Embed Size (px)
Citation preview

Interventional Interventional Pulmonology:Pulmonology:
Who Should Learn and Who Should Learn and How?How?
Michael S Machuzak, MDMichael S Machuzak, MDMedical Director, Center for Major Airway Medical Director, Center for Major Airway
DiseaseDiseaseTransplant InstituteTransplant Institute
StaffStaffRespiratory InstituteRespiratory Institute

No DisclosuresNo Disclosures
Consultant to:Consultant to: OlympusOlympus CareFusionCareFusion


BackgroundBackground Hospital of the University of PennsylvaniaHospital of the University of Pennsylvania
ResidencyResidency FellowshipFellowship
2 year IP Fellowship2 year IP Fellowship Daniel StermanDaniel Sterman
PENNPENN Ali MusaniAli Musani
National JewishNational Jewish Marseille, FranceMarseille, France
Herve Dutau et alHerve Dutau et al Chiba, JapanChiba, Japan
Kasu Yasufuku et alKasu Yasufuku et al
Cleveland ClinicCleveland Clinic 20062006
What is Interventional What is Interventional Pulmonology?Pulmonology?
Advanced Advanced Diagnostic Diagnostic BronchoscopyBronchoscopy
Airway ImagingAirway Imaging AutofluorescenceAutofluorescence Narrow-BandNarrow-Band Confocal Confocal
Nodule, Mass & Lymph Nodule, Mass & Lymph node biopsynode biopsy
CT fluoroCT fluoro Electromagnetic guidanceElectromagnetic guidance Virtual bronchoscopic Virtual bronchoscopic
navigationnavigation Endobronchial UltrasoundEndobronchial Ultrasound
Convex & RadialConvex & Radial
Therapeutic Therapeutic BronchoscopyBronchoscopy
Central Airway ObstructionCentral Airway Obstruction AblationAblation DilationDilation Stent placement Stent placement
Management of Lung Txp Management of Lung Txp airway complicationsairway complications
Endoscopic Emphysema Endoscopic Emphysema TreatmentTreatment
Treatment of FistulaTreatment of Fistula BPF, TE, BE, etc…BPF, TE, BE, etc…
Thermal Ablation for Thermal Ablation for AsthmaAsthma

What is Interventional What is Interventional Pulmonology?Pulmonology?
Pleural Disease & MorePleural Disease & More
Pleural Manometry and Ultrasound for Pleural Manometry and Ultrasound for Large Volume ThoracentesisLarge Volume Thoracentesis Thoracoscopy +/- PleurodesisThoracoscopy +/- Pleurodesis Tunneled catheter Tunneled catheter
Minimally Invasive Pleural InterventionMinimally Invasive Pleural Intervention Medical thoracoscopyMedical thoracoscopy Tunneled catheterTunneled catheter Pigtail catheter placementPigtail catheter placement
OtherOther Tracheostomy, PEG, Trans-Tracheal Oxygen CathetersTracheostomy, PEG, Trans-Tracheal Oxygen Catheters

What is Interventional What is Interventional Pulmonology?Pulmonology?
Evolving specialtyEvolving specialty >20 years>20 years Meld of many different specialtiesMeld of many different specialties
Pulmonary, ENT, Thoracic surgery, IR, Pulmonary, ENT, Thoracic surgery, IR, Oncology, etc…Oncology, etc…
Emphasis on multidisciplinary careEmphasis on multidisciplinary care New technologies & proceduresNew technologies & procedures Training???????Training???????
In developmentIn development

Why Learn a New Why Learn a New Procedure?Procedure?
Improve patient Improve patient carecare MaximizeMaximize
Diagnostic yieldDiagnostic yield Pt outcomesPt outcomes Revenue StreamRevenue Stream Multidisciplinary careMultidisciplinary care Independence Independence
MinimizeMinimize InvasivenessInvasiveness RiskRisk CostCost
OtherOther Lack of expertise Lack of expertise
locallylocally It’s funIt’s fun
??????
Reasons NOT to Reasons NOT to Learn a New Learn a New ProcedureProcedure Never learned the old wayNever learned the old way
Advanced technology does Advanced technology does NOT NOT improve improve basic skillsbasic skills
It seems coolIt seems cool Need volume to obtain/maintain Need volume to obtain/maintain
competencycompetency Too costlyToo costly

How to Learn New How to Learn New ProceduresProcedures
Read the literature Read the literature Really???Really???
Standard trainingStandard training PCCM fellowshipsPCCM fellowships
CoursesCourses Single or multiple Single or multiple
dayday Mini-fellowshipsMini-fellowships
Weeks - monthsWeeks - months Dedicated year Dedicated year
of IP trainingof IP training
Web-based Web-based curriculumcurriculum
Supervised Supervised simulator sessionssimulator sessions

Short courses / “Mini-Short courses / “Mini-fellowships”fellowships”
Excellent exposure to one/variety of Excellent exposure to one/variety of techniquestechniques
DidacticsDidactics Hands-onHands-on
Simulators Simulators High vs. Low fidelity modelsHigh vs. Low fidelity models
Animal modelsAnimal models PatientsPatients
Apprenticeship Apprenticeship
Middle AgesMiddle Ages InternshipsInternships FellowshipsFellowships Post-gradPost-grad
Benefits:Benefits: Structured approachStructured approach AccountabilityAccountability
Mentee AND mentorMentee AND mentor
Need:Need: StructureStructure CurriculumCurriculum Defined outcome measuresDefined outcome measures TimeTime
Web-Based EducationWeb-Based Education
www.bronchoscopy.orgwww.bronchoscopy.org


