Embed Size (px)
Citation preview
Interval History
• The patient was admitted to respiratory isolation to rule out active infection with Mycobacterium Tuberculosis
• Acid-fast bacilli culture and smear were negative
• The patient improved on empiric NSAIDs and was discharged home
• The patient returned to her baseline exercise tolerance and was asymptomatic within 1 week
Interval History
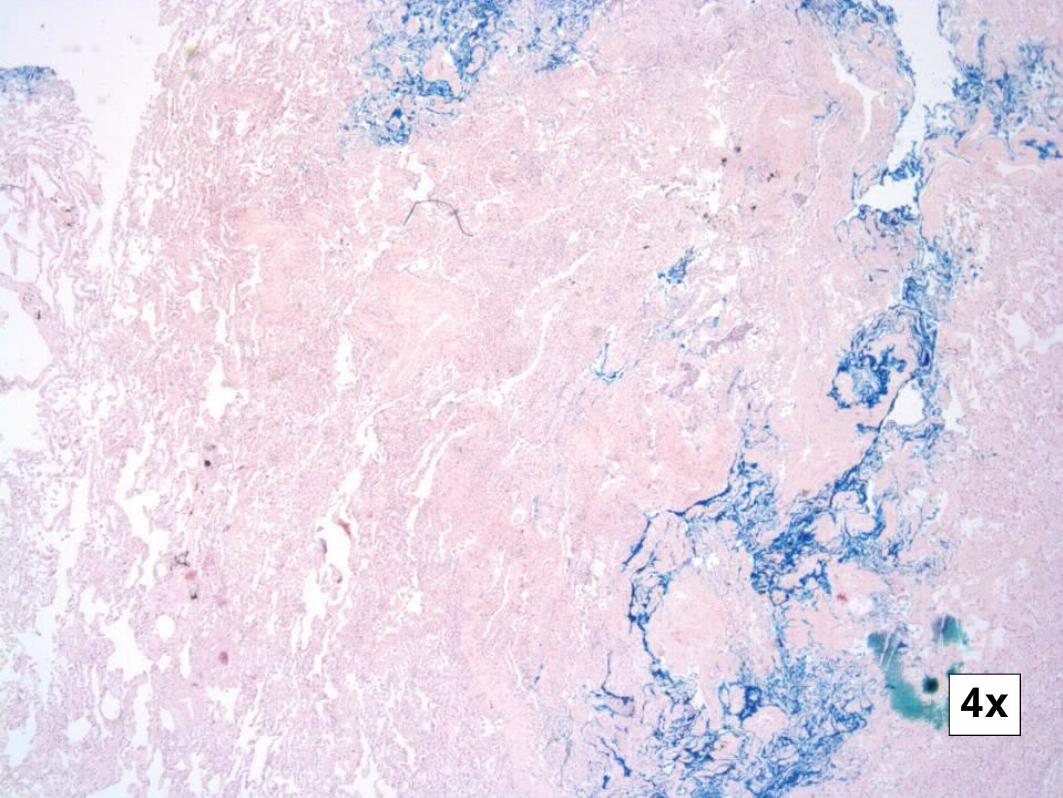
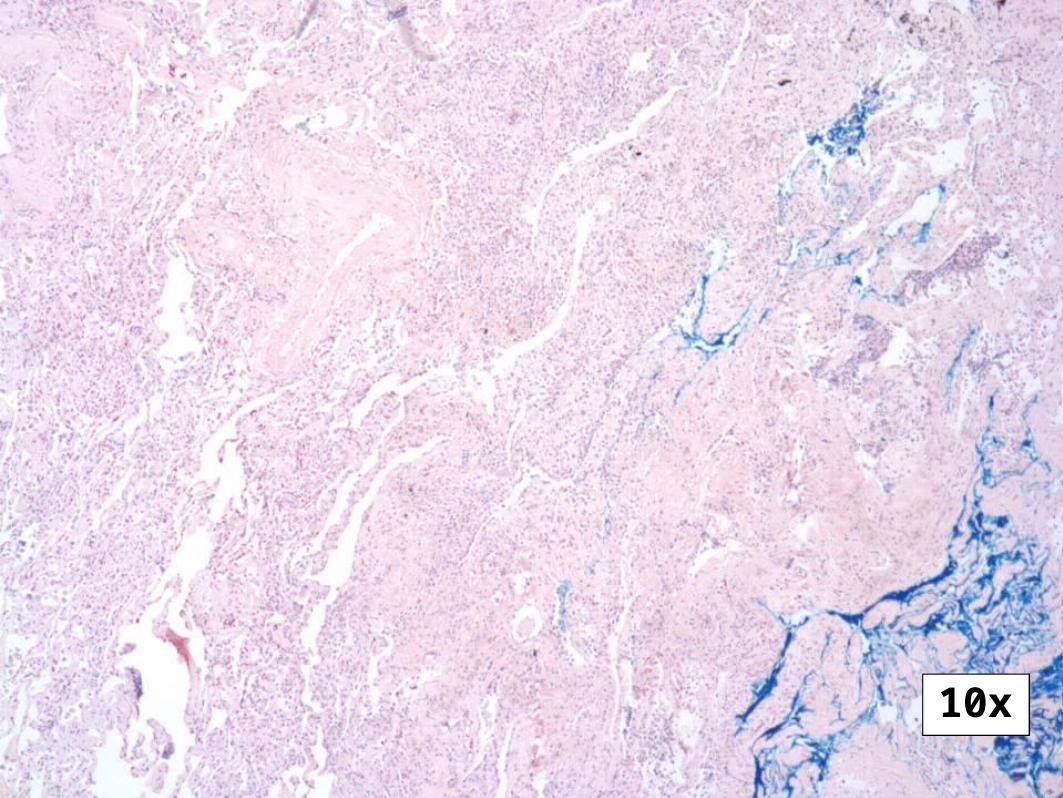
• Repeat CT imaging showed resolution of effusions, but persistent nodules, concerning for metastatic disease of unknown primary
• PET Scan and Abdominal CT scans did not show evidence of extrapulmonary malignancy
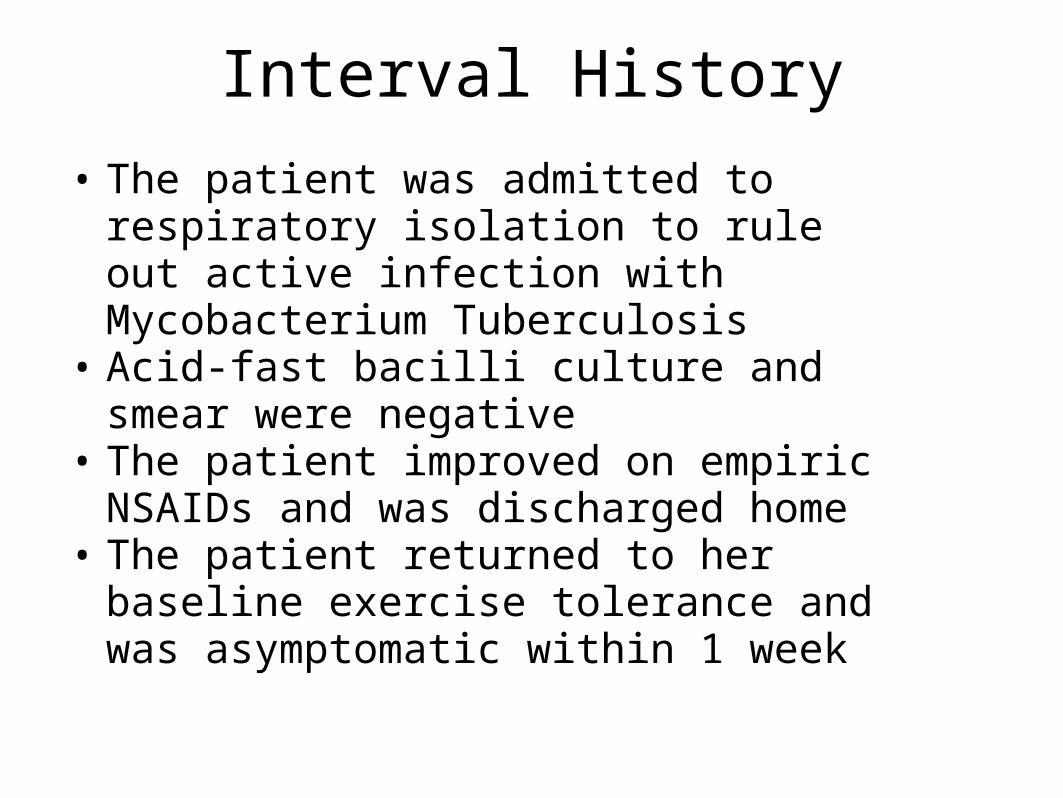
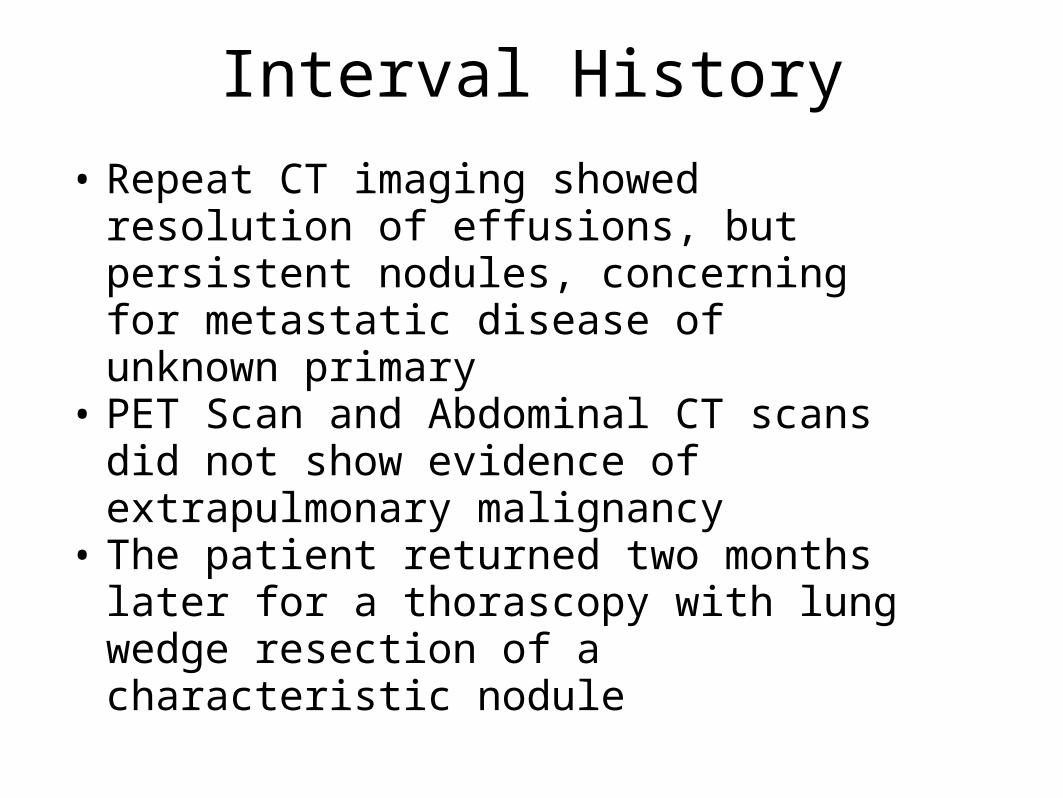
• The patient returned two months later for a thorascopy with lung wedge resection of a characteristic nodule
