Embed Size (px)
Citation preview

Interprofessional Learning Unit 2
Group Number: 87
Confidentiality has been respected throughout this work and no names of people or places have been included This report is entirely our own work Group 87 confirm that we fully understand that this report remains the property of the host organisation and we may not personally/professionally share or use any part of it, without the express permission of the host organisation. We appreciate that no member should retain copies subsequent to successful completion of IPLU2/IPLU3 and if we wish to evidence our success we know we may use/refer to the Group Project Assessment Report. Indicate Word Count: 3086 Executive summary: 464

Executive summary 1) Background
A Preceptorship programme is designed to aid and support the transition from
student to fully competent professional. It involves a newly qualified registrant
(NQR) within many areas of healthcare being assigned a “mentor” or
preceptor who will monitor and assist them to grow in professional and clinical
confidence thus providing the NQR with stability and better patient care. The
aim was to decipher whether the minimum corporate standards for
preceptorship were being met across all healthcare profession throughout the
acute trust.
An audit is carried out as a means of measuring the levels of achievement in
relation to the standards set out. A strict audit cycle is followed to ensure that
all areas are covered. The audit was carried out ensuring data protection and
confidentiality was maintained at all times.
2) Methodology
A questionnaire was designed in order to quantify how the level of
preceptorship in practice met the minimum corporate standards. A sample
size of 55 NQRs was used. A pilot study was carried out to ensure that the
questionnaire used was an unbiased analysis and as a result led to some
rewording of questions. The questionnaire was distributed. All quantitative
data was visually represented using charts and qualitative data was
thematically analysed.
3) Results
The results revealed that NQRs were not always beginning their training at
the start of their employment, although most had been assigned a preceptor.
Some did not have a preceptor at all or their preceptor had left. The majority
received intensive training in their first week; more than half thought that they
did not receive the sufficient study days required. Those that did thought it
was mainly constructed through formative teaching, most agreed that they
had competencies to complete and over half said they did not have regular

3
meetings with their preceptor. Of those eligible for the six month appraisal,
lest than half said this had occurred. The majority of preceptors were rated
better than satisfactory. The Flying Start scheme received positive comments.
4) Discussion
It is a concern that some NQRs were not commencing the preceptorship
programme immediately, causing them to be unaided during the significant
first weeks; some were without a preceptor at all. This could be due to the
NQRs being trained within the trust and already deemed competent. Although
most disagreed that they were receiving the full allocated study time, they
may not have been aware of how study days could be constituted.
We recommend that all NQRs are assigned a preceptor regardless of whether
or not employment starts within the annual recruitment period. All NQRs and
preceptors need to be made aware of the corporate standards.
For a future re audit it would be beneficial to break down the analysis by
divisions to illustrate differences and preceptor programme strategies.
4
Contents
1. Introduction
1.1 Background 5
1.2 Aims and objectives 5
1.3 Understanding the audit process 6
1.4 Steps of the audit 7
1.5 Ethical considerations 9
1.6 Understanding audit standards 10
2. Methodology
2.1 Data collection 11
2.2 Sample size 11
2.3 Pilot study 11
2.4 Data analysis 11
3. Results 12
4. Discussion
4.1 Conclusion 18
4.2 Recommendations 20
4.3 Action planning 21
5. References 23
6. Appendices
6.1 Minimum corporate standards 24
6.2 Questionnaire 25
5
1. Introduction
1.1 Background
Preceptorship was introduced into clinical practice following the outcome of a
nurse education review, resulting in Project 2000 in the 1990s (DoH, 2009).
Preceptorship is a programme designed for newly qualified registrants (NQRs)
in Band 5. The aim of the programme is to develop competence and
confidence within the professional role, in order to benefit the patient and
service as a whole (Ashurst, 2008). A support system is provided to enable
NQRs to further develop skills in the first few months of employment. NQRs
are supported whilst achieving their relevant competencies, enabling faster
progression to the next pay band (DoH, 2004).