Bronchoscopy SimulatorsBronchoscopy Simulators Multi-center prospective cohort study using BSMulti-center prospective cohort study using BS
Differentiate b/t expert & noviceDifferentiate b/t expert & novice Does use of BS improve rate of skill acquisition?Does use of BS improve rate of skill acquisition?
““Experts" (> 500, n = 9)Experts" (> 500, n = 9) ““Intermediates" (25 to 500, n = 8)Intermediates" (25 to 500, n = 8) ““Novices" (none, n = 11)Novices" (none, n = 11)
2 BS cases with performance measures 2 BS cases with performance measures recordedrecorded
Distinguishing performance measures identifiedDistinguishing performance measures identified Used to evaluate the learning curve for new fellowsUsed to evaluate the learning curve for new fellows
RCT comparing quality of bronch performanceRCT comparing quality of bronch performance New pulmonary fellowsNew pulmonary fellows
Conventional methodsConventional methods SimulatorSimulator
Am. J. Respir. Crit. Care Med., Volume 164, Number 12, December 2001, 2248-2255

Bronchoscopy SimulatorsBronchoscopy Simulators
Experts > Intermediates > NovicesExperts > Intermediates > Novices Procedure timeProcedure time % of segments visualized% of segments visualized Time in red-outTime in red-out Wall collisionsWall collisions
New fellowsNew fellows After 20 simulations After 20 simulations Improved Improved
SpeedSpeed % segments visualized% segments visualized Time in red-outTime in red-out CollisionsCollisions
Am. J. Respir. Crit. Care Med., Volume 164, Number 12, December 2001, 2248-2255

Bronchoscopy SimulatorsBronchoscopy Simulators
BS Fellows > Conventional fellowsBS Fellows > Conventional fellows First actual bronchoscopiesFirst actual bronchoscopies
Procedure time Procedure time 815 vs. 1,168 s815 vs. 1,168 s
p = 0.001p = 0.001 Bronch nurse subjective quality assessment Bronch nurse subjective quality assessment
scorescore 7.7 ± 0.3 vs. 3.7 ± 2.57.7 ± 0.3 vs. 3.7 ± 2.5
p = 0.05p = 0.05 Quantitative bronch quality scoreQuantitative bronch quality score
% segments correctly identified/procedure time% segments correctly identified/procedure time 0.119 ± 0.015 vs. 0.046 ± 0340.119 ± 0.015 vs. 0.046 ± 034
p = 0.03p = 0.03
Am. J. Respir. Crit. Care Med., Volume 164, Number 12, December 2001, 2248-2255

Bronchoscopy SimulatorsBronchoscopy Simulators
BS able to assess experience levelBS able to assess experience level Training new fellows on BS Training new fellows on BS
More rapid acquisition of expertiseMore rapid acquisition of expertise Compared with conventional training Compared with conventional training
methodsmethods
Technology has potentialTechnology has potential Facilitate bronch trainingFacilitate bronch training Improve objective evaluations of bronch Improve objective evaluations of bronch
skillsskills
Am. J. Respir. Crit. Care Med., Volume 164, Number 12, December 2001, 2248-2255

Interventional Pulmonology Interventional Pulmonology ≠ interventional ≠ interventional
pulmonologypulmonology Is a dedicated 1 year fellowship Is a dedicated 1 year fellowship
necessary for comprehensive training in necessary for comprehensive training in IP?IP? Establish basis for structured training in IP Establish basis for structured training in IP Distinct from standard PCCM trainingDistinct from standard PCCM training Structure to allow successful acquisition of Structure to allow successful acquisition of
skill set & experienceskill set & experience Specific skill sets may NOT require yearSpecific skill sets may NOT require year
EBUSEBUS Navigational bronchoscopyNavigational bronchoscopy Thermoplasty etc.Thermoplasty etc.

www.aabronchology.orgwww.aabronchology.org
““AABIP was founded in 1992 with the primary AABIP was founded in 1992 with the primary goal to foster excellence in Bronchology and goal to foster excellence in Bronchology and other Interventional Pulmonology related areas”other Interventional Pulmonology related areas”
““The cornerstone of our mission is to enhance The cornerstone of our mission is to enhance multidisciplinary and international collaboration multidisciplinary and international collaboration in our quest to develop, evaluate, and in our quest to develop, evaluate, and disseminate techniques, procedures, and cases”disseminate techniques, procedures, and cases”

Training: What is Training: What is Happening?Happening? > 50%> 50% pulmonologists pulmonologists
Inadequate training in “advanced diagnostic Inadequate training in “advanced diagnostic techniques such as TBNA”techniques such as TBNA”
> 70%> 70% practicing bronchoscopists practicing bronchoscopists Perform <100 bronchoscopies/yrPerform <100 bronchoscopies/yr
70%70% felt additional training should be felt additional training should be providedprovided ONLY to those interested in developing specific ONLY to those interested in developing specific
skillsskills
ONLY 25%ONLY 25% of pulmonologists perform all of pulmonologists perform all procedures required for board certificationprocedures required for board certification
Colt et al, Journal of Bronchology. 2000;7:8 Pastis et al, Chest 2005; 127: 1614

Advanced Training during Advanced Training during Standard FellowshipStandard Fellowship
Survey 122 PCCM fellowship directorsSurvey 122 PCCM fellowship directors Response 77%Response 77%
Wide variation in procedures offeredWide variation in procedures offered Presence of an IPPresence of an IP
Increased likelihood of advanced procedural trainingIncreased likelihood of advanced procedural training Brachytherapy (p < 0.05)Brachytherapy (p < 0.05) Electrocautery/argon plasma coagulation (p < 0.001)Electrocautery/argon plasma coagulation (p < 0.001) Stents (p < 0.001)Stents (p < 0.001) Laser therapy (p < 0.01)Laser therapy (p < 0.01) Rigid bronchoscopy (p < 0.001)Rigid bronchoscopy (p < 0.001) Cryotherapy (p < 0.05)Cryotherapy (p < 0.05)
For For only 3 of the 17 proceduresonly 3 of the 17 procedures did > 50% of did > 50% of the programs reach the targeted numbers to the programs reach the targeted numbers to obtain competencyobtain competency
Pastis et al, Chest 2005; 127: 1614 Colt et al, Journal of Bronchology. 2000;7:8