4x
10x
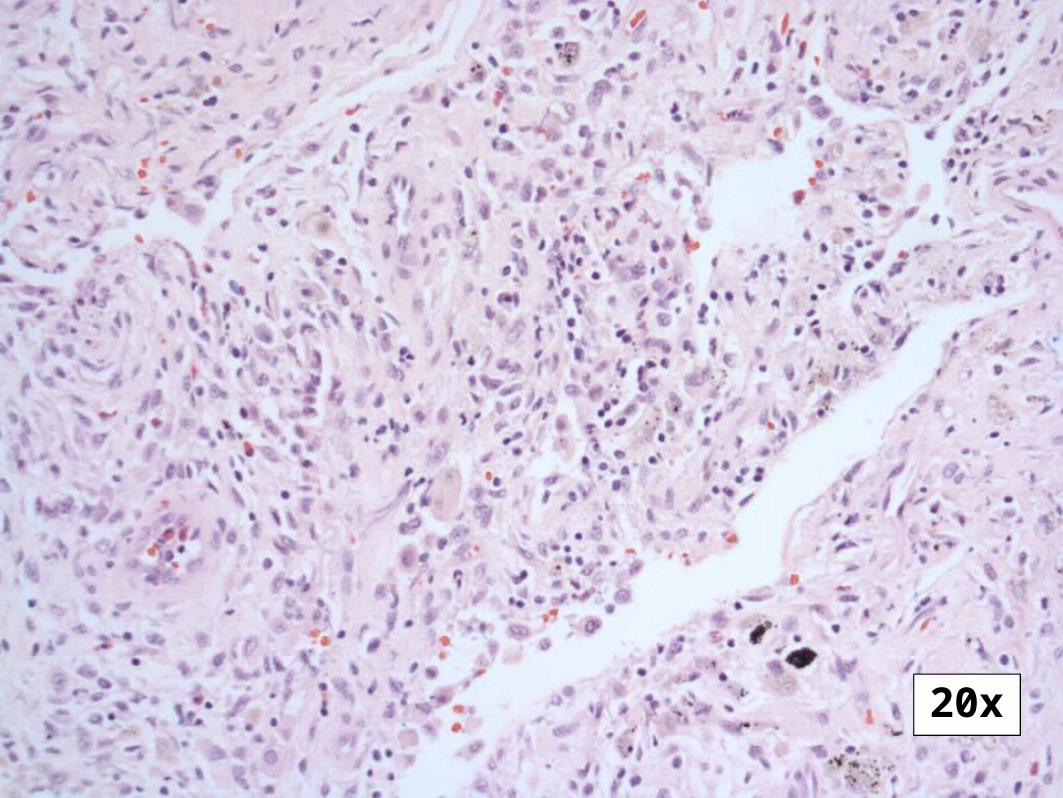
20x
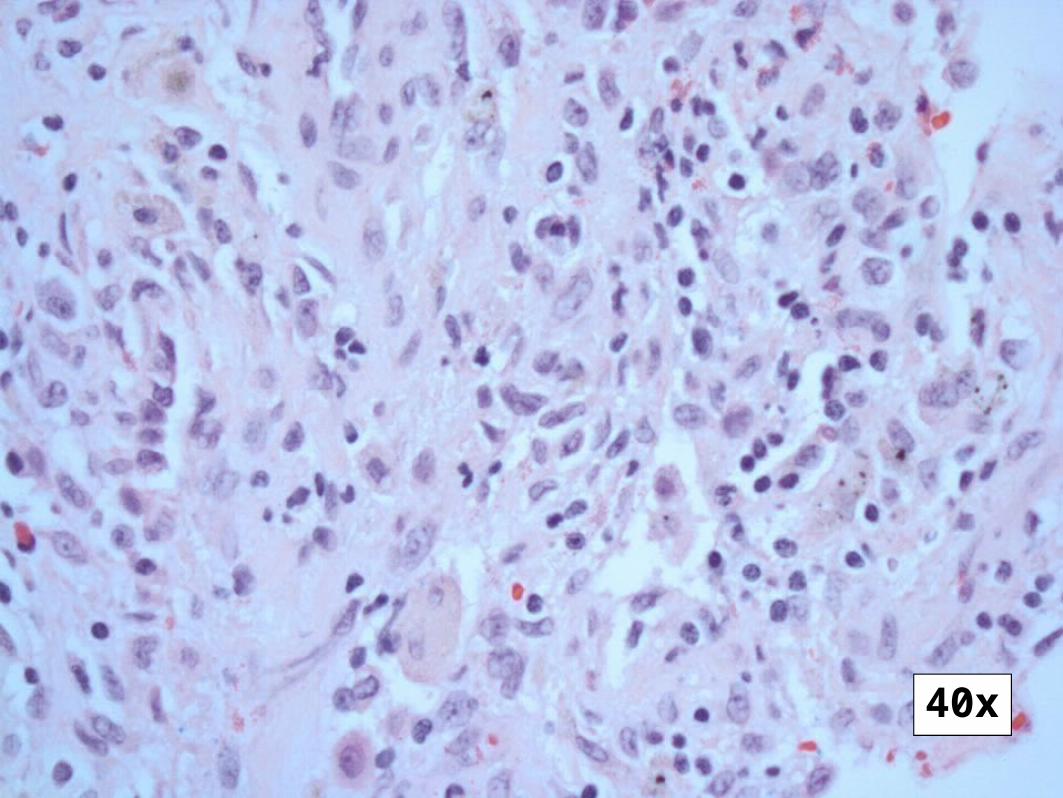
40x
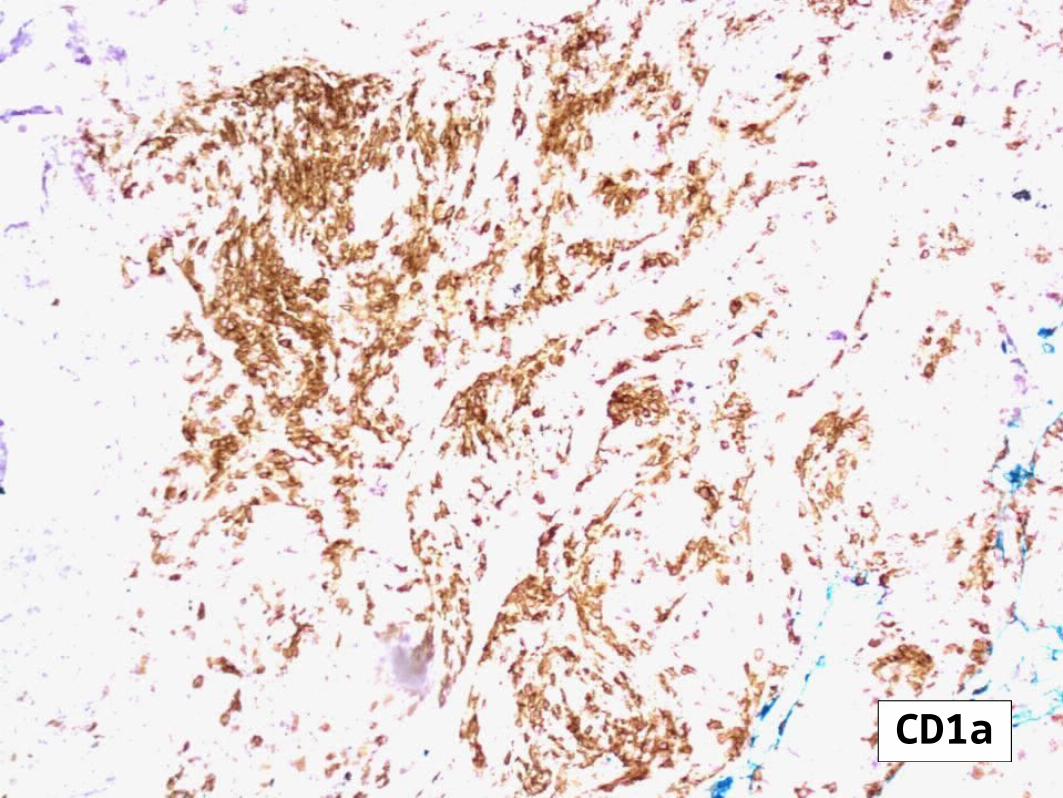
CD1a
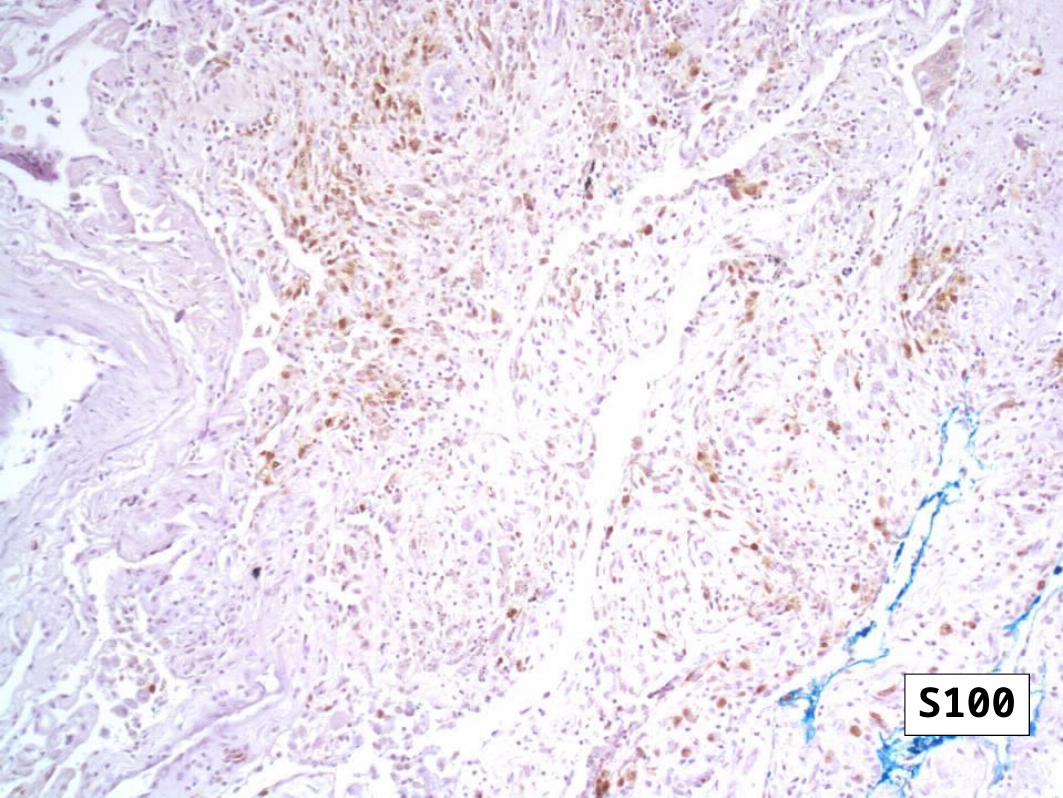
S100
PULMONARY LANGERHANS’- CELL HYSTIOCYTOSIS
Final Pathological Diagnosis
PLCH: Introduction
• Histiocytosis encompasses a group of diverse disorders with the common primary event of the accumulation and infiltration of monocytes, macrophages, and dendritic cells in the affected tissues
• Langerhans Cells are a dendritic cell subtype and part of the monocyte-macrophage lineage derived from bone marrow involved in antigen presentation in the tracheobronchial tree
Classification of Histiocytosis
• Single-organ involvemento Lung (>85% of lung involvement occurs in isolation)o Boneo Skino Pituitaryo Lymph Nodeso Thyroid, Liver, Spleen, Brain
