Embed Size (px)
Citation preview

Radiologic Management of Vertebral hemangiomas
I.-D. Laredo l , D. Reizine2, 1.-1. Merland2, and M. Bard l
Departments of 1 Bone and Joint Radiology and of 2 Neuroradiology and Therapeutic Angiography Hopital Lariboisiere, Paris, France
Vertebral hemangiomas (VH) include a range of clinical entities from the frequent, incidentally noted, asymptomatic lesion to the rare expansile tumor that may compress the spinal cord.
Asymptomatic vertebral hemangiomas (A VH)
AVH are very frequent. AVHs are seen at autopsy in 10-11 % of cases [8]. Only a small percentage of these A VHs are detected on plain radiographs. Incidental finding of A VH is more frequent at CT study. In most cases, A VH are located at the lumbar spine and thoraco-Iumbar junction. They usually have the characteristic vertically striated radiographic appearance described by Perman [12]. In addition, AVHs have the radiologic features of inactive (regular striations and normal cortex), localized (incomplete involvement of the vertebral body, normal neural arch and soft tissue) angiomatous dystrophy. Selective arteriography, when performed, shows few or no abnormal vessels. These radiologic features are different from those of VH responsible for cord compression [8] (Figs. 1-3).
Fig. 1. Asymptomatic VH of L 4 with regular sticated appearance. Note normal cortex and sparing of
the pedic1es
M. Bard et al. (eds.), Interventional Radiology in Bone and Joint© Springer-Verlag/Wien 1988

212 1.-D. Laredo etal.
Compressive vertebral hemangiomas (CVH)
Fig_ 2. AP tomogram of an asymptomatic VH ofL 2. Note incomplete involvement of the vertebral body, normal cortex and regular striation
Fig. 3. CT scan of an asymptomatic VH of L 1: note regular trabeculation, sparing of the neural arch and normal soft tissue. As usual in asymptomatic VH the cortex appears almost normal. The minute cortical discontinuity of the midposterior vertebral body corresponds to normal venous drain-
age of the vertebral body
CVH occur more rarely than AVHs. The 14 cases ofCVH that we previously reported were seen over a 20-year period through selective referrals [8]. The role of vascular radiologic procedures in the diagnosis and treatment of CVH is discussed below.
Symptomatic vertebral hemangiomas (SVH)
A radiographic image suggestive of VH is sometimes found in patients consulting for back pain. In these cases, careful radiologic evaluation as detailed below, may help to determine appropriate management.