Goals of TrainingGoals of Training
Understand:Understand: Appropriate evaluation & management of Appropriate evaluation & management of
disease processdisease process Technical aspects of the procedureTechnical aspects of the procedure
Recognize pathologyRecognize pathology Distinguish from normalDistinguish from normal
Perform:Perform: Correct procedure expeditiouslyCorrect procedure expeditiously Communicate effectivelyCommunicate effectively
Ensure competent support staffEnsure competent support staff Avoid, recognize and treat complicationsAvoid, recognize and treat complications Know when NOT to do the procedureKnow when NOT to do the procedure
What is Competence?What is Competence?
Institute for International Medical Institute for International Medical EducationEducation ““Possession of a satisfactory level of Possession of a satisfactory level of
relevant knowledge and acquisition relevant knowledge and acquisition of a range of relevant skills that of a range of relevant skills that include interpersonal and technical include interpersonal and technical components…necessary to perform components…necessary to perform the tasks that reflect the scope of the tasks that reflect the scope of professional practices”professional practices”

What is Competence?What is Competence?
““Competence may differ Competence may differ from "performance", from "performance", which denotes actions which denotes actions taken in a real life taken in a real life situationsituation
Competence is therefore Competence is therefore not the same as not the same as "knowing" on the "knowing" on the contrary, contrary, it may well be it may well be about recognizing one's about recognizing one's own limits”own limits”

Is Competence Related to Is Competence Related to Repetition?Repetition?
Repetition allows for repeat trainingRepetition allows for repeat training Improves dexterityImproves dexterity Improves infrastructureImproves infrastructure
Makes systems function smoothlyMakes systems function smoothly Makes introduction of systems to avoid Makes introduction of systems to avoid
mistakes worthwhilemistakes worthwhile Improves success & decreases error!Improves success & decreases error!

Volume Thresholds:Volume Thresholds:No Correct AnswerNo Correct Answer
Too highToo high Many excludedMany excluded
Low dissemination of useful technologiesLow dissemination of useful technologies Missed opportunitiesMissed opportunities
Too lowToo low ComplicationsComplications Inappropriate utilization patternsInappropriate utilization patterns
We NEED to directly measure & monitor outcomes & We NEED to directly measure & monitor outcomes & performance qualityperformance quality Feedback to physicians rather than:Feedback to physicians rather than:
Expert opinionExpert opinion Volume requirementsVolume requirements Other surrogate markersOther surrogate markers
System combined with volume rqts & other didactic System combined with volume rqts & other didactic instrumentsinstruments
One of the greatest challenges:One of the greatest challenges: Necessary procedural quality benchmarks do not existNecessary procedural quality benchmarks do not exist
Registry data, collected by the ACCP, may be able to Registry data, collected by the ACCP, may be able to address this in the futureaddress this in the future AcQuire AcQuire Chest 2010(137)
More is Better: Numbers More is Better: Numbers MatterMatter
(NO data to support otherwise)(NO data to support otherwise) Drivers educationDrivers education PilotsPilots SurgerySurgery
esophagealesophageal cardiaccardiac endocrineendocrine airwayairway vascularvascular
ERCP: 200ERCP: 200 Central lines: 50Central lines: 50
Not completely Not completely dependent on #sdependent on #s
Birkmeyer NEJM 2002Jowell Endoscopy 1999Sznajder Arch Intern Med 1986

Vascular ProceduresVascular Procedures
High-volume providersHigh-volume providers Significantly better outcomesSignificantly better outcomes Elective Elective ANDAND emergent setting emergent setting
Subspecialty trainingSubspecialty training Considerable impactConsiderable impact Morbidity and mortalityMorbidity and mortality
Evidence for specialization of vascular Evidence for specialization of vascular servicesservices Performed by high-volume, specialty Performed by high-volume, specialty
trained providerstrained providers
J Vasc Surg 2007 Mar;45(3):615-26.
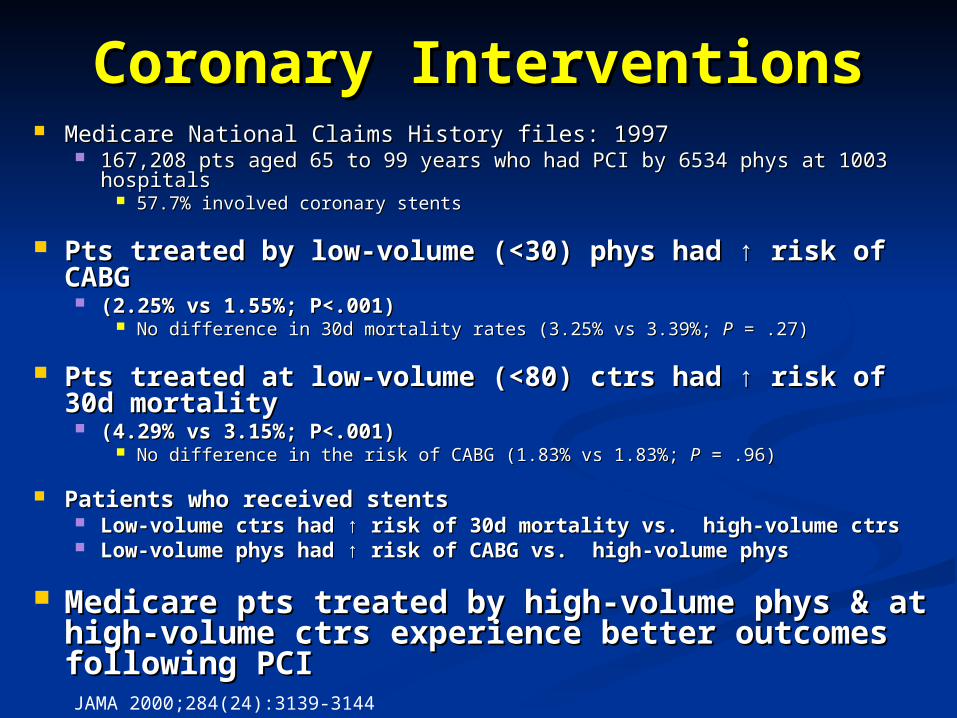
Coronary InterventionsCoronary Interventions Medicare National Claims History files: 1997Medicare National Claims History files: 1997
167,208 pts aged 65 to 99 years who had PCI by 6534 phys at 1003 hospitals167,208 pts aged 65 to 99 years who had PCI by 6534 phys at 1003 hospitals 57.7% involved coronary stents57.7% involved coronary stents
Pts treated by low-volume (<30) phys had ↑ risk of Pts treated by low-volume (<30) phys had ↑ risk of CABGCABG (2.25% vs 1.55%; P<.001)(2.25% vs 1.55%; P<.001)
No difference in 30d mortality rates (3.25% vs 3.39%; No difference in 30d mortality rates (3.25% vs 3.39%; PP = .27) = .27)
Pts treated at low-volume (<80) ctrs had ↑ risk of 30d Pts treated at low-volume (<80) ctrs had ↑ risk of 30d mortalitymortality (4.29% vs 3.15%; P<.001)(4.29% vs 3.15%; P<.001)
No difference in the risk of CABG (1.83% vs 1.83%; No difference in the risk of CABG (1.83% vs 1.83%; PP = .96) = .96)
Patients who received stentsPatients who received stents Low-volume ctrs had ↑ risk of 30d mortality vs. high-volume ctrsLow-volume ctrs had ↑ risk of 30d mortality vs. high-volume ctrs Low-volume phys had ↑ risk of CABG vs. high-volume physLow-volume phys had ↑ risk of CABG vs. high-volume phys
Medicare pts treated by high-volume phys & at Medicare pts treated by high-volume phys & at high-volume ctrs experience better outcomes high-volume ctrs experience better outcomes following PCIfollowing PCIJAMA 2000;284(24):3139-3144