• Multisystem Diseaseo Multiorgan disease with lung involvemento Multiorgan disease without lung involvemento Multiorgan histiocytic disorder
Historical Terms
• Hystiocytosis X• Eosinophilic Granuloma• Letter-Siwe disease
o A rare systemic aggressive disease seen in adults
• Hand-Schüller-Christian diseaseo Triad of exopthalmos, central diabetes
insipidus, and bone lesions
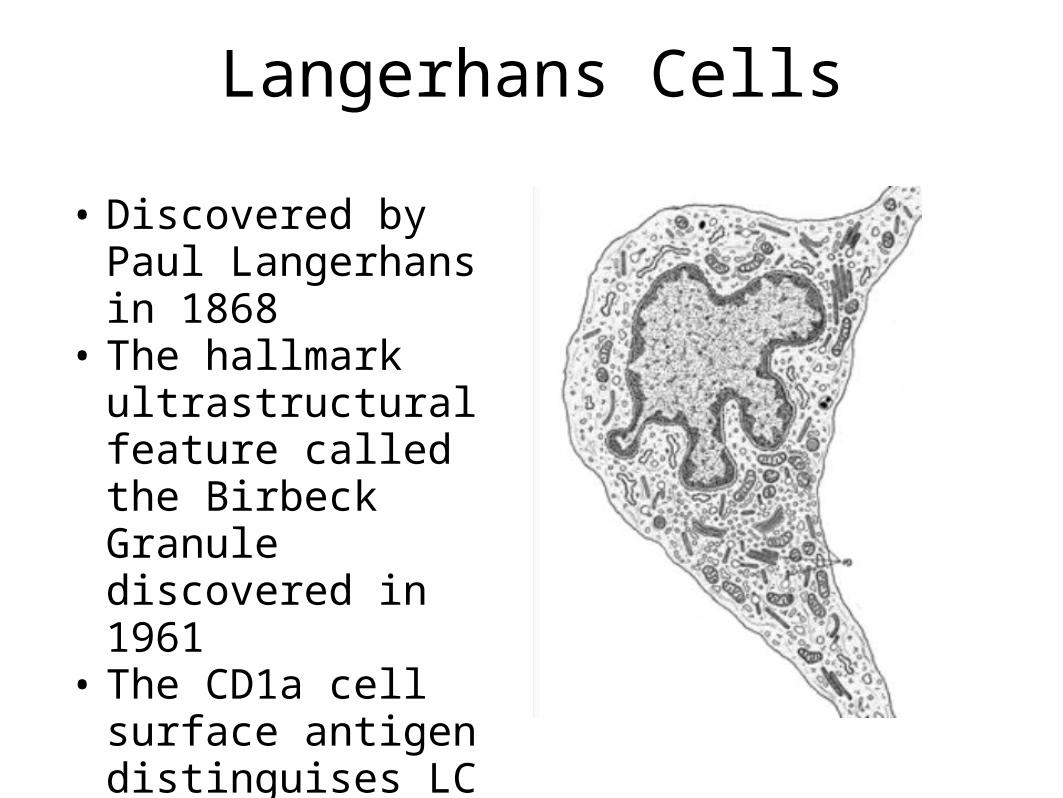
Langerhans Cells
• Discovered by Paul Langerhans in 1868
• The hallmark ultrastructural feature called the Birbeck Granule discovered in 1961
• The CD1a cell surface antigen distinguises LC from other histiocytes
Epidemiology
• Precise incidence and prevalence is hard to define in this diseaseo 1200 new cases per yearo 0.5-5.4 cases / million
• 5% of lung-biopsy specimens in patients with ILD result in PLCH
• No known genetic susceptibility• Mainly in caucasians. Male to female