Since 2008 there has been a push within the health service to develop and
understand the benefits of Preceptorship for NQRs (DoH, 2008). The Acute
Trust we audited set out “Minimum corporate standards” (see appendix 1),
outlining the requirements for their preceptorship programme. The standards
were designed to enable NQRs to have an understanding of the education
and support they should receive and competencies they need to achieve.
Within the minimum corporate standards there was the implementation of the
pilot scheme “Flying Start”. This is an online scheme which is designed to aid
the preceptorship programme and provide a constant form of support.
1.2 Aims and objectives
The aim of the audit was to find out whether NQRs, including nurses and
allied health professionals, were on a preceptorship programme which met
the minimum corporate standards set by the Acute Trust.
6
This was a new audit with a key objective to review the preceptorship
programme and make appropriate recommendations for future practice based
on analysis of our findings.
1.3 Understanding the Audit Process
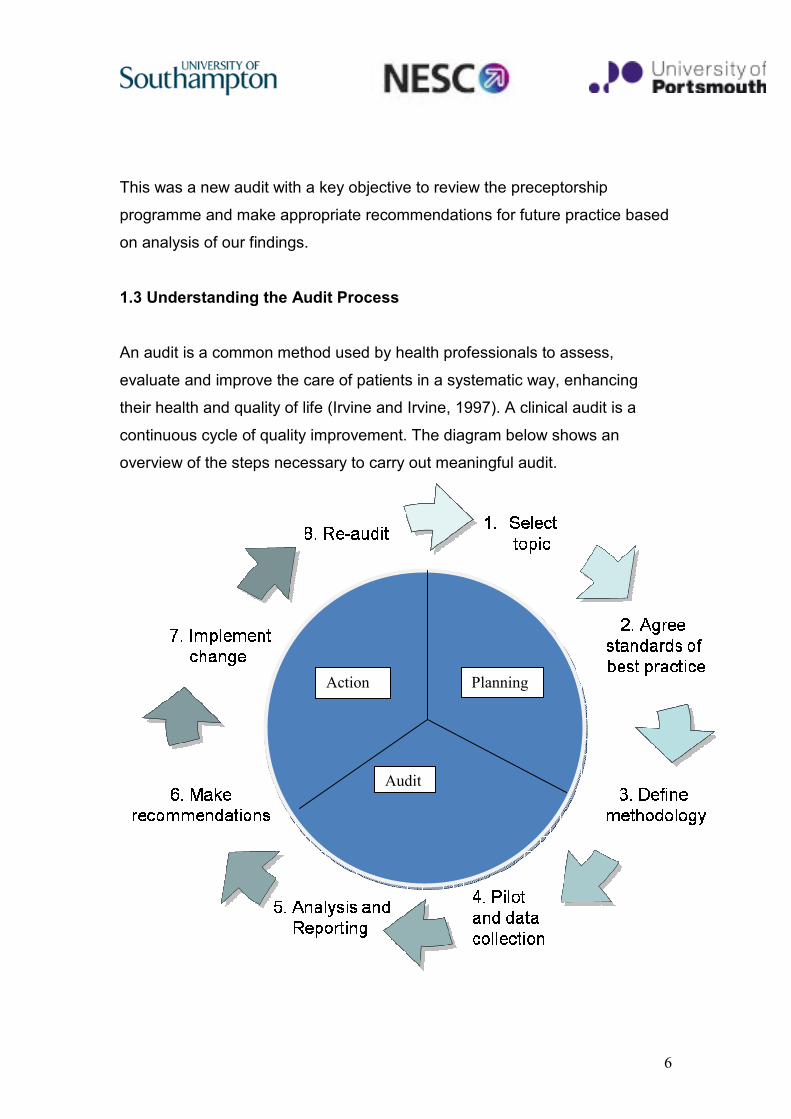
An audit is a common method used by health professionals to assess,
evaluate and improve the care of patients in a systematic way, enhancing
their health and quality of life (Irvine and Irvine, 1997). A clinical audit is a
continuous cycle of quality improvement. The diagram below shows an
overview of the steps necessary to carry out meaningful audit.