Surgical OncologySurgical Oncology Retrospective cohort study using Surveillance, Epidemiology & Retrospective cohort study using Surveillance, Epidemiology &
End Results (SEER)End Results (SEER) 5013 pts in SEER registry 65 or > at cancer diagnosis 1984-19935013 pts in SEER registry 65 or > at cancer diagnosis 1984-1993 30 D mortality in relation to procedure volume, adjusted for co-30 D mortality in relation to procedure volume, adjusted for co-
morbidity, pt age, & cancer stage morbidity, pt age, & cancer stage Higher volume linked with lower mortalityHigher volume linked with lower mortality
Pancreatectomy (Pancreatectomy (PP=.004)=.004) Esophagectomy (Esophagectomy (PP<.001)<.001) Liver resection (Liver resection (PP=.04)=.04) Pelvic exenteration (Pelvic exenteration (PP=.04)=.04)
Not for:Not for: Pneumonectomy (Pneumonectomy (PP=.32)=.32) EsophagectomyEsophagectomy PancreatectomyPancreatectomy
When complex surgical oncologic When complex surgical oncologic procedures provided by surgical teams in procedures provided by surgical teams in hospitals w/ specialty expertise, mortality hospitals w/ specialty expertise, mortality rates are lowerrates are lowerJAMA 1998; 280(2): 1747-1751

Surgeon Volume & Surgeon Volume & MortalityMortality
National Medicare claims data base for 1998-National Medicare claims data base for 1998-19991999 Mortality among 474,108 patientsMortality among 474,108 patients 1 of 8 cardiovascular procedures or cancer resections1 of 8 cardiovascular procedures or cancer resections
Surgeon volume inversely related to Surgeon volume inversely related to operative mortality for alloperative mortality for all
(P=0.003 for lung resection, P<0.001 for all other procedures)(P=0.003 for lung resection, P<0.001 for all other procedures)
For many proceduresFor many procedures Observed associations b/t hospital volume & operative mortalityObserved associations b/t hospital volume & operative mortality Largely mediated by surgeon volumeLargely mediated by surgeon volume
Patients can improve their chances of Patients can improve their chances of survivalsurvival Even at high-volume hospitalsEven at high-volume hospitals
Surgeons who perform operations frequentlySurgeons who perform operations frequentlyNEJM 2003 349(22):2117-27

Teaching Procedural Teaching Procedural SkillsSkills
Medical Procedure ServiceMedical Procedure Service See one, do one, teach oneSee one, do one, teach one
Often:Often: See one done wrong, do one wrong, teach one wrongSee one done wrong, do one wrong, teach one wrong
Simulation training with 2w rotationSimulation training with 2w rotation
Central lines / Thora’s supervised by IP staffCentral lines / Thora’s supervised by IP staff LPs / Para’s supervised by hospitalist staffLPs / Para’s supervised by hospitalist staff
Decreased complications, improved confidenceDecreased complications, improved confidence
Smith et al, Sim Healthc 2010; 5:146 Huang et al, Acad Med 2009; 8:1127 Huang et al, Acad Med 2006; 119:e17

ACCPACCP ERS/ATSERS/ATS
Rigid Bronchoscopy Rigid Bronchoscopy 2020
Endobronchial Ultrasound Guided Endobronchial Ultrasound Guided TBNATBNA
5050 4040
Laser Laser
1515 2020
ElectrocauteryElectrocautery 1515 1010
Argon Plasma Coagulation Argon Plasma Coagulation
1515 1010
Cryotherapy Cryotherapy
1010
Airway stentsAirway stents 2020 1010
Tunneled pleural catheterTunneled pleural catheter 1515
Medical thoracoscopyMedical thoracoscopy 2020
Percutaneous dilational tracheotomyPercutaneous dilational tracheotomy 2020 5-105-10
Ernst et al, Chest 2003Bolliger et al, ERJ 2002
Number achievement alone does not establish competencyNumber achievement alone does not establish competency
Endoluminal therapies may be combined to achieve the Endoluminal therapies may be combined to achieve the recommended numberrecommended number
The list is representative & not all-inclusiveThe list is representative & not all-inclusive
Procedural Procedural RecommendationsRecommendations