ratio is changing over the decades…• >90% of PLCH patients are smokers
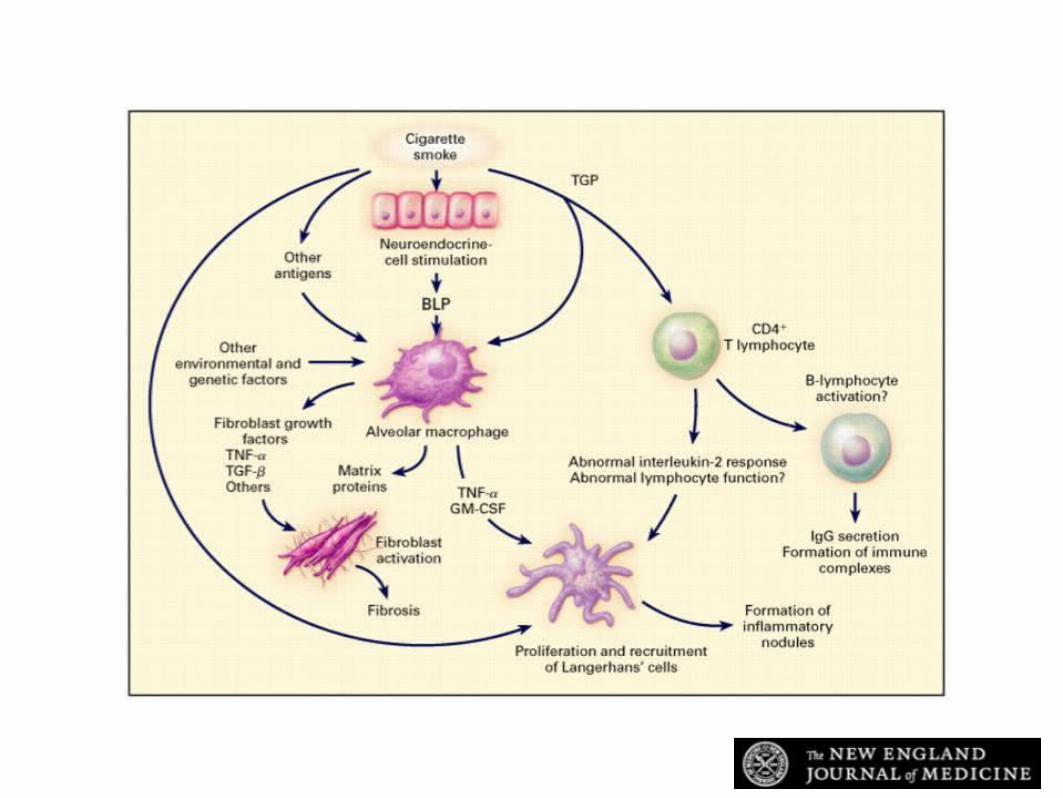
Vassallo R et al. N Engl J Med 2000;342:1969-1978
Proposed Pathogenesis of PLCH

Reactive vs. Neoplastic?
• Spontaneous remission
• Abscence of chromosomal abnormalities
• Overall good prognosis in majority of cases
• Monoclonal proliferation in extrapulmonary tissue
• Infiltration of aberrent cells into normal tissue
• Response to chemotherapy and possible fatal outcome in more severe cases
Histopathological Features
• Proliferation of Lagerhans Cells along the small airways serves as the nidus of cellular/fibrotic nodules from 5mm to 1.5 in size. Eosinophils may be present
• In severe disease, nodules may interconnect and cavitate to produce distinctive honeycomb-like structures