Action
Audit
Planning

7
Figure 1: The Audit Cycle (from East Kent Clinical Audit Service; available from http://www.ekclinicalauditservice.nhs.uk)
1.4 Steps of the audit
Step 1:
Audit topic selected: Minimum Corporate Standards Preceptorship
Programme.
Step 2:
Agreed standards of best practice: Minimum corporate standards produced by
the acute trust incorporating a multi disciplinary approach. (See appendix 1)
Step 3:
Methodology: Audit tool designed to obtain quantitative and qualitative data
on how the preceptorship programme is being delivered across the acute
trust. The tool aims to investigate the extent to which the minimum corporate
standards are being met. (See appendix 2)
Step 4:
Pilot study and Data Collection: A pilot study was completed using a sample
size of 8 NQRs to test the validity of the audit tool. Data was collected by
distributing questionnaires to different ward settings over a period of four
days.
Step 5:

8
The data obtained was analysed in Excel and presented in graph form. The
qualitative data was interpreted by the audit team.
Step 6:
Recommendations: not all standards were met and future recommendations,
include more study days and a designated member of staff to oversee the
preceptorship programme.
Due to time constraints, step 7 (implementing change) and step 8 ( re-audit),
were not carried out but it is recommended this is completed in the future,
continuing the audit cycle.
NICE guidelines state that audit is important for improving patient care and
outcomes through a systematic review of care against explicit criteria. In
addition, audit should promote implementation of change (NICE, 2002).
Clinical audit needs:
• Evidence based standards
• A team/ multi-disciplinary approach
• Monitoring of practice
• Commitment to change
Audit standards are to ensure health professionals participate in regular
clinical audits and review services to ensure best practice and patient care
delivery is improved, raising standards (Clinical Audit Support Centre, 2010).
The audit followed the steps outlined in the cycle above, excluding the re-
audit, which is a step that we would recommend is carried out in the future.
9
1.5 Ethical Considerations
This audit was undertaken with consideration to data protection and
confidentiality to maintain participants’ anonymity. This was necessary to
ensure that participants would feel comfortable divulging what could be
considered sensitive information to us.
The NHS Confidentiality Code of Practice (DoH, 2003) outlines a
confidentiality model based on four key principles: Protect, Inform, Provide
Choice and Improve. Our investigation adhered to these principles as follows:
Protect: Data was stored in accordance with The Data Protection Act (1998)
and all data was destroyed after analysis. The location and name of the trust
in which our audit took place was removed from any written work, to ensure
maximum protection and confidentiality.
Inform: All participants were informed of what we were auditing and why we
were doing it.
Provide Choice: To ensure confidentiality, data collection was anonymous
and participants had the right to refuse to complete the questionnaire.
Improve: We performed a pilot study to test our method of data collection.
This resulted in a few minor changes which improved confidentiality
throughout the questionnaire.
Furthermore our audit met the criteria of SMART guidelines, whereby the
audit was specific to preceptorship. Our results were measurable and
achievable through a questionnaire, carried out in a realistic and timely
manner.

10
1.6 Understanding Audit Standards
The minimum corporate standards (See Appendix 1) were set out by the
Acute Trust in 2009 and each Division was invited to apply for funds to
develop a preceptorship programme.
The minimum standards were developed in accordance with
recommendations arising from Lord Darzi’s report “High Quality Care for All”
(DoH, 2008). The report identifies the importance of improving NHS education
and training for both service users and healthcare professionals.
Preceptorship programmes are an element of education where NQRs are
supported through consistent opportunities to update and develop their skills.
The report also states investment funds will be increased with regards to
preceptorship to ensure NQRs can learn and be supported by senior
colleagues.
11
2. Methodology
2.1 Data Collection
To investigate how the current preceptorship programme in practice
compares to corporate minimum standards, a questionnaire was designed to
obtain quantitative and qualitative data. This method of data collection would
provide results, achieving our aims and providing further recommendations to
improve the preceptorship programme.
