-
Journal of Clinical InvestigationVol. 45, No. 12, 1966
Further Studies on the Interrelationship betweenParathyroid
Hormone and Vitamin D *
CLAUDEARNAUD,HOWARDRASMUSSEN,tANDCONSTANTINEANASTt(From the
Department of Biochemistry, University of Pennsylvania School of
Medicine,
Philadelphia, Pa., and the Department of Pediatrics, University
of Missouri Schoolof Medicine, Columbia, Mo.)
Calcium homeostasis is achieved by the inter-play of a number of
humoral agents (1). Ofcentral importance are the activities of
parathyroidhormone (PTH) and of vitamin D. This wasfully
appreciated 35 years ago (2), but in spiteof considerable effort,
the nature of the relation-ship remains controversial. Recent
opinion hasvaried from that of a complete dependence ofhormone
action upon the presence of vitamin D(3) to that of a complete
independence of action(4, 5). In our initial studies of this
problem, weconcluded that in the absence of vitamin D aphysiologic
concentration of parathyroid hormoneexerted its usual effect upon
the renal excretionof phosphate but was unable to mobilize
calciumfrom bone (6).
Since these studies were published, two groupsof investigators
have challenged our conclusions(7, 4). Harrison and Harrison
reaffirmed theirprevious observations (7) and concluded, as theyhad
before, that all of the actions of parathyroidhormone depended upon
vitamin D. At the oppo-site extreme, Ney and associates concluded
that allof the effects of parathyroid hormone are exertedin the
D-deficient organism. These differencesare difficult to explain.
However, both studiesdiffered from ours in several respects. In
thestudy of Harrison and Harrison (7), no attemptwas made to define
or control the level of endoge-nous parathyroid hormone, although
we found this
* Submitted for publication April 8, 1966; acceptedSeptember 7,
1966.
Presented in part at the 47th Annual Meeting of theEndocrine
Society, June 1965.
Supported by grants from the National Institutes ofHealth
(AM-09650, AM-09494-01, and AM-01351-08).
tAddress requests for reprints to Dr. Howard Ras-mussen, Dept.
of Biochemistry, University of Pennsyl-vania School of Medicine,
Philadelphia, Pa.
t Dept. of Pediatrics, University of Missouri, Columbia,Mo.
to be of prime importance (6). In the work doneby Ney and
co-workers a different species wasemployed, and the degree of D
deficiency wasassessed by different criteria (4). Nevertheless,both
studies raised points that seemed worthy offurther examination.
The development of a technique for study ofthe response of the
conscious rat to the long-termperfusion of hormones (8) has allowed
us to ex-amine several aspects of this problem more di-rectly. The
experimental design permitted theexclusion of altered endogenous
secretion of para-thyroid hormone or thyrocalcitonin as
variables.The results reaffirm our previous conclusion andexplain,
in large part, the previous disparity ofopinion regarding the
nature of the parathyroidhormone vitamin D interrelationship.
Methods
Vitamin D deficiency was produced in young growingHoltzman rats
as previously described (9). Control ani-mals received the same
purified diet but were given 75 Uof vitamin D3 in cottonseed oil by
oral intubation dailyfor the week before study. Urinary calcium and
phos-phate were measured simultaneously with a
TechniconAutoanalyzer (6). Plasma calcium and phosphate
weremeasured by the same means except for a manifold modi-fication
that allowed for a microdetermination on 50 to100 Id of plasma.
Magnesium in the urine was measuredby absorption flame
spectrophotometry with a Perkin-Elmer instrument (10). Urinary
sodium and potassiumwere measured by emission spectrophotometry
with aZeiss instrument. Urinary inulin was measured by anautomated
procedure with a Technicon Autoanalyzer (11).
The technique of long-term perfusion of the rat wasdeveloped as
a modification of that described by Cotlove(12). With rats under
ether anesthesia, a no. 240polyethylene catheter 1 was placed in
the urinary bladder,a no. 50 polyethylene catheter 1 was placed in
the ex-ternal jugular vein, and the parathyroid or both thy-roid
and parathyroid glands were removed by surgicalmeans. In some
instances parathyroidectomy was per-
' Clay-Adams Co., New York, N. Y.
1955
-
C. ARNAUD, H. RASMUSSEN,AND C. ANAST
TABLE I
Electrolyte balance during period of control infusion
No. ofexperi-ments Na K Mg Ca
/Amoles/hr pmoles/hr jumoles/hr itmoles/hrPTX*
+D 6 +38 -4 4t -11 ±3 +3± 0.5 +10 ± 2-D 5 +26 ± 4 -22 ± 4 +1 ±
0.25 +14 ± 3
High Ca-D 4 + 8 ±1
Sham+D 4 +28 ± 5 -16 ± 4 -2 ±t 0.5 + 8 ± 2-D 4 -15 ±3 - 9 ±2
+4±0.5 +13 ±3
* PTX = parathyroidectomized rats; high Ca = rats fed a
highcalcium vitamin D-deficient diet; sham = sham-operated control
rats.
t Mean ± standard deviation.
formed with an electric cautery. After surgery, the ani-mal was
placed in a cage similar to that designed byCotlove (12) with the
jugular vein catheter exitingthrough the top and the bladder
catheter and hind legsthrough the rectangular opening in the
bottom. Thejugular vein catheter was connected to a peristaltic
pumpthat delivered 3.0 to 4.0 ml per hour. The animals wereperfused
at this rate with a solution containing 4%o dex-trose, 5 mMcalcium
chloride, 5 mMmagnesium chloride,20 mMsodium chloride, 2.5
mMpotassium chloride, and20 mg per L inulin. Urine was collected at
half-hour or2-hour intervals. The animals were perfused for 16
hoursafter surgery before measurements of urinary volume
anddeterminations of electrolyte content were begun. Collec-tions
were then made during a control period of at least10 hours before
parathyroid hormone (5 ,ug per hour) wasadded to the perfusate.