Skill MaintenanceSkill Maintenance
Continued performance is Continued performance is requiredrequired Preservation of learned materialPreservation of learned material
CME is integral to medical CME is integral to medical practicepractice State licensure, ABIM, BLS/ ACLS etc.State licensure, ABIM, BLS/ ACLS etc.
No reason to think it is different No reason to think it is different for proceduresfor procedures
CredentialingCredentialing
Local hospital functionLocal hospital function NO national standardNO national standard
Regulated by bylawsRegulated by bylaws
May include proctoringMay include proctoring
Goal is improved patient careGoal is improved patient care
Should include ongoing quality Should include ongoing quality controlcontrol

Lessons from our Lessons from our ColleaguesColleagues ABIM Subspecialty boardsABIM Subspecialty boards
Interventional Cardiology & Interventional Cardiology & ElectrophysiologyElectrophysiology Additional 12m over the standard 3 yearsAdditional 12m over the standard 3 years
Society of American Gastrointestinal and Society of American Gastrointestinal and Endoscopic Surgeons (SAGES)Endoscopic Surgeons (SAGES) ““short courses…do not constitute sufficient short courses…do not constitute sufficient
training”training”http://www.sages.org/sg_pub16.htmlGuidelines for Training in Diagnostic and Therapeutic Endoscopic Retrograde Cholangiopancreatography (ERCP)Training Guidelines published on: 10/2006 by the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES)

Stepping ForwardStepping Forward
“… “… AABIP is a leading provider of AABIP is a leading provider of Interventional Pulmonary Interventional Pulmonary fellowships… The AABIP is pleased to fellowships… The AABIP is pleased to announce that Interventional announce that Interventional Pulmonology will participate in the Pulmonology will participate in the NRMP match starting this year as a NRMP match starting this year as a new fellowship match for the 2012 new fellowship match for the 2012 appointment year”appointment year”

IP Training: The Future is IP Training: The Future is NowNow
Outline an approach to IP training Outline an approach to IP training Principles & objectives of IP trainingPrinciples & objectives of IP training Disease specific knowledge base requirementsDisease specific knowledge base requirements Suggestions for:Suggestions for:
Curricula developmentCurricula development Responsibilities of IP program directorsResponsibilities of IP program directors
Lamb, Feller-Kopman et al, CHEST 2010; 137:195

Developing IP TrainingDeveloping IP Training
Specific recommendationsSpecific recommendations Uniform IP fellowship programUniform IP fellowship program
Clarifying the expectationsClarifying the expectations Skills and knowledge baseSkills and knowledge base
Accomplished during the training periodAccomplished during the training period Dedicated IP programsDedicated IP programs
1 year of additional training1 year of additional training
Not intended to excludeNot intended to exclude Select proceduresSelect procedures Properly trained pulmonologistsProperly trained pulmonologists Specialists from other disciplinesSpecialists from other disciplines
Benefits of Dedicated IP Benefits of Dedicated IP TrainingTraining
Increase # of physicians trained at Increase # of physicians trained at ‘higher standard’‘higher standard’ ImprovedImproved
Patient outcomesPatient outcomes ResearchResearch
Case series Case series Outcomes data Outcomes data Define best practiceDefine best practice TranslationalTranslational
ReimbursementReimbursement

Structure of IP Training Structure of IP Training ProgramProgram
Occur in context of defined training Occur in context of defined training programprogram Existing ACGME-accredited PCCM programExisting ACGME-accredited PCCM program Independent program directed by those with Independent program directed by those with
formal IP trainingformal IP training Given multidisciplinary nature of IPGiven multidisciplinary nature of IP
Essential that institutions have:Essential that institutions have: Departments of internal medicineDepartments of internal medicine
SpecialtiesSpecialties Radiology/interventional radiologyRadiology/interventional radiology PathologyPathology Thoracic surgeryThoracic surgery OtolaryngologyOtolaryngology Radiation oncologyRadiation oncology Medical oncologyMedical oncology Lamb, Feller-Kopman et al, CHEST
2010; 137:195

Training in Advanced Training in Advanced ProceduresProcedures
Pursued ONLY if there is realistic expectation Pursued ONLY if there is realistic expectation trainee will achieve sufficient proficiencytrainee will achieve sufficient proficiency Perform w/o supervision at completion of trainingPerform w/o supervision at completion of training Maintain skill setMaintain skill set
Brief exposure not adequate to achieve Brief exposure not adequate to achieve competencycompetency Standard PCCM or thoracic fellowship programsStandard PCCM or thoracic fellowship programs Training coursesTraining courses
Designated training programsDesignated training programs Offer full complement of technologies & clinical Offer full complement of technologies & clinical
applicationsapplications IndependentlyIndependently Collaboration with other disciplines in their institutionsCollaboration with other disciplines in their institutions
Other interventional pulmonary training programsOther interventional pulmonary training programs

Goals of IP Training Goals of IP Training ProgramProgram
Evaluate & manage patientsEvaluate & manage patients Complex airwaysComplex airways Thoracic & pleural diseaseThoracic & pleural disease
Recommend most appropriate diagnostic &/or Recommend most appropriate diagnostic &/or therapeutic proceduretherapeutic procedure
Understanding of indications, Understanding of indications, contraindications & additional diagnostic & contraindications & additional diagnostic & therapeutic alternativestherapeutic alternatives Context of safety & timelinessContext of safety & timeliness
Demonstrate ability to obtain accurate & Demonstrate ability to obtain accurate & thorough pre-procedure assessmentthorough pre-procedure assessment Identification of specific risk factors for procedureIdentification of specific risk factors for procedure
Demonstrate ability to minimize & manage Demonstrate ability to minimize & manage anticipated & unanticipated complicationsanticipated & unanticipated complications

Goals of IP Training Goals of IP Training ProgramProgram
Accurately identify, describe & communicate pertinent Accurately identify, describe & communicate pertinent procedural findingsprocedural findings
Recognize limitationsRecognize limitations SelfSelf Particular specialty or institutionParticular specialty or institution Appropriately refer patients to providers w/ required equipment & Appropriately refer patients to providers w/ required equipment &
skill setskill set
Demonstrate personal skills:Demonstrate personal skills: Obtaining informed consentObtaining informed consent Advanced directivesAdvanced directives Medical ethicsMedical ethics Communication to patients, families & referring physiciansCommunication to patients, families & referring physicians
Develop understanding of required equipmentDevelop understanding of required equipment Maintenance & technical troubleshootingMaintenance & technical troubleshooting
Contribute to & critically evaluate the scientific literatureContribute to & critically evaluate the scientific literature
Demonstrate the responsible use of resourcesDemonstrate the responsible use of resources Diagnostic testingDiagnostic testing Therapeutic interventionsTherapeutic interventions