2.2 Sample Size
The total sample size was 55 NQRs, 3 of which were on the Flying Start
programme, including nurses, midwives, occupational therapists,
physiotherapists and dieticians. Within the trust, 232 post qualified
professions had been employed. A random sample size of 55 was seen as
sufficient due to time available and convenience.
2.3 Pilot Study:
A pilot study of our questionnaire was given to 8 NQRs to check the feasibility
and to improve the research design. From this study a few questions were
altered, in order to maintain confidentiality and improve specificity.
The questionnaires (see appendix 2), consisting of 8closed and 3 open
questions, were distributed by the audit team to different professions in
different ward areas over a period of 4 days. The NQRs self completed the
questionnaire to prevent researcher bias. Aware of time constraints our
questionnaire was concise and clear with no leading questions.
2.4 Data analysis
Data was analysed using Excel. Quantitative data was graphed to provide a
visual representation of our findings. Thematic analysis was carried out on the
qualitative data.
12
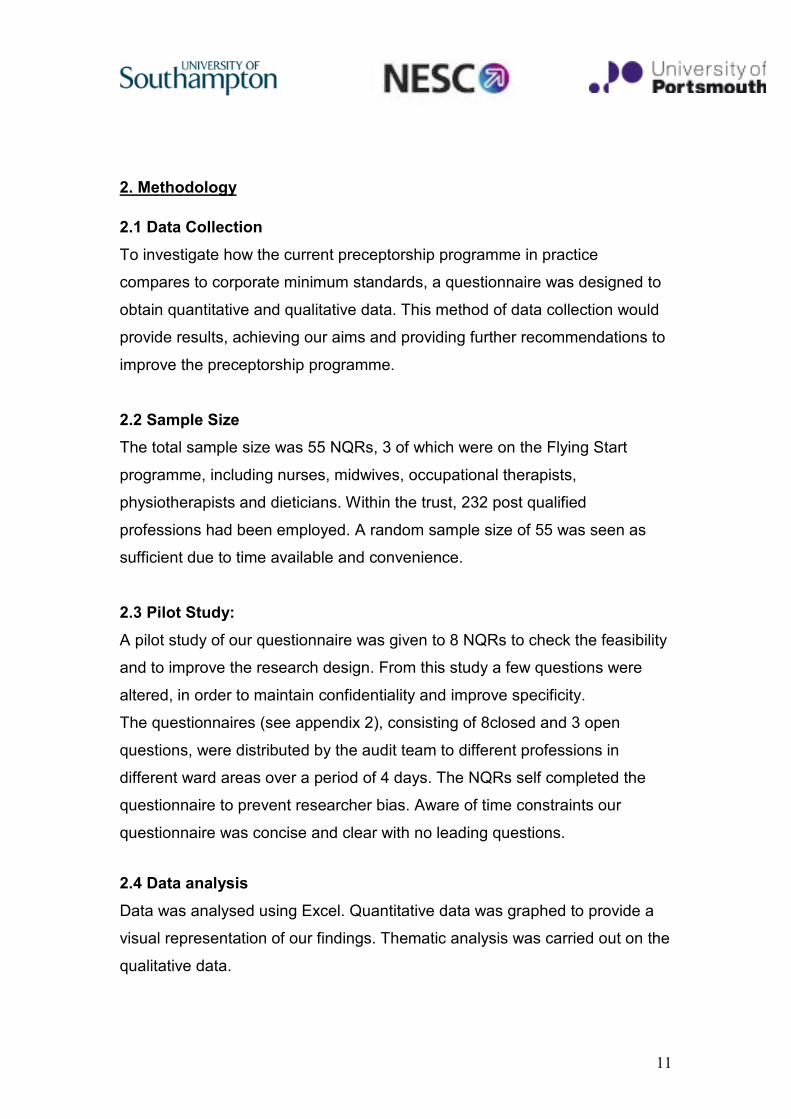
3. Results
The results were compiled from the audit tool, demonstrating the views of
NQRs from a range of professions.
The pie chart above shows the proportion of each profession completing the
audit tool.