Hormone infusion was usuallycontinued for 20 hours, and then a
period without hor-mone was recorded. Weobtained blood samples by
car-diac puncture before surgery in order to measure plasmacalcium
and phosphate. This was done to be certain ofthe degree of D
deficiency or D repletion. Rats wereconsidered D deficient only if
they had stopped gainingweight after 3 weeks of vitamin D-free diet
and if theconcentration of calcium in the plasma (plasma
calcium)was below 6.5 mg per 100 ml. The mean plasma calciumvalue
of the D-fed controls was 10.8 ± 0.4 mg per 100ml before surgery.
One group of animals was raised ona high calcium vitamin D-free
diet, and their mean pre-operative plasma calcium was 9.6 + 0.3 mg
per 100 ml.These animals did not stop gaining weight but were
con-sidered vitamin D deficient because littermates raised ona
normal calcium D-deficient diet in adjacent individualcages
exhibited classic disturbances in growth and plasmacalcium levels.
The number of animals studied in eachgroup is indicated in the
Figure legends; standard statis-tical methods were used to obtain
values for standarderror of the mean and significance of the
differencesbetween means (13).
The purified parathyroid hormone used was preparedby the method
of Hawker, Glass, and Rasmussen (14).
Results
Initially, the reproducibility of the perfusiontechnique was
established. Two problems of im-mediate concern were the stability
of the base-linerates of electrolyte excretion and the balance
offluid and electrolytes.
Wefound that 10 to 15 hours of perfusion withthe control
solution was necessary before the ratesof excretion of the various
electrolytes becamestable. Therefore, in all experiments to be
re-ported, the animals were perfused for at least 15hours before
urine collections were begun. Col-lections over the ensuing 10
hours constituted thecontrol period for each experiment.
After the postsurgical equilibration period, therates of urine
flow were from 0.05 to 0.1 mlper hour less than the measured rates
of perfusateinfusion in all the animals. However, there ap-peared
to be no significant fluid retention. Theanimals weighed 3 to 4 g
less after a 50-hourexperiment than before surgery. Postmortem
ex-amination revealed no evidence of abnormal fluid
VITAMIN D DEFICIENTPTH 5%pg/HR I
_ ^A ... ,,,..::% >
...494
1 1 I I I I
20 30 0 10 20 30TIME-HOURS
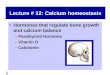
FIG. 1. RATES OF EXCRETION OF INULIN, PHOSPHATE,CALCIUM,
MAGNESIUM, POTASSIUM, AND SODIUM BEFOREAND DURING THE INFUSION OF
PARATHYROID HORMONE(PTH). Five ,ug per hour PTHwas infused into a
D-fed(left) and a D-deficient (right) parathyroidectomizedrat
maintained on a constant infusion of glucose andelectrolytes.
1956
-
PARATHYROIDHORMONEAND VITAMIN D
retention, and the rates of infusion were less thanthe maximal
rates the rats could tolerate. Ratesof urine flow up to 5.0 to 6.0
ml per hour couldbe produced by increasing the rate of
infusion.Because of these facts, it was concluded that theslight
discrepancies between rates of infusion andrates of urine flow were
accounted for by insen-sible water loss and possibly by slight
evaporationfrom the urine samples when they were in thefraction
collector. It should be noted, however,that there was usually
sodium retention and alwayspotassium loss during the control period
(TableI), possibly as a result of adrenal hyperactivitysecondary to
the stress of surgery and experi-mentation. In all instances in
which sodiumretention occurred, it was followed by sodiumdiuresis
during hormone infusion (Figures 1 and2). Magnesium excretion
balanced intake, butthere was always calcium retention that was
moremarked in the D-deficient than in the D-fed ani-mals (Table
I).
Our initial studies were carried out in para-thyroidectomized
animals. Two typical experi-ments are shown in Figure 1. In the rat
fedvitamin D, the infusion of parathyroid hormoneat a rate of 5 Fug
per hour led to a prompt increasein the rate of excretion of
phosphate, potassium,and sodium, and an initial fall in magnesium
andcalcium excretion (Figure 1). The changes inrates of magnesium
and potassium excretion werenot sustained but returned to baseline
or slightlygreater values after 4 to 6 hours of perfusion.In
contrast, the initial phosphaturia was followedby a sustained
phosphate excretion throughoutthe course of the perfusion. Calcium
excretion,after decreasing initially, returned to the controlrate
and then rose, after 15 to 22 hours of constanthormone perfusion,
to a rate considerably higherthan that observed initially. Changes
in the rateof sodium excretion were more variable but ingeneral
paralleled those of phosphate.
