Embed Size (px)
Citation preview

Interventions for Clients
with Fluid and Electrolyte imbalances

2

3
Body Fluid Compartments
• 2/3 (65%) of TBW is intracellular (ICF)
• 1/3 extracellular water– 25 % interstitial fluid (ISF)
– 5- 8 % in plasma (IVF intravascular fluid)
– 1- 2 % in transcellular fluids – CSF, intraocular fluids, serous membranes, and in GI, respiratory and urinary tracts (third space)

4

5

6
• Fluid compartments are separated by membranes that are freely permeable to water.
• Movement of fluids due to:– hydrostatic pressure
– osmotic pressure\
• Capillary filtration (hydrostatic) pressure
• Capillary colloid osmotic pressure
• Interstitial hydrostatic pressure
• Tissue colloid osmotic pressure

7

8
Balance• Fluid and electrolyte homeostasis is
maintained in the body
• Neutral balance: input = output
• Positive balance: input > output
• Negative balance: input < output

9

10

11
Solutes – dissolved particles• Electrolytes – charged particles
– Cations – positively charged ions
• Na+, K+ , Ca++, H+
– Anions – negatively charged ions
• Cl-, HCO3- , PO4
3-
• Non-electrolytes - Uncharged • Proteins, urea, glucose, O2, CO2

12

13
Regulation of body water• ADH – antidiuretic hormone + thirst
– Decreased amount of water in body– Increased amount of Na+ in the body– Increased blood osmolality– Decreased circulating blood volume
• Stimulate osmoreceptors in hypothalamusADH released from posterior pituitaryIncreased thirst

14

15
Result:increased water consumptionincreased water conservation
Increased water in body, increased volume and decreased Na+ concentration

Fluid Volume Excess
Occurs when the body retains both water and sodium in similar proportions to normal ECF. It is also called hypervolemia.
Common causes include:-- Excessive intake of sodium chloride- Administering sodium-containing infusions too rapidlyDisease processes that alter regulatory mechanisms such as heart failure, renal failure.

Edema Excess interstitial fluid.
Edema typically is most apparent in areas where the tissue pressure is low, such as around the eyes, and in dependent tissues (known as dependent edema), where hydrostatic capillary pressure is high.
Pitting edema: edema that leaves a small depression or pit after finger pressure is applied to the swollen area.



Electrolyte Imbalances

RISK FACTOR
Loss of sodium, as in:
Loss of GI .fluids
Use of diuretics
Gains of water, as in:
Excessive administration of
D5W
Water intoxication
Disease states associated with
SIADH (a form of
hyponatremia)
Pharmacologic agents that
may impair water excretion
Assessments
Anorexia
Nausea and vomiting
Lethargy
Confusion
Muscle cramps
Fingerprinting over sternum
Muscular twitching
Seizures
Coma
Serum Na below 135 mEq/L
Urine specific gravity <1.010
Nursing interventions-Monitor fluid losses and gains.-Monitor for presence of GI and CNS symptoms.- Monitor serum Na levels.- Check urine specific gravity.-If able to eat, encourage foods and fluids with high sodium content.-Be aware of sodium content of common-IV fluids.-Avoid giving large water supplements to-Patients receiving isotonic tube feedings.-Take seizure precautions when hyponatremia is severe
Hyponatremia

RISK FACTOR
Water deprivation
Increased sensible and
insensible water loss
Ingestion of large amount of
salt
Excessive parenteral
administration of sodium-
containing solutions
Profuse sweating
Diabetes insipidus
Assessments
Thirst
Elevated body temperature
Tongue dry and swollen,
sticky mucous Membranes
Severe hypernatremia
Disorientation
Hallucinations
Irritable and hyperactive
Focal or grand mal seizures
Coma
Serum Na above 145 mEq/L
Urine specific gravity
>1.015
Nursing interventions- Monitor fluid losses and gains.- Observe for excessive intake of high sodium foods.- Monitor for changes in behavior such as restlessness, lethargy, and disorientation.- Look for excessive thirst and elevated body temperature.- Monitor serum Na levels.- Check urine specific gravity.- Give sufficient water with tube feedings to Keep serum Na and BUN at normal limits.
Hypernatremia

RISK FACTORDiarrheaVomiting or gastric suctionPotassium-wasting diureticsPoor intake as in anorexia nervosa,alcoholism, potassium-freeparenteral .fluidsPolyuria
AssessmentsFatigueAnorexia, nausea, and vomitingMuscle weaknessDecreased bowel motilityCardiac arrhythmiasPolyuria, nocturia, dilute urinePostural hypotensionSerum K below 3.5 mEq/LECG changesT waves flattening and ST segment depression on ECG
Nursing interventions- Monitor for occurrence of Hypokalemia.- Prevent Hypokalemia by:- Encouraging extra K intake if possible- Educating about abuse of laxatives and diuretics-Administer oral K supplements if ordered.- Be knowledgeable about danger of IV potassium administration.
Hypokalemia

RISK FACTORDecreased potassium excretion:Oliguric renal failurePotassium-sparing diureticsHigh potassium intake, especiallyin presence of renal insufficiencyShift of potassium out of cells into the plasma(acidosis, tissue trauma, infection, burns)
AssessmentsVague muscle weaknessCardiac arrhythmiasParesthesias of face, tongue, feet, andhandsFlaccid muscle paralysisGI symptoms such as nausea, intermittent intestinal colic, or diarrhea may occurSerum K above 5.0 mEq/LPeaked T waves, widened QRS on ECG
Nursing interventionsMonitor for hyperkalemia, which is life threatening.Prevent hyperkalemia by:Following rules for safe administration of KAvoiding giving patients with renal insufficiency K-saving diuretics, K supplements,or salt substitutesCautioning about foods high in potassium content
Hyperkalemia


RISK FACTORSurgical hypoparathyroidismMalabsorption Vitamin D deficiencyAcute pancreatitisExcessive administration of citrated bloodAlkalotic states
AssessmentsTrousseau’s and Chvostek’s signsNumbness and tingling of fingers and toesMental changesSeizuresSpasm of laryngeal musclesECG changesCramps in muscles of extremitiesTotal serum calcium <8.5 mg/dL
Nursing interventionsTake seizure precautions when hypocalemia is severe.Monitor condition of airway.Take safety precautions if confusion is present.Educate people at risk for osteoporosis about need for dietary calcium intake.Discuss calcium-losing aspects of nicotine and alcohol use.
Hypocalcaemia

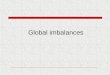
Hypocalcemia

Hypocalcemia

A positive Trousseau's signMuscular contraction including flexion of the wrist and metacarpophalangeal joints, hyperextension of the fingers and flexion of the thumb on the palm

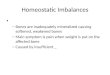
A positive Chvostek's sign.Twitching or contraction of the facial muscles produced by tapping on the facial nerve at specific point

RISK FACTORHyperparathyroidismMalignant neoplastic diseaseProlonged immobilizationLarge doses of vitamin DOveruse of calcium supplementsThiazide diuretics
AssessmentsMuscular weaknessTiredness, lethargy , ConstipationAnorexia, nausea, and vomitingDecreased memory and attention spanPolyuria and polydipsiaRenal stonesCardiac arrestSerum calcium >10.5 mg/dL
Nursing interventionsIncrease mobilization when feasible.Encourage sufficient oral intake.Discourage excessive consumption of milk products.Encourage bulk in the diet.Take safety precautions if confusion is presentBe alert for signs of digitalis toxicity in Hypercalcaemia patients.Force fluids to prevent formation of renal stones.
Hypercalcaemia

Hypercalcemia

Hypomagnesemia Signs/symptoms Causes