Goals of IP Training Goals of IP Training ProgramProgram
Obtain skills to develop & direct sustainable IP Obtain skills to develop & direct sustainable IP programprogram
Maintain & review outcomes & compare with Maintain & review outcomes & compare with benchmarksbenchmarks Maintain the highest possible quality of careMaintain the highest possible quality of care
Complete training:Complete training: 2 primary advanced diagnostic techniques2 primary advanced diagnostic techniques
Endobronchial ultrasoundEndobronchial ultrasound Threshold numbers with appropriate supervisionThreshold numbers with appropriate supervision
Minimum of 2 ablative techniquesMinimum of 2 ablative techniques in therapeutic mgt of in therapeutic mgt of airwayairway
Use of BOTH silicone & metallic airway stentsUse of BOTH silicone & metallic airway stents PlacementPlacement RemovalRemoval Management of complicationsManagement of complications

Responsibilities of IP Responsibilities of IP Training ProgramTraining Program
Expert IP as training program directorExpert IP as training program director
Structured, multidisciplinary didactic Structured, multidisciplinary didactic curriculumcurriculum
Hands-on teachingHands-on teaching Appropriate mentoring and supervisionAppropriate mentoring and supervision Simulation training when applicable Simulation training when applicable
Monitor & record acquisition of Monitor & record acquisition of appropriate technical & cognitive appropriate technical & cognitive skillsskills

Responsibilities of IP Responsibilities of IP Training ProgramTraining Program
Review trainee's procedural logReview trainee's procedural log All proceduresAll procedures Indications, complications & outcomes of interventionIndications, complications & outcomes of intervention
Established performance standardsEstablished performance standards
Review & update the program’sReview & update the program’s Training methodologyTraining methodology Quality of trainingQuality of training
Peer-reviewed/medical society guidelinesPeer-reviewed/medical society guidelines
Conduct semiannual reviewsConduct semiannual reviews 360° fashion360° fashion
Trainee and faculty giving & receiving formal feedbackTrainee and faculty giving & receiving formal feedback
Document active researchDocument active research
Demonstrate CME in IPDemonstrate CME in IP

Between Between Infectious Infectious Diseases & Diseases & Nephrology!Nephrology!
www.nrmp.org

Remaining QuestionsRemaining Questions
Need to show that IP training achieves Need to show that IP training achieves goalsgoals VolumeVolume Patient outcomesPatient outcomes Higher qualityHigher quality
ResearchResearch GrantsGrants PublicationsPublications
How further spread of dedicated IP How further spread of dedicated IP training programs will impact standard training programs will impact standard PCCM fellowship trainingPCCM fellowship training

REFERENCES:REFERENCES:11 Ernst A, Silvestri GA, Johnstone D, American College of Chest Physicians : Interventional pulmonary procedures: Ernst A, Silvestri GA, Johnstone D, American College of Chest Physicians : Interventional pulmonary procedures:
guidelines from the American College of Chest Physicians. guidelines from the American College of Chest Physicians. ChestChest 123. (5): 1693-1717.2003 123. (5): 1693-1717.2003
22 Bolliger CT, Mathur PN, Beamis JF, European Respiratory Society/American Thoracic Society , et al: ERS/ATS Bolliger CT, Mathur PN, Beamis JF, European Respiratory Society/American Thoracic Society , et al: ERS/ATS statement on interventional pulmonology. statement on interventional pulmonology. Eur Respir JEur Respir J 19. (2): 356-373.2002 19. (2): 356-373.2002
33 Pastis NJ, Nietert PJ, Silvestri GA, American College of Chest Physicians Interventional Chest/Diagnostic Procedures Pastis NJ, Nietert PJ, Silvestri GA, American College of Chest Physicians Interventional Chest/Diagnostic Procedures Network Steering Committee : Variation in training for interventional pulmonary procedures among US Network Steering Committee : Variation in training for interventional pulmonary procedures among US pulmonary/critical care fellowships: a survey of fellowship directors. pulmonary/critical care fellowships: a survey of fellowship directors. ChestChest 127. (5): 1614-1621.2005 127. (5): 1614-1621.2005
44 Killeen SD, Andrews EJ, Redmond HP, Fulton GJ: Provider volume and outcomes for abdominal aortic aneurysm Killeen SD, Andrews EJ, Redmond HP, Fulton GJ: Provider volume and outcomes for abdominal aortic aneurysm repair, carotid endarterectomy, and lower extremity revascularization procedures. repair, carotid endarterectomy, and lower extremity revascularization procedures. J Vasc SurgJ Vasc Surg 45. (3): 615- 45. (3): 615-626.2007626.2007
55 McGrath PD, Wennberg DE, Dickens , Jr , JrJD, et al: Relation between operator and hospital volume and outcomes McGrath PD, Wennberg DE, Dickens , Jr , JrJD, et al: Relation between operator and hospital volume and outcomes following percutaneous coronary interventions in the era of the coronary stent. following percutaneous coronary interventions in the era of the coronary stent. JAMAJAMA 284. (24): 3139-3144.2000 284. (24): 3139-3144.2000
66 Begg CB, Cramer LD, Hoskins WJ, Brennan MF: Impact of hospital volume on operative mortality for major cancer Begg CB, Cramer LD, Hoskins WJ, Brennan MF: Impact of hospital volume on operative mortality for major cancer surgery. surgery. JAMAJAMA 280. (20): 1747-1751.1998 280. (20): 1747-1751.1998
77 Birkmeyer JD, Stukel TA, Siewers AE, Goodney PP, Wennberg DE, Lucas FL: Surgeon volume and operative mortality Birkmeyer JD, Stukel TA, Siewers AE, Goodney PP, Wennberg DE, Lucas FL: Surgeon volume and operative mortality in the United States. in the United States. N Engl J MedN Engl J Med 349. (22): 2117-2127.2003 349. (22): 2117-2127.2003
88 American Board of Internal Medicine : American Board of Internal Medicine : Internal medicine and subspecialty policiesInternal medicine and subspecialty policies. Accessed March, 18, . Accessed March, 18, 2008 http://www.abim.org/certification/policies/imss.aspx 2008 http://www.abim.org/certification/policies/imss.aspx
99 Society of American Gastrointestinal Endoscopic Surgeons : Society of American Gastrointestinal Endoscopic Surgeons : Guidelines for training in diagnostic and therapeutic Guidelines for training in diagnostic and therapeutic endoscopic retrograde cholangiopancreatographyendoscopic retrograde cholangiopancreatography. Accessed March 18, . Accessed March 18, 2008 http://www.sages.org/sagespublications/guidelines/guidelines.php 2008 http://www.sages.org/sagespublications/guidelines/guidelines.php
1010 Jowell PS: Endoscopic retrograde cholangiopancreatography: toward a better understanding of competence. Jowell PS: Endoscopic retrograde cholangiopancreatography: toward a better understanding of competence. EndoscopyEndoscopy 31. (9): 755-757.1999 31. (9): 755-757.1999
1111 Eisen GM, Dominitz JA, Faigel DO, American Society for Gastrointestinal Endoscopy. Standards of Practice Eisen GM, Dominitz JA, Faigel DO, American Society for Gastrointestinal Endoscopy. Standards of Practice Committee , et al: Guidelines for advanced endoscopic training. Committee , et al: Guidelines for advanced endoscopic training. Gastrointest EndoscGastrointest Endosc 53. (7): 846-848.2001 53. (7): 846-848.2001
1212 American Society for Gastrointestinal Endoscopy : Principles of training in gastrointestinal endoscopy. From the American Society for Gastrointestinal Endoscopy : Principles of training in gastrointestinal endoscopy. From the ASGE. American Society for Gastrointestinal Endoscopy. ASGE. American Society for Gastrointestinal Endoscopy. Gastrointest EndoscGastrointest Endosc 49. (6): 845-853.1999 49. (6): 845-853.1999
1313 Bucholz EI, Duncan JR: Assessing system performance. Bucholz EI, Duncan JR: Assessing system performance. J Vasc Interv RadiolJ Vasc Interv Radiol 19. (7): 987-994.2008 19. (7): 987-994.2008