In contrast, the infusion of hormone at the samerate into a
D-deficient parathyroidectomized ratled to the initial changes in
electrolyte excretionthat were qualitatively similar to those seen
in theD-fed animal, i.e., an increased rate of sodium,potassium,
and phosphate excretion, and a fallin excretion of calcium and
magnesium. However,a different pattern of response emerged during
thelater hours of perfusion (Figure 1). The rate of
TIME, HOURS
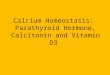
FIG. 2. PATTERNSOF URINARY ELECTROLYTEEXCRETIONBEFORE, DURING,
ANDAFTER THE INFUSION OF PARATHYROID
HORMONE, 5 ,uG PER HOUR, IN PARATHYROIDECTOMIZED(PTrX) AND
SHAM-OPERATEDD-DEFICIENT AND D-FED RATS.All animals were maintained
on a normal calcium andphosphate diet, except the third group of
D-deficientanimals, which were maintained on a high calcium
normalphosphate diet. The shaded areas represent the valuesduring
hormone infusion. Number of animals in eachgroup: +D, 6; -D, 5; -D
high calcium diet, 4; +Dsham, 4; -D sham, 4.
phosphate excretion fell, after the initial increase,to rates
only slightly greater than the control rates;the initial decrease
in rate of calcium excretion wasfollowed by a gradual return to a
rate nearly equalto, but never in excess of, the control.
Also,sodium diuresis was not sustained as in the D-fedanimal.
The rates of inulin excretion were also mea-sured in these
animals. There was no significantchange in the excretion of
constantly infusedinulin during hormone infusion in either
animal(Figure 1). Rates of inulin excretion were mea-sured in six
additional animals, and in all instancesthe infusion of parathyroid
hormone at a rate of5 ug per hour had no effect upon this rate.
The same protocol was followed in six otherD-fed and five other
D-deficient animals. Theresults are recorded as the means of the
values
1957
-
C. ARNAUD, H. RASMUSSEN,AND C. ANAST
TABLE II
Comparison of responses to parathyroid hormone infusion in
parathyroidectomizedvitamin D-fed and D-deficient rats
Urinary electrolyte excretion in 5 hours
Animal* HP04- Ca++ Mg K Na
jumoles jsmoles pmoles Amoles Ismoles+D 24.0 -± 4.2 36.0 it 4.4
69.0 ±- 5.2 108 ±t 10 150 ±- 13-D Ct 7.5 it 3.0$ 27.0 it 3.4 75.0
-- 5.8 150 it 11$ 180 -± 17- D(Ca) 6.1 i 2.6T 34.0 It 4.7
+D 258.0 i 20 7.5 it 2.3 48.0 it 5.8 180 it 12 330 it 12-D 5
120.0 ±i 9$ 3.6 ±t 0.9$ 33.0 4t 4.9§ 165 ±t 11 390 it 14t- D(Ca)
204.0 -- 12§ 8.0 -- 2.5
+D 188.0 it 15 28.0 -- 4.3 81.6 it 6.3 236 -- 15 414 It 16-D 10
65.0 ±t 8$ 17.0 ±- 5.2$ 73.0 ±t 6.2 124 ±t 12$ 580 ±t 23T- D(Ca)
225.0 -- 17 12.0 -- 3.2$
+D 151.0 ± 17 90.3 ±t 8.8 89.4 ±t 7.0 179 ±t 8 571 ±- 29- D 15
44.0 ±t 9t 22.0 ±t 4.0t 73.0 -- 5.8 124 ±t 12$ 521 ±t 20§- D(Ca)
143.0 ±t 16 23.0 -- 5.1$
+D 138.0 -- 16 107.7 -- 9.0 83.2 ±- 5.8 155 ±- 13 487 -- 26-D 20
44.0 i11t 22.0 ±4i 4.3t 69.0 ± 7.1§ 132 ± 14§ 430 ± 12§-D(Ca) 99.0
± 17§ 23.0 ± 6.6$
+D 30.0 ± 4.2 127.6 ± 11.0 78.2 ± 6.0 55 ± 7 77 ±t 11-D PH 5.0
2.2$ 42.6 ± 7.1t 91.3 ± 8.3 40 ± 8 208 ± 15$-D(Ca) 4.8 ± 2.4$ 51.7
± 9.3t
* +D = 6 vitamin D-fed controls; -D = 5 vitamin D-deficient rats
on normal calcium intake; -D(Ca) = 4vitamin D-deficient rats on
high calcium intake.
t C = excretion during 5-hour control period; 5, 10, 15, 20 =
excretion during first 5, 10, 15, 20 hours of hormoneinfusion; and
PH = excretion during S hours after hormone infusion.
$ p < 0.001 when values (mean ± standard error) between +D
and - D animals are compared.§ p < 0.025 when values (mean ±
standard error) between +D and -D animals are compared.
for 5-hour periods before, during, and after hor-mone perfusion
in Figure 2 (columns 1 and 2).Also shown are the responses of four
sham-operated animals (Figure 2, columns 4 and 5),and the changes
in urinary calcium and phosphateexcretion on a high calcium, normal
phosphate' diet(Figure 2, column 3). Table II summarizes
theelectrolyte data and gives the results of the sta-tistical
evaluation of the differences between themean values for the
various 5-hour periods be-tween D-fed and D-deficient animals.
Table IIIshows the mean plasma calcium and phosphatevalues of
animals in each group before surgery,during the period of control
perfusion, and after12 hours of hormone infusion. All three
measure-ments could not be made in all animals in eachgroup.