• Given that most patients are smokers, concominant COPD and ILD 2/2 respiratory bronchiolitis is often present
Clinical Presentation
• Cough (50-70%)• Dyspnea (30-50%)• Fever, weight loss, diaphoresis (20-
30%)• Asymptomatic (25%)• Chest Pain (10%)
Clinical Presentation
• Pneumothorax (10-20%)• Extrapulmonary disease (15%)• Pulmonary hypertension• Respiratory failure• Secondary malignancy
• Physical Exam and Laboratory findings are variable
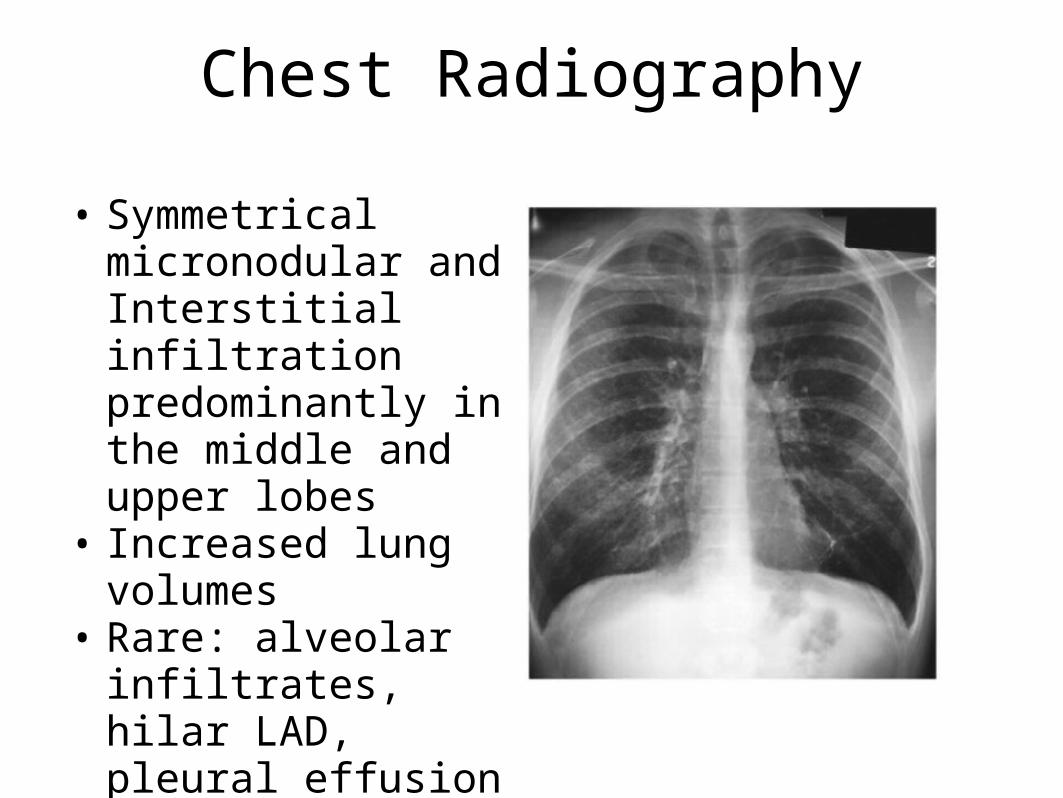
Chest Radiography
• Symmetrical micronodular and Interstitial infiltration predominantly in the middle and upper lobes
• Increased lung volumes
• Rare: alveolar infiltrates, hilar LAD, pleural effusion
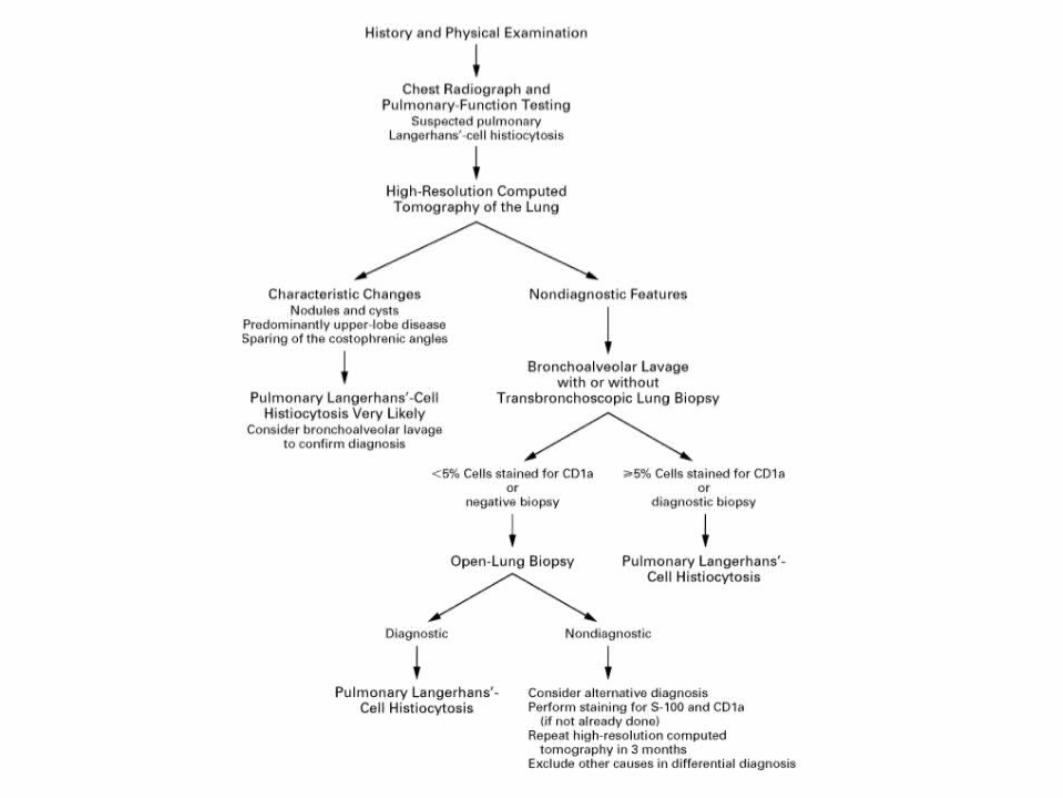
Tissue Diagnosis
• Bronchoalveolar Lavage• Transbronchial Biopsy• Open vs. Thorascopic Lung
Biopsy
Management
• Smoking Cessation• Corticosteroids• Chemotherapy