Radiologic management of vertebral hemangiomas 213
eVH
Rare in the first decade oflife, eVH occurs at any age, with a peak frequency in the young adult. CVH preferentiaJly occurs in the thoracic spine. More specificaJly 72% to 93% [8] of cases are located from T-3 to T-9, that is, on seven thoracic vertebrae.
CVH outside the thoracic spine are rare. Only a few cases of cervical CVH are cited in the literature, and these are often cases of regional skeletal angiomatosis [8]. The lumbar and sacral spine are infrequently involved by CVH. CVH must be distinguished from extradural, foraminal, or paravertebral arteriovenous malformations, in which involvement of bone is secondary. In most cases, CVHs are responsible for slow, progressive compression of the spinal cord. Months or even years of back or nerve-root pain may precede spinal cord compression. Frequently, pain is absent, and sensory or motor deficiency, often of insidious onset, is the presenting complaint. As a result, the patient is frequently seen at a late stage of the condition. A unique form of onset is the development of paraplegia in women in their third trimester of pregnancy. In these cases, onset of impairment is often sudden and complete. The spontaneous evolution of neurologic signs is most often unfavorable but unpredictable, and partial or even complete remissions of varying duration have been reported [8]. Palpation of local tumefaction is rare and more suggestive of an adjacent angiomatosis in the soft tissue.
The radiographic appearance of CVH is usually characteristic of VH with a vertical striated appearance. However, the radiographic appearance of CVH can be misleading. In some cases, demineralization of the vertebral body and nonvisualization of the pedicles suggest metastasis [4]. In others, the dominant radiographic feature may be an expanded cortex [10] or a paravertebral soft-tissue swelling [10]. Even in those lesions with radiologic characteristics of VH in general, CVH shows additional features of active (irregular trabeculae with lytic zones, poorly defined and expanded cortex) and extensive (involvement of the entire vertebral body, neural arch and soft-tissue extensions) vascular tumors (Fig. 4 a--c) [8].
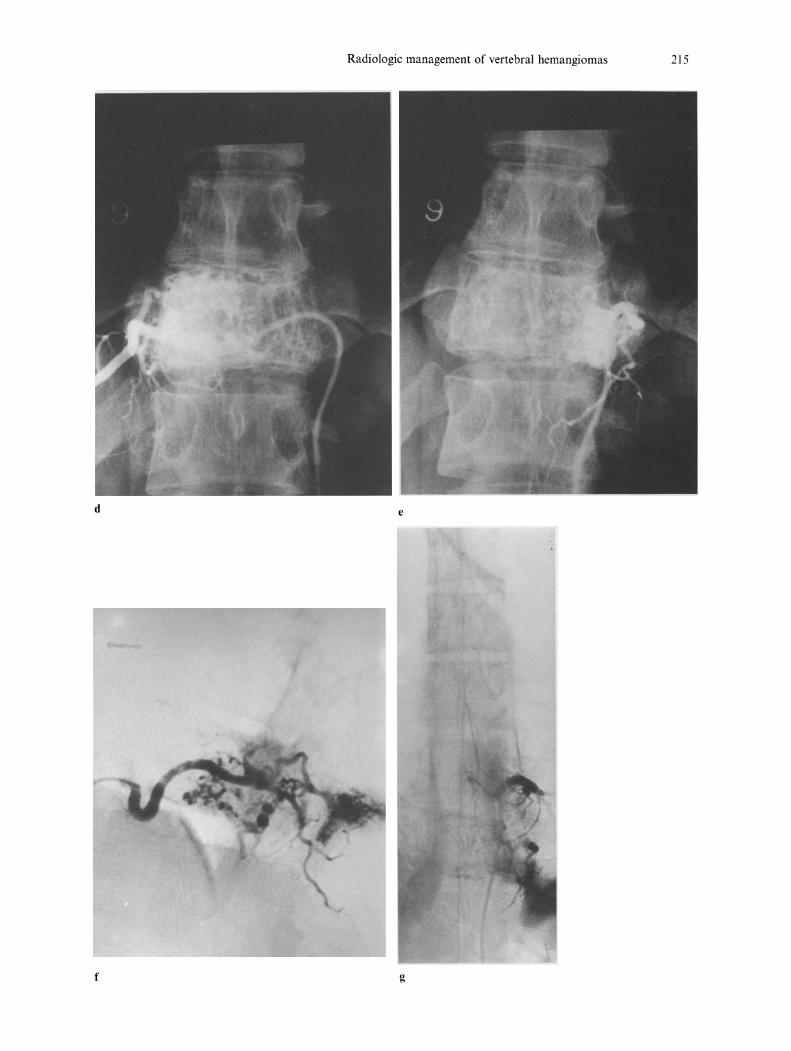
Selective arteriography of the spinal cord, first developed by Djindjian et al. [3], is an obligatory procedure in cases of CVH (Fig.4 d-g). The arteriographic appearance is usually characteristic: dilatation of arterioles of the vertebral body, multiple blood pools in the capillary phase, and, finally, intense opacification extending beyond the normal hemivertebral territory throughout the entire vertebral body. Opacification beyond normal cortical limits corresponds to extension of the angioma into the paravertebral soft tissues and the spinal canal (best seen on lateral radiographic views). The absence of early venous draining distinguishes CVH from high-flow arteriovenous malformations. The origin of the anterior spinal artery supplying the cord is visualized and can thus be avoided during embolization and/or the surgical approach. Embolization of one or more feeding arteries greatly reduces bleeding and facilitates surgery [1,9]. In the absence of preoperative embolization, bleeding during surgery may be extremely profuse. Surgical findings confirm that compression of the spinal cord is more often due to extradural extension of the angioma than to bone expansion.
The treatment of VH accompanied by neurologic signs has been much debated. Decompressive laminectomy is the usual treatment. Radiation therapy is sometimes recommended as an adjunct to decompressive laminectomy.

214 1.-D. Laredo et a!.
Others have proposed radiation therapy as the sole treatment for CVH [8] because of the high rate of surgical morbidity and failures. Current treatment of CVH associates preoperative embolization and decompressive laminectomy [1, 2, 7, 9]. Inert, non-resorbable particles are generally used. All feedings pedicles must be embolized with respect to the anterior spinal artery. In certain cases, embolization alone allowed complete and durable neurologic recovery. Hekster [6, 7] reported a case report concerning a patient with paraplegia due to spinal compression by a vertebral hemangioma which was treated in 1972 by embolization and radiotherapy [7]. Fifteen years later the patient was still in excellent condition and without motor impairment [6].
a
c
Fig. 4 a, b. Plain films of a compressive vertebral hemangioma. c CT of the same patient: irregular trabeculation, extension in the paravertebral soft tissue. d, e Angiography shows hypervascularisation. f Lateral view of the left 10th intercostal artery. g Anterior spinal artery arises from the left 9th intercostal artery: embolization can be
performed
Radiologic management of vertebral hemangiomas 215
d e
f g