Because of the small number of valuesin some groups, the mean and
range in each groupare recorded rather than the standard error.
The plasma values and the changes in electrolyteexcretion were
highly reproducible from one ani-mal to the next within a given
group but varied
considerably from group to group. Early in thecourse of this
project, a single bloodletting fre-quently led to a significant
decrease in the urinaryoutput during the next 0.5-hour period, but
theurinary output returned to the previous levelthereafter. After
further experience, it was pos-sible to obtain three blood samples
from a singleanimal within a 24-hour period without greatlyaltering
the rate of urine flow. The number ofmeasurements within each group
was too few toobtain precise statements of significance, but asseen
in Table III, the results were clear. Therewas no significant rise
in plasma calcium in theD-deficient animals of any group after
hormoneinfusion, although in each instance there was atendency for
the value to rise slightly. On theother hand, there was a rise in
plasma calcium inthe D-fed animals (Table III). The plasma
phos-phate decreased in all animals except in the intactD-deficient
ones (Table III).
The slight rise in plasma calcium seen in allD-deficient animals
was associated with definite
1958
-
PARATHYROIDHORMONEAND VITAMIN D
TABLE III
Plasma calcium and phosphate values in rats before
parathyroidectomy or thyroparathyroidectomy,during the control
infusion, and after 12 hours of hormone infusion
Plasma calcium Plasma P04
Status Vitamin D No. rats Pre-op.* Control inf.t PTHJ Pre-op.*
Control infQt PTHt
mg/100 ml mg/100 mlPTX + 4 11.1 i 0.4 8.4 ± 0.4 13.1 4L 0.6 11.3
i 0.3 10.2 ± 0.5 7.4 ± 0.4PTX - 4 6.0 ± 0.2 7.0 ± 0.4 8.1 i 0.3
11.4 i 0.3 10.8 ± 0.3 8.4 i 0.3
PTX§ - 4 9.6 ± 0.3 8.3 ± 0.3 8.9 i 0.4 9.3 i 0.4 8.9 i 0.3 6.2 ±
0.5High Ca
Intact + 3 11.4 A 0.3 10.2 i 0.3 12.2 i 0.3 11.3 ± 0.4 10.7 i
0.4 8.6 i 0.1Intact - 2 6.1 4± 0.3 7.1 i 0.2 7.2 ± 0.2 11.8 ± 0.3
10.8 ± 0.4 10.4 ± 0.3
TXPTXII + 4 10.8 i 0.3 8.8 ± 0.3 18.2 i 1.4 11.2 ± 0.4 11.0 ±
0.2 7.2 i 0.4TXPTXf - 4 6.1 i 0.2 9.2 ± 0.4 9.8 i 0.4 10.8 A 0.4
10.6 i 0.3 7.3 ± 0.5
* Values before surgery.t Values after surgery and at least 10
to 12 hours of perfusion with control solution.t Values after 12
hours of parathyroid hormone (PTH) infusion.§ Maintained on a high
calcium vitamin D-deficient diet.
Thyroparathyroidectomized.¶ These D-deficient animals were
perfused with a solution containing 25 M CaCl2 rather than the
usual 5 mM
concentration;
renal retention of calcium during hormone infu-sion and a slight
calcium diuresis after the hor-mone infusion stopped (Figure 2,
columns 2 and3). This pattern was also seen in the intactD-fed
animals, but in the D-fed parathyroidec-tomized animals the initial
retention of calciumwas followed by a marked diuresis.
It is noteworthy that the magnitude of the initial(first 5
hours) phosphaturia seen in the D-defi-cient animals (Figure 2,
column 2) was approxi-mately 50%o (p < 0.001) and the potassium
di-uresis 20%o of that seen in the D-fed animals(Figure 2, column
1). Conversely, the initialmagnesium retention was twice as great
in theD-deficient animals as in the D-fed (p < 0.025)(Figure 2,
columns 1 and 2). Also, the initialmagnesium retention in the D-fed
animals wasfollowed by a diuresis of magnesium during thelater
hours of hormone infusion, whereas this didnot occur in the
D-deficient animals although thelatter had a magnesium diuresis
after the cessationof hormone infusion.
If D-deficient animals were maintained on ahigh calcium diet
during the entire period beforestudy, their initial phosphaturia
during the first10 hours of hormone perfusion was
considerablygreater (p < 0.01) than that seen in
D-deficientanimals raised on a normal calcium diet (Figure2,
columns 2 and 3), and was approximately 80%o
of that seen in the D-fed animals (Figure 2, col-umns 1 and 3).
The results in Figure 2, column3 represent the mean values of four
animals.
Animals subjected to a sham operation ratherthan
parathyroidectomy responded differently thandid the
parathyroidectomized animals. Those fedvitamin D ('Figure 2, column
4) had qualitativelysimilar initial changes (compared to D-fed
para-thyroidectomized animals) in rates of electrolyteexcretion.
However, the magnitude of the phos-phaturia was significantly less
(p < 0.01) thanthat seen in parathyroidectomized animals, andthe
marked secondary rise in rate of calciumexcretion, normally seen in
the parathyroidec-tomized rats, was not seen in the
sham-operatedone. However, after the cessation of hormoneinfusion
in these latter animals, a striking calciumdiuresis was always
observed. In contrast, D-de-ficient sham-operated animals had no
significantchange in potassium or phosphate excretion duringhormone
infusion although the rates of excretionof sodium, calcium, and
magnesium all fell sig-nificantly (p < 0.01) and rose again only
uponcessation of hormone infusion.