Michael S Machuzak, MDMichael S Machuzak, MDMedical Director, Center for Major Airway DiseaseMedical Director, Center for Major Airway Disease
Transplant InstituteTransplant InstituteStaff, Respiratory InstituteStaff, Respiratory Institute
Cleveland ClinicCleveland Clinic
Thank Thank you!you!



What constitutes adequate evidence of competenceWhat constitutes adequate evidence of competence Previous guidelines were expert based and used volume criteria for determining Previous guidelines were expert based and used volume criteria for determining
competencecompetence Lack of empirical data to support these guidelines, and they have been controversialLack of empirical data to support these guidelines, and they have been controversial While volume criteria are practical, their use to define competence is problematicWhile volume criteria are practical, their use to define competence is problematic
Measures of volume are only a surrogate for measures of qualityMeasures of volume are only a surrogate for measures of quality The assumption is that the more a physician performs a procedure, the better he or The assumption is that the more a physician performs a procedure, the better he or
she will beshe will be Precise data describing the learning curve for procedures are difficult to obtainPrecise data describing the learning curve for procedures are difficult to obtain Significant variability in terms of the rate of skill acquisition, so what constitutes Significant variability in terms of the rate of skill acquisition, so what constitutes
sufficient volume to learn a skill may vary widely between individuals. Even if data on sufficient volume to learn a skill may vary widely between individuals. Even if data on learning curves were available, where to set the volume thresholds for certification learning curves were available, where to set the volume thresholds for certification would always be a difficult question given this variability. Should it be toward the top would always be a difficult question given this variability. Should it be toward the top of the distribution, such that 95% of all graduates will have adequate experience? of the distribution, such that 95% of all graduates will have adequate experience? Should it be the median? No matter where we set volume thresholds, the answer will Should it be the median? No matter where we set volume thresholds, the answer will be wrong. Set it too high, and many will be excluded, with the result being slow be wrong. Set it too high, and many will be excluded, with the result being slow dissemination of otherwise useful technologies and missed opportunities. Set it too dissemination of otherwise useful technologies and missed opportunities. Set it too low, and complications and inappropriate utilization patterns will develop. A simpler low, and complications and inappropriate utilization patterns will develop. A simpler solution is to measure and monitor outcomes and performance quality directly and to solution is to measure and monitor outcomes and performance quality directly and to provide feedback to physicians rather than relying solely on expert opinion, volume provide feedback to physicians rather than relying solely on expert opinion, volume requirements, or other surrogate markers. Such a system could be combined with requirements, or other surrogate markers. Such a system could be combined with volume requirements and other didactic instruments. One of the greatest challenges volume requirements and other didactic instruments. One of the greatest challenges in the field, however, is that the necessary procedural quality benchmarks for such a in the field, however, is that the necessary procedural quality benchmarks for such a system do not exist. Registry data, collected by the ACCP, may be able to address this system do not exist. Registry data, collected by the ACCP, may be able to address this in the future.[8] in the future.[8]