o Vinblastine, MTX, Cyclophosphamide, Etoposide
o 2-chlorodeoxyadenosine• Immune modulation: Etanercept• Pleurodesis of pneumothoraces• Serial TTE and PFTs to monitor
progression
Prognosis
• For a majority of patients, the disease regresses with smoking cessation
• It is not known to predict those who tend to progress, although age, prolonged constitutional symptoms, extrapulmonary involvement, abnormal PFTs are markers of poor outcome
Back to our case…
• This patient has baseline respiratory insufficiency 2/2 PLCH and COPD, but presented with an acute respiratory illness not characteristic of these diagnoses
• She endorsed chills, dyspnea, and chest pain. There was radiographic evidence of pleuropericarditis which symptomatically and radiographically improved within 1-2 weeks on NSAIDs
Dfdx of pleuropericarditis
• Viral / Acute idiopathic • Drug-induced• Collagen vascular: Sarcoid, RF, Lupus• Tuberculosis• Malignancy• Infarction pericarditis• Uremia• Atypical infections: fungal
Follow-up• Pleural fluid was negative for Acid-Fast,
Bacterial or Fungal organisms• HIV Negative• The patient continues to struggle with
smoking cessation and reports baseline shortness of breath and cough
• The patient reports an increase in smoking because of the anxiety of “having cancer”
• Steroids have not been offerred due to the relatively mild course of her disease
Dfdx of pleuropericarditis
• Viral / Acute idiopathic• Drug-induced• Collagen vascular: Sarcoid, RF, Lupus• Tuberculosis• Malignancy• Infarction pericarditis• Uremia• Atypical infections: fungal
Dfdx of pleuropericarditis
• Viral / Acute Idiopathic• Drug-induced• Collagen vascular: Sarcoid, RF, Lupus• Tuberculosis• Malignancy• Infarction pericarditis• Uremia• Atypical infections: fungal