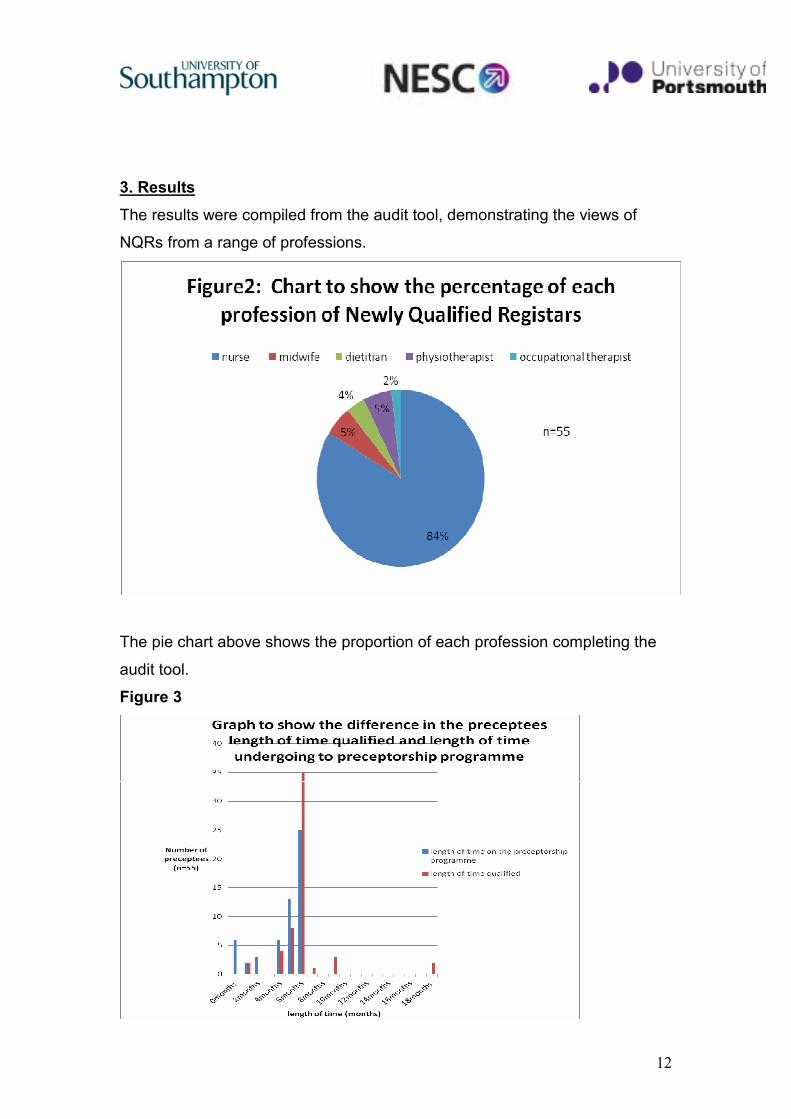
Figure 3
13
This graph compares the length of time since qualifying (and duration of
employment) against the amount of time participants have been undergoing
preceptorship. It clearly demonstrates that although people are receiving
preceptorship, the length of time does not match their time qualified. 74% of
NQRs have been working for a 6 month period, with only 45% of these having
been on the preceptorship programme for the required 6 months. Analysis of
written comments revealed this was due to NQRs not always beginning their
preceptorship at time of qualification/employment. Many said they worked
unaided for the first month.