The lack of both a rise in plasma calcium(Table III) and a
secondary calcium diuresis(Figures 1 and 2, columns 2 and 3) in the
D-defi-cient parathyroidectomized animals was inter-preted to mean
that the parathyroid hormone was
1959
-
C. ARNAUD, H. RASMUSSEN,AND C. ANAST
TABLE IV
Phosphate balances in D-deficient ratsgiven parathyroid
hormone*
Total Excessdecrease urinary
Rats No. Diet ECF HPO4t HPO4-
J.molesPTX 4 Normal Ca 24 150tPTX 3 High Ca 27 330tTXPTX 4
Normal Ca 27 128t
* Calculated from the data in Figure 2, columns 2 and 3;Figure
3, column 2; and Tables II and III.
t ECF = extracellular fluid.t Significantly greater (p <
0.001) than the total de-
crease in ECF phosphate.
unable to mobilize calcium from bone. If this wasthe case, it
could be argued that it would also beunable to mobilize phosphate
from bone. Thequestion then arose as to the source of the
urinaryphosphate seen in the D-deficient animals (Figure2, columns
2 and 3). From the data in Figure 2(columns 2 and 3) and Table III,
it was possibleto calculate the excess phosphate appearing in
theurine of the D-deficient animals during the first10 hours of
hormone infusion. This was done bysubtracting the rates during the
control periodfrom those seen in the first two 5-hour periodsof
hormone infusion. The difference was takenas a measure of phosphate
loss and recorded inTable IV as excess urinary HPO4=. The total
lossof phosphate from plasma and extracellular fluidswas calculated
from the differences in the plasmaphosphate concentrations seen
during the controlinfusion and after 12 hours of hormone
infusion(Table I), assuming the plasma and the extra-cellular fluid
volume to be 20 % of the bodyweight. These values are recorded in
Table IVas total decrease in extracellular fluid (ECF)HP04=. In
both instances, the phosphate appear-ing in the urine was
considerably in excess of thatwhich disappeared from the
extracellular fluids(p < 0.001). This was true even if the
totalECF volume was as great as 30% of the bodyweight.
Because of the recent evidence that thyrocalci-tonin suppresses
the action of parathyroid hor-mone upon bone resorption (15), it
was consideredimportant to determine whether thyrocalcitoninwas
involved in the altered responses of the D-de-ficient animals to
parathyroid hormone infusion.For this purpose, four D-deficient and
four D-fedanimals were thyroparathyroidectomized and per-
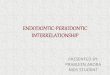
fused. The changes in plasma calcium and phos-phate and in the
rates of urinary excretion ofcalcium and phosphate are shown in
Figure 3 andTable III. In all the D-fed animals, the
initialphosphaturia was equal to that seen in the
para-thyroidectomized animals (compare Figure 3,column 1, with
Figure 2, column 1). However,there was no initial calcium retention
as seen inthe parathyroidectomized animals. Calcium ex-cretion rose
slightly during the first 6 hours andthen rapidly over the next 6.
This was associatedwith a striking rise in plasma calcium [from
8.8to 18.2 as compared to 8.4 to 13.1 in the para-
TIME, HOURSFIG. 3. CONCENTRATIONSOF CALCIUM AND PHOSPHATE
IN PLASMA AND RATES OF EXCRETION OF CALCIUM ANDPHOSPHATEIN THE
URINE BEFOREAND DURING THE INFU-SION OF PTH INTO
THYROPARATHYROIDECTOMIZEDD-FED(LEFTr) AND D-DEFICIENT (RIGHT) RATS.
There werefour animals in each group. The shaded areas along
thelower curves represent the range of values, and the heavyline
represents the mean. The first pair of plasma valuesin each case
represents the values obtained before theanimals were operated on.
The latter two pairs repre-sent values taken during the control
period and duringthe period of hormone infusion, respectively. Note
thatthe D-deficient animals were infused with a more con-centrated
solution of calcium chloride so that the concen-tration of calcium
in their plasma during the period ofcontrol infusion was nearly
identical to that seen in theD-fed controls.
1960
-
PARATHYROIDHORMONEAND VITAMIN D
thyroidectomized animal (Table III) ]. The ratesof excretion of
both calcium and phosphate fellduring the last 4 hours of
perfusion, but after16 to 20 hours of hormone infusion these
animalsdeveloped oliguria and died. The decline in cal-cium and
phosphate excretion coincided with theonset of oliguria. The
apparent cause of deathwas gross nephrocalcinosis. Because of this,
per-fusion could not be continued as long in theseanimals.
