285.19. Wolf S. Wolff H. A summary
of experimental evidence rela-tion life stress to the pathogenesis
of emotional hypertensionin man. In: Bell E T. ed. Hypertension.
Minneapolis: Universi-ty of Minnesota Press, 1951.20 . Tlieorell T.
SchaiMng. D, Akerstedt T. Circulatory reactions incoronary patients
during interviewa noninvasive study. BiolPsychol. 1977;5:233-243.21
. Dimsdale JE, Stem MJ, Dillon E. The stress interview as a toolfor
examining physiological reactivity. Psychosom Med.
124 Behavioral Medicine
-
7/28/2019 Interview Psychosomatic
9/10
DETER, BLECHER, & WEBER
1988;50:64-71,22 . Svensson JC. Theorell T. Cardiovascular
effects of anxietyinduced by interviewing young hypertensive male
subjects. JP.syclwsom Res. 1982;26(3):359-370.23 . Stemmler G.
P.sychophysiologische Emotionsmuster: Ein
empirischer und methodologischer Beilrag zur intra-
undinteriindividuellen Begrimdbarkeii spezifischer Profile
beiAngst, Arger und Freude. Frankfurt. Germany: Lang; 1984.24 .
Jammer UD. Shapiro D. Hui KK. Oakley ME. Lovett M . Hos-tility and
differences between clinic, self-determined, andambulatory blood
pressure. Psychosom Med. 1993;55:203-211.25 . Miller SB.
Cardiovascular reactivity in anger-defensive indi-viduals: the
influence of task demands. Psycho.som Med.1993;55:78-85.26. Mann S
J, James G D. Defensiveness and essential hyp erten-sio n. 7
P.iyc/jtJ^owi Res. 1998;45(2):139-I48.27.Rutledge T, Linden W,
Davies R. Psychological response
styles and cardiovascular health: confound or independ
riski'actor? Health Psychol. 20 0 0 ;1 9 :4 4 1 ^5 L
28 . Amann FW. Bolli P. Buhler FR. Personality and
adrenergicfactors in essential hypertension. Contrib
Nephrol.1982:30:64-69.29 . Frederikson M. Psychophysiological
theories on sympatheticnervous system reactivity in the development
of essentialhypertension. Scand J Psychol. 1991;32:254-274.30 .
Dimsdale JE. Mills O. Dillon E. Does reactivity testing in
thelaboratory reflect blood pressure changes elsewhere? ./
Psy-chosom Res. 1992:36:701-705.31 . Deter HC. Buchholz K. Schorr
U. Schachinger H. Turan S,Shamia AM. Psychophysiologica! reactivity
of salt-sensitivenormolensive subjects. J Hyperten.w 1997; 15:
839-844.32 . Light K. Gindler S. Sherwood A, et al. High stress
responsiv-ity predicts later blood pressure only in combination
with pos-itive family history and high life stress.
Hypertension.I999;33:1458-1464.
Vol 32 , Winter 2007 125
-
7/28/2019 Interview Psychosomatic
10/10