216 J.-D. Laredo et al.
Clinical approach of SVH
Patients with VH in whom the only complaint is local pain (with no objective evidence of spinal cord compression) must be distinguished from those with asymptomatic and compressive VH. In these cases it is difficult to select adaquate management.
Since CVHs and A VHs have different radiographic and arteriographic features (Table 1), it has been stated that, in individual cases, the radiographic
Table 1. Radiologic signs of CVH versus A VH [8]
Signs
T-3 to T-9 location
Involvement of entire vertebral body
Involvement of neural arch (pedieles)
Irregular trabeculation
Expanded and poorly defined cortex
Soft tissue swelling
CVH (n = 14)
13
13
13
10
13
10
AVH (n = 11)
4
3
o I
o
Table 2. Management of VH using a scoring system (plain films and CT)
Signs
T-3 to T-9 location
2 Involvement of entire vertrebral body
3 Involvement of neural arch (pedieles)
4 Irregular trabeculation (lytic zone)
5 Expanded and poorly defined cortex
6 Soft tissue swelling
Final score
* Score 0-2 with or without local pain:
--+ Probable inactive VH
¢ Routine elinical and radiological follow-up
* Score 3 and/or nerve root pain:
--+ Possible aggressive VH
¢ Selective arteriography in specialized center
Score Value
Sign present
6
Sign absent
o
o
o
o
o o
o

Radiologic management of vertebral hemangiomas 217
appearance may help to evaluate the aggressiveness of a VR. In a previous paper [8], we postulated that those SVH with radiologic features of CVH may correspond to aggressive lesions while those those with the features of A VH are likely to be inactive. We have proposed a scoring system based on 6 radiologic criteria evaluated on plain films and CT (Table 2). This scoring system helps to place an individual lesion in the group of aggressive or inactive VH. For each criteria, one point in given if that feature is present and no points if it is absent. A score ranging from 0 to 6 is thus obtained for each lesion. With that scoring system, CVH have a score of 4 or more while A VH have a score of 2 or less [8]. Therefore, in the evaluation of an individual case of SVH, a score from 0 to 2 suggests inactive, localized, angiomatous dystrophy, necessitating only routine clinical and radiologic follow-up (Table 2). By contrast, a score of 3 or more and/or the presence of nerve-root pain in the territory of the lesion seen on the radiographs raises the possibility of an active VH and requires the use of selective arteriography followed by embolization of the feeding arteries if hypervascularization is noted. The score is also useful as an element of comparison for follow-up radiologic examinations.
References
1. Benati A, da Pian R, Mazza C et al (1974) Preoperative embolization of a vertebral haem angioma compressing the spinal cord. Neuroradiology 7: 181-183
2. Bouchez B, Gozet G, Lecoutour X, Kassiotis P, Arnott G, Delecour M (1984) Compression medullaire par angiome vertebral au cours de la grossesse: un cas traite par embolisation. Presse Med 13: 1696-1697
3. Djindjian R, Cophignon J, Merland J-J, Theron J, Houdard R (1973) Embolization in vertebro-medullary pathology. Neuroradiology 6: 132-142
4. Gaston A, Nguyen JP, Djindjian Metal (1985) Vertebral haemangioma: CT and arteriographic features in three cases. J Neuroradiol 12: 21-33
5. Gross CE, Hodge CHJ, Binet EF, KricheffH (1976) Relief of spinal block during embolization of a vertebral body hemangioma. J Neurosurg 45: 327-330
6. Hekster REM, Endtz LJ (1987) Spinal cord compression caused by vertebral hemangioma relieved by percutaneous catheter embolization 15 years later. Neuroradiology 29: 101
7. Hekster REM, Luyendijk N, Tan TI (1972) Spinal cord compression caused by vertebra hemangioma relieved by percutaneous catheter embolization. Neuroradiology 3: 160-164
8. Laredo JD, Reizine D, Bard M, Merland J-J (1987) Vertebral hemangioma, radiologic evaluation. Radiology 161: 186-189
9. Lepoire J, Montaut J, Picard L, Heppner H, Masingue M, Arnould G (1973) Embolisation prealable a l'exen':se d'un hemangiome du rachis dorsal. Neurochirurgie 19: 173-181
10. McAllister VL, Kendall BE, Bull JWD (1975) Symptomatic vertebral haemangiomas. Brain 98: 71-80
11. Mohan V, Gupta SK, Tuli SM, Sanyal B (1980) Symptomatic vertebral haemangiomas. Clin Radiol 31: 575-579
12. Perman F (1926) On hemangiomata in the spinal column. Acta Chir Scand 61: 91-105