In contrast to the D-fed animals, the responsesof
thyroparathyroidectomized D-deficient animalswere not very
different from those seen in para-thyroidectomized D-deficient
animals (compareFigure 3, column 2, with Figure 2, column 2). Inan
attempt to make the experimental situation be-tween D-fed and
D-deficient animals as comparableas possible, we infused the
thyroparathyroidecto-mized D-deficient animals with a solution
con-taining 25 rather than 5 mMCaCl2. This wassufficient to raise
their plasma calcium concentra-tions to values slightly greater
than those of theD-fed animals (Table III and Figure 3). Thisled to
a much higher rate of calcium excretion andto the complete
disappearance of phosphate fromthe urine during the control period
(Figure 3).In spite of the high rate of urinary calcium excre-tion,
the animals were in significant positive cal-cium balance,
approximately 60 umoles per hour.Parathyroid hormone infusion led
to a prompt andstriking fall in urinary calcium, which
remainedbelow control values throughout the period of hor-mone
infusion. Phosphaturia was also observedand was approximately 40%o
of that seen initiallyin the D-fed controls (Figure 3). The total
ex-cess phosphate in the urine was significantlygreater (p <
0.001) than that which disappearedfrom the ECF (Table IV). The
plasma calciumrose only slightly, 9.2 to 9.8 mg per 100 ml,
ascompared to the striking rise, 8.8 to 18.2, seen inthe D-fed
animals. In spite of the high initial ratesof calcium infusion and
excretion, these animals didnot develop nephrocalcinosis.
Discussion
The present results extend our previous obser-vations (6) and
those of Harrison and Harrison(7). In D-deficient rats with intact
parathyroidglands, the injection (6, 7) or infusion of para-thyroid
hormone (Figure 2, column 5, and Table
II) led to no change in plasma calcium or phos-phate and no
change in the urinary excretion ofphosphate. However (Figure 2,
column 5), asignificant (p < 0.025) decrease in magnesium
andsodium and a slight decrease in calcium excretionwere observed.
Removal of the parathyroid orboth thyroid and parathyroid glands of
these ani-mals altered this pattern of response. Plasma phos-phate
fell after hormone infusion (Table III), andphosphaturia as well as
magnesium and calciumretention occurred (Figure 2, columns 2 and
3;and Figure 3, column 2). Plasma calcium roseslightly, but in no
instance was this significant(p < 0.2). This slight rise in
plasma calcium wasthought to be a consequence of renal retention
ofcalcium. Furthermore, the responses of the
thyro-parathyroidectomized D-deficient animals (Figure3, column 2)
indicate that the lack of calcium mo-bilization during hormone
infusion was not dueto the presence of excess thyrocalcitonin. This
isin sharp contrast to the results of hormone perfu-sion in D-fed
animals. The presence of the thy-roid gland altered the pattern of
response of thisgroup (compare Figure 2, column 1, and Figure
3,column 1). In the absence of endogenous thyro-calcitonin,
parathyroid hormone led to a morerapid mobilization of calcium from
bone. Duringthe same period, the infusion of hormone
intoD-deficient animals maintained on a much higherrate of calcium
infusion led to no significant hy-percalcemia, but to a striking
decrease in the rateof urinary calcium excretion (Figure 3).
The major differences in the responses of
theparathyroidectomized D-deficient and D-fed ratsto the long-term
infusion of parathyroid hormoneare the less marked initial
phosphate and potassiumdiuresis, the lack of delayed
hypercalciuria, andthe poorly sustained phosphaturia in the
D-defi-cient group (Figures 1 and 2). The latter twofindings
probably reflect the failure of the hormoneto induce the
mobilization of calcium and phos-phate from bone in the absence of
vitamin D. Ifthis conclusion is accepted, then the data shown
inTable IV indicate that parathyroid hormone mo-bilizes phosphate
from a source other than thebone and extracellular fluids,
presumably the in-tracellular fluids. This in turn implies that
para-thyroid hormone alters intracellular electrolyteconcentrations
as well as those in extracellularfluids, a point that has been
discussed previously
1961
-
C. ARNAUD, H. RASMUSSEN,AND C. ANAST
in relation to the effects of this hormone on iso-lated
mitochondria (1).
The less marked initial phosphaturia seen inthe D-deficient
animals (Figure 2, column 2 vs.column 1; and Figure 3) is difficult
to explain.There are several possibilities. It is conceivablethat
the rats employed in these studies were notadequately depleted of
vitamin D and that thisvitamin is necessary for the action of
parathyroidhormone on the renal tubule as well as on bone.However,
if one considers the total response ofthe tubule to hormone
infusion, then it is apparentthat the quantitative changes in
excretion of so-dium and calcium were similar in D-fed and
D-de-ficient parathyroidectomized animals; that thechanges in
magnesium excretion were greater(p < 0.025) in the D-deficient
animals (Figure 2,columns 1 and 2); and that even in
D-deficientsham-operated animals (Figure 2, column 5) achange in
magnesium and calcium excretion wasobserved. Thus, by some
criteria, the kidney ofthe D-deficient animal responds to
parathyroidhormone as well as or better than that of the
D-fedanimal, but by others it responds less well.