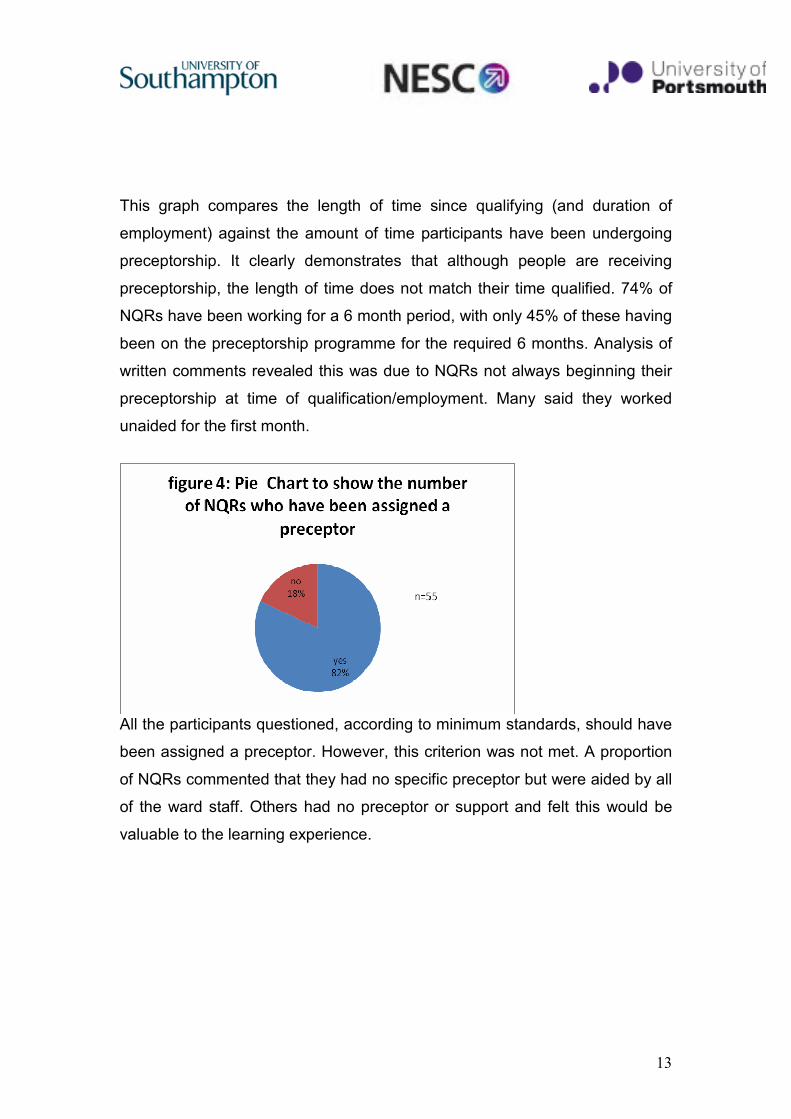
All the participants questioned, according to minimum standards, should have
been assigned a preceptor. However, this criterion was not met. A proportion
of NQRs commented that they had no specific preceptor but were aided by all
of the ward staff. Others had no preceptor or support and felt this would be
valuable to the learning experience.
14
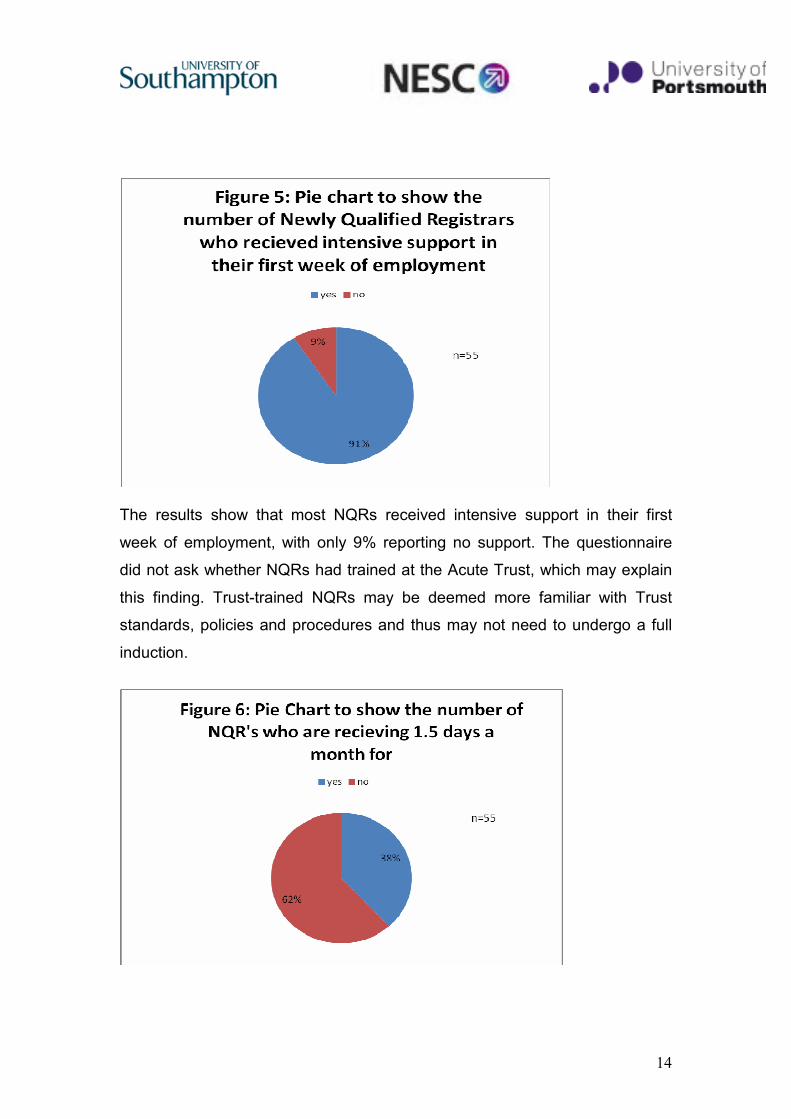
The results show that most NQRs received intensive support in their first