Final Diagnoses
• Pulmonary Langerhans’-Cell Histiocytosis, • Acute Viral Plueropericarditis
• Active Tobacco Abuse• Coronary Artery Disease• COPD• Essential HTN• Anxiety / Dysthymia
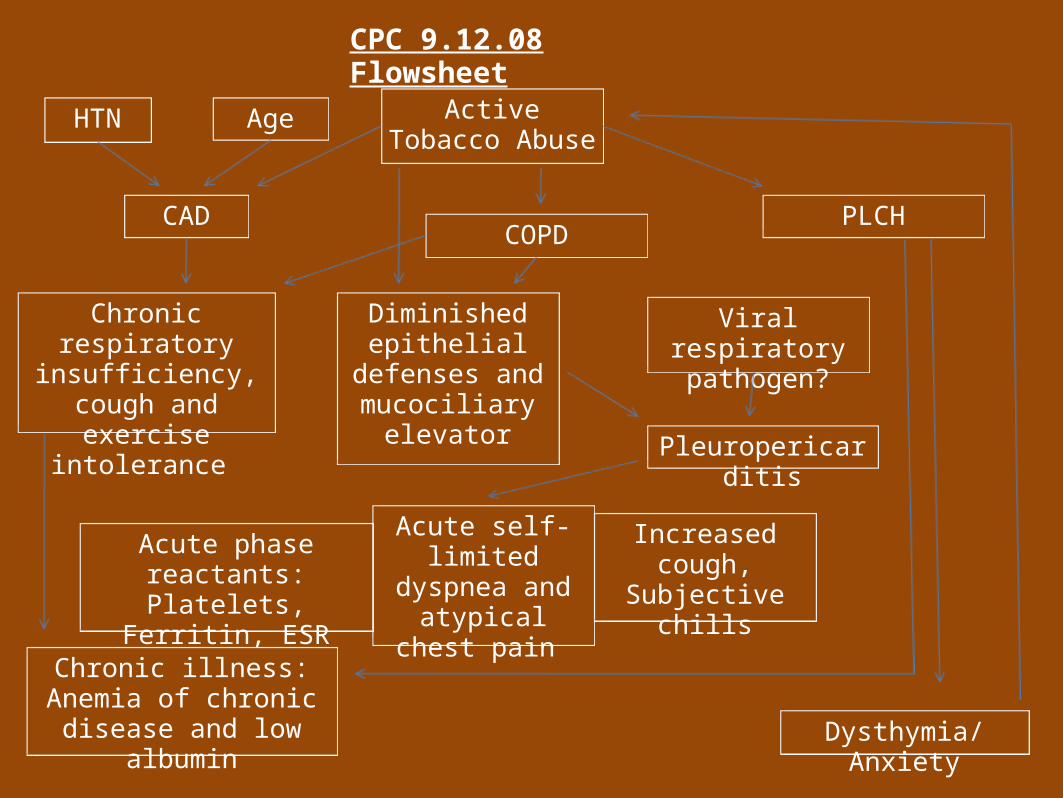
Active Tobacco Abuse
COPD
HTN
CAD PLCH
Age
Diminished epithelial
defenses and mucociliary
elevator
Viral respiratory pathogen?
Pleuropericarditis
Chronic respiratory insufficiency, cough
and exercise intolerance
Acute self-limited dyspnea and atypical chest
pain
Increased cough, Subjective chills
CPC 9.12.08 Flowsheet
Acute phase reactants: Platelets, Ferritin, ESR
Dysthymia/Anxiety
Chronic illness: Anemia of chronic disease and
low albumin
Thank You!
• Dr. Martin Blaser• Dr. Anthony Grieco• Dr. Elvio Ardilles• Dr. Jonathon Ralston• Dr. Kristin Remus• Dr. James Tsay• Dr. Christina Yoon





