One possibility that may account for the differ-ences in
phosphate excretion in the differentgroups of animals is that they
had varying de-grees of secondary hyperparathyroidism beforethese
experiments were undertaken; it is possiblethat this altered the
concentrations of intracellularelectrolytes and consequently renal
responses.There is increasing evidence (6, 16, 17) that
sig-nificant hyperparathyroidism exists in vitaminD-deficient rats
maintained on a normal calciumintake. This appears to be a
consequence of thehypocalcemia that results from the vitamin
defi-ciency (6, 17) and can be prevented in large partby putting
these animals on high calcium intakes(6, 17). In the present
context, perhaps the mostimportant consequence of chronic secondary
hy-perparathyroidism is possible depletion of intra-cellular
phosphate stores. It is important to pointout that, although our
animals were studied aftertheir parathyroid glands had been
removed, theyreceived no phosphate after this surgery and
hencewould not have repleted tissue stores of this sub-stance. The
most obvious difference betweenD-deficient animals on a normal and
on a highcalcium intake (Figure 2, columns 2 and 3; andTable III)
is that the former have low levels of
plasma calcium and the latter have high levels.Thus, the latter
would not have secondary hyper-parathyroidism [see also (17)], and
the responseof these animals measured in terms of
phosphateexcretion (Figure 2, column 3; and Table II)and plasma
phosphate (Table III) was similar tothat seen in D-fed controls
(Figure 2, column 1).On the other hand, the D-deficient animals
withhypocalcemia undoubtedly had secondary hyper-parathyroidism
with resultant changes in phos-phate metabolism (6), and their
response mea-sured as phosphate excretion (Figure 2, column 2)was
significantly less than that of the D-fed con-trols. This
difference would account for the factthat parathyroid hormone
mobilized less totalphosphate in the D-deficient animals on a
normalcalcium intake than it did in the D-deficient animalson a
high calcium intake (Table IV). The ac-ceptance of this proposal
must await the demon-stration that parathyroid hormone alters
intra-cellular phosphate concentrations. These studiesare in
progress.
The results with the group of D-deficient ani-mals fed a high
calcium diet (Figure 2, column 3;and Table III) were of importance
for anotherreason. These animals had the same plasma cal-cium
values as the D-fed animals (Table III) dur-ing the period of
control infusion (before hormoneinfusion) and the same degree of
calcium retentionduring this period (Table I). Nevertheless,
theinfusion of hormone into these D-deficient animalsdid not lead
to significant rise in plasma calcium(Table III) or delayed
hypercalciuria as seen inthe D-fed animals (Figure 2, columns 3 and
1).Also the fall in plasma phosphate concentrationwas as great in
this group of animals as that seenin the D-fed ones (2.8 vs. 2.7,
Table III). Thus,in terms of initial changes in phosphate
metabo-lism, the two groups were nearly identical; inspite of this,
parathyroid hormone did not mobilizecalcium from bone. These data
constitute thestrongest argument in support of our previousthesis
(6) that parathyroid hormone is unable tomobilize calcium from bone
in D-deficient ratsbut is still able to exert its usual effects on
renalfunction.
This thesis is also supported by the recent stud-ies of the
effect of inhibitors of RNAand proteinsynthesis upon the response
of rats to parathyroidhormone and vitamin D (8, 18, 19). The
infu-
1962
-
PARATHYROIDHORMONEAND VITAMIN D
sion of parathyroid hormone into an actinomycin-treated rat
leads to the same pattern of urinaryelectrolyte changes (8) as seen
in the D-deficientrat (Figures 2 and 3), that is, the early
renalresponse is normal, but the secondary changes dueto
mobilization of calcium and phosphate from boneare absent.
Similarly, Zull, Czarnowska-Misztal,and DeLuca (18) and Norman (19)
have shownthat prior treatment with actinomycin D blocks thenormal
response of vitamin D-deficient rats to theadministration of
vitamin D.
Thus, evidence gathered by several differentmeans leads to the
conclusion that vitamin D isnecessary for the expression of some,
but not all,effects of parathyroid hormone. The problem
thatdevelops is that of accounting for the divergentviews of others
(4, 5, 7, 20). There is no basicdisagreement between our data and
those of Har-rison and Harrison (7). The important point isthat, in
a D-deficient rat, exogenous parathyroidhormone has little
detectable influence on phos-phate metabolism because of high
levels of en-dogenous hormone, which are already exerting anearly
maximal effect. Only by removing theparathyroid glands is it
possible to demonstrate aneed for, or a response to, exogenous
hormone(Figure 2). Other studies in rodents (5, 20),which have led
to results different from ours andthose of Harrison and Harrison,
can be questionedon their lack of sufficient evidence that the
ani-mals involved were completely D deficient. Themost serious
challenge to our thesis comes from thework of Ney and associates
(4). These authorsconcluded, on the basis of the response of
D-defi-cient puppies to parathyroidectomy and to para-thyroid
extract, that parathyroid hormone exertsits usual effects on bone
even in D deficiency.One possible explanation is that the nature of
thehormone-vitamin relationship described in thepresent report is
unique to the rat. A more likelyexplanation is that the dogs
studied by Ney andco-workers did not have as severe a degree ofD
deficiency as that developd by the rats. One ofthe dogs with the
most marked hypocalcemia hadno change in plasma calcium after
parathyroidec-tomy, and several others had minimal changesboth
after operation and after the subsequent in-jection of parathyroid
extract. In fact, there wasdirect correlation between the initial
level ofplasma calcium and the fall observed after parathy-
roidectomy (omitting animal T782, which was mostunusual), and
all animals were initially hypocal-cemic. These results could be
accounted for ifthe animals studied had varying degrees of D
de-ficiency, and they are similar to our previous ob-servations in
the rat (6).
Unfortunately, there is as yet no simple methodby which the
degree of D deficiency can be assessedin experimental animals;
hence, it is not an easymatter to resolve all controversy.
Nevertheless,in the species in which the degree of deficiencycan be
best controlled, the rat, it seems clear thatvitamin D is necessary
for physiologic concen-trations of parathyroid hormone to mobilize
cal-cium and phosphate from bone. On the otherhand, there appears
to be no vitamin D require-ment for the expression of parathyroid
hormoneaction at the level of the renal tubule.