Developing the infrastructure necessary for these multiple training environments along with a means of Developing the infrastructure necessary for these multiple training environments along with a means of certification and monitoring of quality will be necessary. One key element that is currently lacking is the certification and monitoring of quality will be necessary. One key element that is currently lacking is the opportunity for supervised hands-on training with new technologies beyond a fellowship. Simulation can opportunity for supervised hands-on training with new technologies beyond a fellowship. Simulation can answer some of these problems, but hands-on patient experience will still be needed.[9] However, it is in this answer some of these problems, but hands-on patient experience will still be needed.[9] However, it is in this area that we face some of the greatest hurdles, since there is no easy way outside of a fellowship for physicians area that we face some of the greatest hurdles, since there is no easy way outside of a fellowship for physicians to get hands-on patient experience. Administrative and legal barriers prevent physicians from easily going to to get hands-on patient experience. Administrative and legal barriers prevent physicians from easily going to other institutions to gain supervised hands-on experience. This has a deadly effect on quality and drastically other institutions to gain supervised hands-on experience. This has a deadly effect on quality and drastically delays the uptake of even the best technologies. It forces physicians to choose between bad options: either delays the uptake of even the best technologies. It forces physicians to choose between bad options: either hold-off on introducing potentially useful new technology or begin using new technology with little in the way of hold-off on introducing potentially useful new technology or begin using new technology with little in the way of prior hands-on experience. Ironically, professors of medicine are not allowed to do what students of medicine prior hands-on experience. Ironically, professors of medicine are not allowed to do what students of medicine do all the time—get hands-on experience somewhere else in a supervised environment. Reform in this area will do all the time—get hands-on experience somewhere else in a supervised environment. Reform in this area will be critical if we are to improve our training system. It will require unconventional thinking, since in this case be critical if we are to improve our training system. It will require unconventional thinking, since in this case the determinants of the quality of care are actually the legal and administrative barriers to training. These are the determinants of the quality of care are actually the legal and administrative barriers to training. These are in urgent need of reform.in urgent need of reform.
Standardization of the IP fellowship curricula will help by providing a framework for discussion of these other Standardization of the IP fellowship curricula will help by providing a framework for discussion of these other areas. In developing standardized curricula, care should also be taken to avoid unnecessary redundancy. areas. In developing standardized curricula, care should also be taken to avoid unnecessary redundancy. Physicians coming to IP fellowship will have had 6 years of training; required elements should be limited to Physicians coming to IP fellowship will have had 6 years of training; required elements should be limited to those things that are truly not covered in sufficient depth during their prior training. Things that should have those things that are truly not covered in sufficient depth during their prior training. Things that should have been learned during prior training can be prerequisites, but such things should not be included as part of the IP been learned during prior training can be prerequisites, but such things should not be included as part of the IP curricula (ie, medical ethics, communication skills). Similarly, mandating procedural training that is well curricula (ie, medical ethics, communication skills). Similarly, mandating procedural training that is well covered in most standard fellowships is probably not warranted. For IP fellowships to be of value, they must covered in most standard fellowships is probably not warranted. For IP fellowships to be of value, they must provide training that is unavailable during standard pulmonary fellowships, and the quality and breadth of that provide training that is unavailable during standard pulmonary fellowships, and the quality and breadth of that training must be consistent between programs, so that other medical professionals and patients will be able to training must be consistent between programs, so that other medical professionals and patients will be able to reliably know what they are getting.reliably know what they are getting.
The proposal by Lamb and colleagues[7] is an important first step in addressing these issues. Individuals may The proposal by Lamb and colleagues[7] is an important first step in addressing these issues. Individuals may hold different beliefs as to whether IP fellowships are essential, a good option, or not necessary. Others may hold different beliefs as to whether IP fellowships are essential, a good option, or not necessary. Others may advocate that certification is best achieved by using volume criteria, performance criteria, or a mixed model. advocate that certification is best achieved by using volume criteria, performance criteria, or a mixed model. However, while there are many unanswered questions and ongoing debates, one thing that is certain is that However, while there are many unanswered questions and ongoing debates, one thing that is certain is that patients and pulmonary medicine will benefit from an academically rigorous and open discussion of how we can patients and pulmonary medicine will benefit from an academically rigorous and open discussion of how we can improve procedural training and certification.improve procedural training and certification.
Ost D, DeRosiers A, Britt EJ, Fein AM, Lesser ML, Mehta AC: Assessment of a bronchoscopy simulator. Ost D, DeRosiers A, Britt EJ, Fein AM, Lesser ML, Mehta AC: Assessment of a bronchoscopy simulator. Am J Am J Respir Crit Care MedRespir Crit Care Med 164. (12): 2248-2255.2001; Abstract 164. (12): 2248-2255.2001; Abstract

Rapid development of new technologies in pulmonary medicine, it has Rapid development of new technologies in pulmonary medicine, it has become increasingly important to ensure that the skills and competency become increasingly important to ensure that the skills and competency needed to provide these services are acquired by practicing physiciansneeded to provide these services are acquired by practicing physicians
Particularly relevant to interventional pulmonology (IP) because of its Particularly relevant to interventional pulmonology (IP) because of its emphasis on technology and proceduresemphasis on technology and procedures
American College of Chest Physicians (ACCP)American College of Chest Physicians (ACCP) European Respiratory SocietyEuropean Respiratory Society American Thoracic SocietyAmerican Thoracic Society Previously issued guidelines regarding training for IP procedures.Previously issued guidelines regarding training for IP procedures.11,,22 Subsequent surveys by the ACCPSubsequent surveys by the ACCP Wide variability between fellowship programs in terms of IP procedures.Wide variability between fellowship programs in terms of IP procedures.33 Not a new problemNot a new problem Over a decade ago demonstrated similar variability in terms of training Over a decade ago demonstrated similar variability in terms of training
for transbronchial needle aspiration.for transbronchial needle aspiration.44,,55 Variability in training adversely impacts patient careVariability in training adversely impacts patient care Lead to underutilization of effective techniquesLead to underutilization of effective techniques Low-quality performance.Low-quality performance.66 It is therefore important that structures and It is therefore important that structures and
processes be developed to facilitate effective procedural training and processes be developed to facilitate effective procedural training and certificationcertification
Chest 123(5):1693-1717; Eur Resir J 19(2): 356-373; Chest 127(5): 1614-1621; Chest 118(3): 625-630; Chest 112(1):251-253; Clin Chest Med 20(1):39-51





























