Embed Size (px)
Citation preview

Interventional Imaging
Steven A. Goldstein MD
Professor of Medicine
Georgetown University Medical Center
MedStar Heart Institute
Washington Hospital Center
Tuesday, October 10, 2017
Cases

DISCLOSURE
I have N O relevant
financial relationships

Management

No symptoms
Symptoms
Refractory Symptoms
Refractory, Severe Sx
Non-obstructionObstruction
No rx
? drug rx
??? DDD-pacing
ETOH septal ablation
B-blockers
Verapamil
Disopyramide
Combined B-blockersand Ca-blockers
Myotomy-Myectomy Transplant
Treatment Strategies for HCM
HCM121

Drug-Refractory HCM
Therapeutic Options
Surgery Dual-chamber
pacemaker
Septal
Ablation

Alcohol Ablation

Alcohol Septal Ablation
• 1994 – 1st procedure at Royal Brompton
• Since then >10,000 performed

HCM - Alcohol Septal Ablation
Indications
• NYHA Class III nor IV*
• LVOT gradient > 50 mmHg at rest
• ≥ 1 septal branch of LAD suitable for intervention
(*unresponsive to maximum medical treatment)
(or with physiologic provacative maneuvers)

HCM - Alcohol Septal Ablation
Selection Criteria
• Symptoms that interfere substantially with
QOL despite optimal medical mgt
• Septal thickness ≥ 1.6 cm
• LVOT gradient ≥ 30 mm Hg at rest or ≥ 50
mmHg with provocation
• Accessible, appropriate septal perforator(s)
• Absence of intrinsic MV abnormality
• Absence of other conditions warranting
cardiac surgery

HOCM - Alcohol Septal Ablation
Echo Methods for Guidance
• Transthoracic echo
• Transesophageal echo
• Intracardiac echo
(TTE)
(TEE)
(ICE)
Majorityof
centers
WHC*
* Moderate sedation; NOT general anesthesia

HOCM - Alcohol Septal Ablation
TEE Views
• Apical 4-chamber view (0°)
• Longitudinal view (120-130°)
• Gastric short-axis view
• Deep transgastric view (for gradient)

Using intracoronary injection of an echo
contrast agent, opacification of the
strategic septal area can be delineated.
Hypertrophic Cardiomyopathy
Alcohol Septal Ablation

Transesophageal Transthoracic
Alcohol Ablation of Septum in HCM
Echo in Cath Lab During Procedure

HOCM - Alcohol Septal Ablation
Echo Guidance During Procedure
Myocardial Contrast Echo
(Intracoronary Contrast)
Goal: Delineate strategic
portion of septum
(perfusion territory of target
septal perforator)

HCM - Alcohol Septal Ablation
Similar to surgical myectomy, this procedure
attempts to debulk the septum in the region
where the LVOT obstruction occurs
A localized myocardial infarction is created by
injecting ethanol into the septal perforator that
supplies the septal myocardium adjacent to
the point of mitral leaflet (SAM)-septal contact

Ethanol-induced
infarction
Alcohol Ablation of Septum in HCM
Nishimura and Holmes N Engl J Med 350:1320(2004)

HOCM - Alcohol Septal Ablation
What to Evaluate Pre-Procedure
• Site and extent of septal hypertrophy
• Intracavitary gradient
• Localization of SAM-septal contact
• Mitral regurgitation (mechanism and degree)

"An important improvement of the new
method in our opinion has been gained
by the integration of echo monitoring"
Faber, Seggewiss, et al
Circulation 98:2415(1998)

0
20
40
60
80
100
>50%reduction Clinical
No Contrast
Contrast
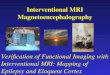
Septal Ablation in HCM
Contrast Echo Helps Improve Results
p<0.01 p<0.05
(n=30)
(n=91)
% P
ati
en
ts
in LVOTG
70
9286
97
improvement
Faber, Seggewiss Circulation 98:2415(1998)

HOCM - Alcohol Septal Ablation
Echo Guidance During Procedure
Assess Immediate Results
• Reduction of contractility/thickening of septum
• Elimination/reduction of SAM
• Elimination/reduction of gradient
• Elimination/reduction of mitral regurgitation

HOCM - Alcohol Septal Ablation
Follow-Up (Post-Procedure Echo)
• LVOT gradient
• Mitral regurgitation
• Diastolic Filling
• Regression of hypertrophy
• LV function (especially septum)

HOCM - Alcohol Septal Ablation
Echo Guidance During Procedure
Goal: Delineate strategic portion of septum
(perfusion territory of target septal perforator)
Myocardial Contrast Echo
(Intracoronary Contrast)

Transesophageal Transthoracic
Alcohol Ablation of Septum in HCM
Echo in Cath Lab During Procedure

Case 1

MM - 61 year-old man
Case 2

Case 3

Case 4

Case 5
BP - 69 year-old female
Aborted RV papillary muscle perfused

Pericardiocentesis

Pericardiocentesis Using Subxiphoid Approach
“Old-Fashioned Way” alligator clip to ECG

Echo-Guided
Pericardiocentesis
• Gold-standard for management of
• Improves success rate
• Improves safety
• Reduces complication rate
effusions reguiring drainage

Location of Needle Entry
Subcostal
Chest wall (79%)
Unknown
Para-apical 67%
L parasternal 6%
L axillary 4%
R parasternal 2%
Posterolateral 0.2%
n = 1,131
Mayo Clinic: courtesy Seward/Khandheria

Needle Attempts for Access
PC
(%)
Number of needle attemptsn = 1,131
Mayo Clinic: courtesy Seward/Khandheria

Success and Complications of
(Consecutive 1,131 procedures)
Successful PC 1,097 (97%)
Major complications 16 (1.4%)
Death 1
Ventricular laceration 6
Intercostal vessel injury 1
Pneumothorax 6
Ventricular tachycardia 1
Infection 1
Minor complications 37 (3.3%)
Mayo Clinic: courtesy Seward/Khandheria

Management of
Cardiac Tamponade
• 1978 Blind pericardiocentesis
• 6% mortality, 50% morbidity
• Echo-guided centesis: n = 1,131
• <0.1% mortality, <2% morbidity
Mayo Clinic: courtesy Seward/Khandheria

Pericardiocentesis
• Call 7-6146 for Microbiology to tube
2 aerobic culture specimen bottles to
the front desk # 205
• Elevate HOB with wedge @ 45°
• Chest prepped and draped
• Page echo stat to Cath Lab (7-6700)
• Sedate as ordered
• Closely monitor HR & BP
• Drop (2) 20cc syringes for labs
• Obtain CCU or ICU bed
• Patient may be sent to a 4th floor
cardiac bed if hemodynamically
stable
• Complete blue FLUID lab
slip with:
• Cell count (purple tube)
• 1 air tight 20 cc syringe
(capped)
• Gram stain
• AFB smear and culture
• Aerobic, anaerobic cultures
• Fungal culture
• Cytology
• Glucose
• Total protein
• Albumin
• LDH
• Adenosine deaminase

Apical Approach

Apical-Lateral Approach

Case 1JC - 55 year-old woman
Contrast confirms

Case 2EW - 80 year-old woman
Apical approach

pericardiocentesis
site (apical)
Not optimal

Case 3TJ - 71 year-old man
Pericardiocentesis
L-axillary approach

pericardiocentesis
site (subaxillary-
lateral))
Not optimal

Case 4RD - 77 year-old man
Massive pericardial effusion