Summary
The response of the D-deficient parathyroidec-tomized rat to the
infusion of parathyroid hormoneis different from that of a D-fed
control. Bothexhibited qualitatively similar initial changes
inplasma phosphate and in the urinary excretionof calcium,
phosphate, magnesium, sodium, andpotassium, but in the D-deficient
animals sus-tained phosphaturia and secondary hypercalciuriaand
hypercalcemia did not develop as they did inthe D-fed animal.
Initial phosphate excretion was less and initialmagnesium
retention greater in D-deficient animalsraised on a normal calcium
intake. However,D-deficient animals raised on a high calcium
in-take had nearly the same initial values of plasmacalcium and
changes in plasma and urinary phos-phate after hormone infusion as
D-fed animalsraised on a normal calcium intake. In spite ofthis,
the D-deficient animals had no rise in eitherplasma or urinary
calcium.
Removal of the thyroid gland did not greatlyalter the response
of the D-deficient rat to para-thyroid hormone, but a more
immediate andmarked calcium diuresis and hypercalcemia wereobserved
in the D-fed animal.
We concluded that vitamin D is necessary forphysiologic
concentrations of parathyroid hormoneto mobilize calcium and
phosphate from bone butnot for the hormone to act on the renal
tubule.
1963
-
C. ARNAUD, H. RASMUSSEN,AND C. ANAST
AcknowledgmentsWeare indebted to Dr. Maurice Pechet for his
advice
in regard to the perfusion technique. Mr. CharlesHawker, Miss
Berit Johannson, and Miss Elizabeth Mid-dleton all rendered
valuable assistance.
References1. Rasmussen, H., and H. F. DeLuca. Calcium homeo-
stasis. Ergebn. Physiol. 1963, 53, 108.2. Shelling, D. H. The
Parathyroids in Health and
Disease. St. Louis, C. V. Mosby, 1935.3. Harrison, H. C., H. E.
Harrison, and E. A. Park.
Vitamin D and citrate metabolism: effect of vita-min D in rats
fed diets adequate in both calciumand phosphorus. Amer. J. Physiol.
1958, 192, 432.
4. Ney, R. L., W. Y. W. Au, G. Kelly, I. Radde, andF. C.
Bartter. Action of parathyroid hormone inthe vitamin D-deficient
dog. J. clin. Invest. 1965,44, 2003.
5. Nichols, G., Jr., S. Schartum, and G. M. Vaes. Someeffects of
vitamin D and parathyroid hormone onthe calcium and phosphorus
metabolism of bonein vitro. Acta physiol. scand. 1963, 57, 51.
6. Rasmussen, H., H. DeLuca, C. Arnaud, C. Hawker,and M. von
Stedingk. The relationship betweenvitamin D and parathyroid
hormone. J. clin. In-vest. 1963, 42, 1940.
7. Harrison, H. E., and H. C. Harrison. The interac-tion of
vitamin D and parathyroid hormone oncalcium, phosphorus and
magnesium homeostasisin the rat. Metabolism 1964, 13, 952.
8. Rasmussen, H., C. Arnaud, and C. Hawker. Actino-mycin D and
the response to parathyroid hormone.Science 1964, 144, 1019.
9. Steenbock, H., and D. C. Herting. Vitamin D andgrowth. J.
Nutr. 1955, 57, 449.
10. Willis, J. B. Determination of calcium and mag-nesium in
urine by atomic absorption spectroscopy.Analyt. Chem. 1961, 33,
556.
11. Roe, J. H., J. H. Epstein, and N. P. Goldstein. Aphotometric
method for the determination of inu-lin in plasma and urine. J.
biol. Chem. 1949, 178,839.
12. Cotlove, E. Simple tail vein infusion method for re-nal
clearance measurements in the rat. J. appl.Physiol. 1961, 16,
764.
13. Snedecor, G. W. Statistical Methods. Ames, Iowa,Iowa State
College Press, 1956.
14. Hawker, C. D., J. D. Glass, and H. Rasmussen. Fur-ther
studies on the isolation and characterizationof parathyroid
polypeptides. Biochemistry 1966,5, 344.
15. Friedman, J., and L. G. Raisz. Thyrocalcitonin in-hibition
of bone resorption in tissue culture. Sci-ence 1965, 150, 1465.
16. Crawford, J. D., D. Gribetz, W. C. Diner, P. Hurst,and B.
Castleman. The influence of vitamin D onparathyroid activity and
the metabolism of calciumand citrate during calcium deprivation.
Endo-crinology 1957, 61, 59.
17. Au, W. Y. W., and L. G. Raisz. Effect of vitamin Dand
dietary calcium on parathyroid activity. Amer.J. Physiol. 1965,
209, 637.
18. Zull, J. E., M. Czarnowska-Misztal, and H. F. De-Luca. On
the relationship between vitamin D ac-tion and
actinomycin-sensitive processes. Proc.nat. Acad. Sci. (Wash.) 1966,
55, 177.
19. Norman, A. W. Actinomcyin D and the response tovitamin D.
Science 1965, 149, 184.
20. Toverud, S. U. The effect of parathyroid hormoneand vitamin
D on serum calcium in rats. Actaphysiol. scand. 1964, 62, 391.
1964