week of employment, with only 9% reporting no support. The questionnaire
did not ask whether NQRs had trained at the Acute Trust, which may explain
this finding. Trust-trained NQRs may be deemed more familiar with Trust
standards, policies and procedures and thus may not need to undergo a full
induction.
15
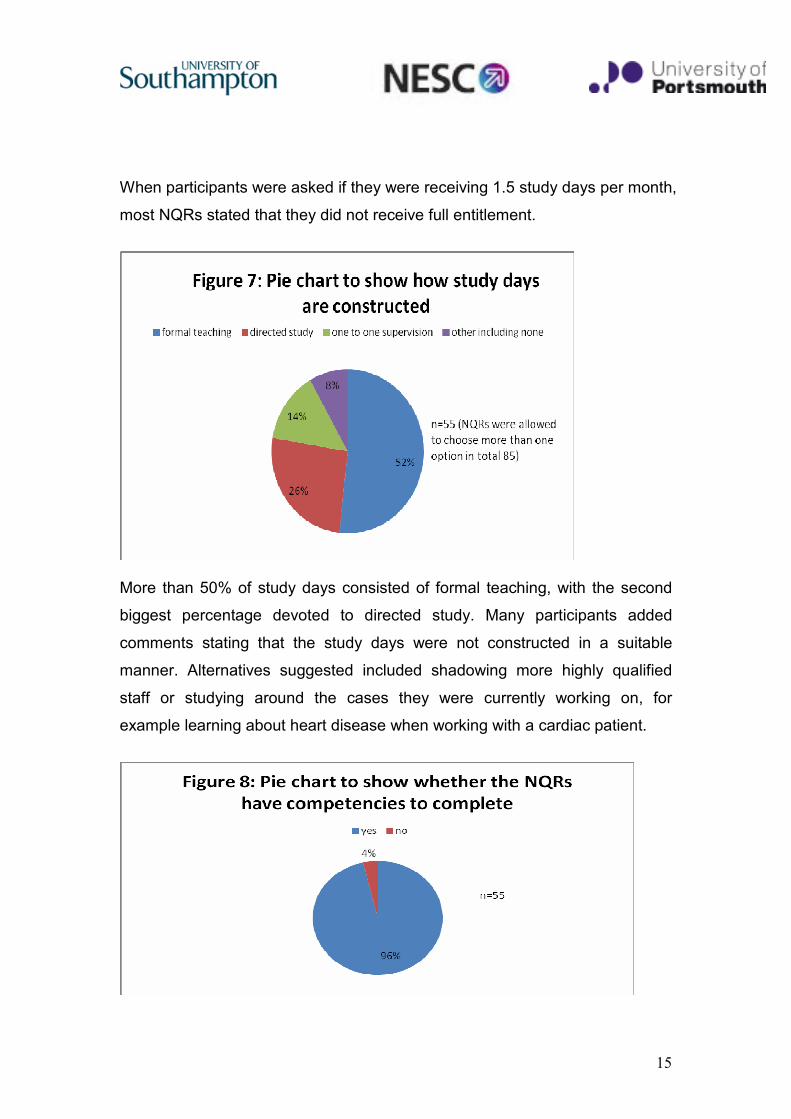
When participants were asked if they were receiving 1.5 study days per month,
most NQRs stated that they did not receive full entitlement.
More than 50% of study days consisted of formal teaching, with the second
biggest percentage devoted to directed study. Many participants added
comments stating that the study days were not constructed in a suitable
manner. Alternatives suggested included shadowing more highly qualified
staff or studying around the cases they were currently working on, for
example learning about heart disease when working with a cardiac patient.
16
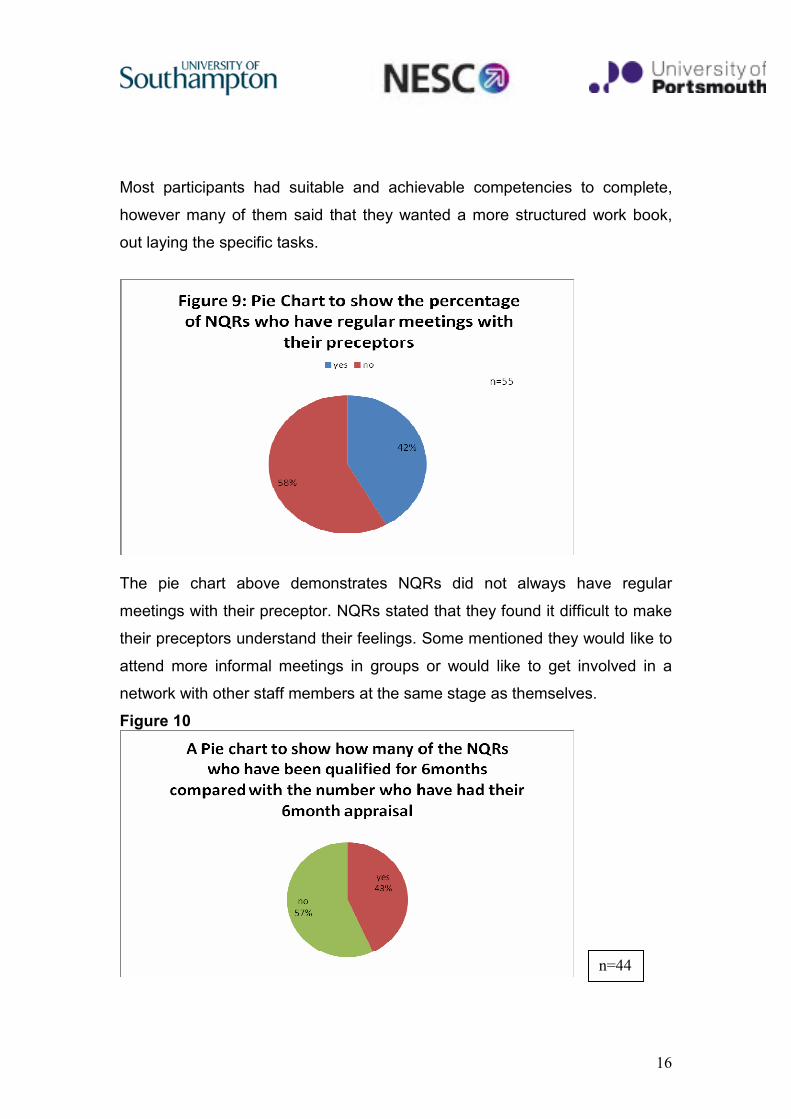
Most participants had suitable and achievable competencies to complete,
however many of them said that they wanted a more structured work book,
out laying the specific tasks.
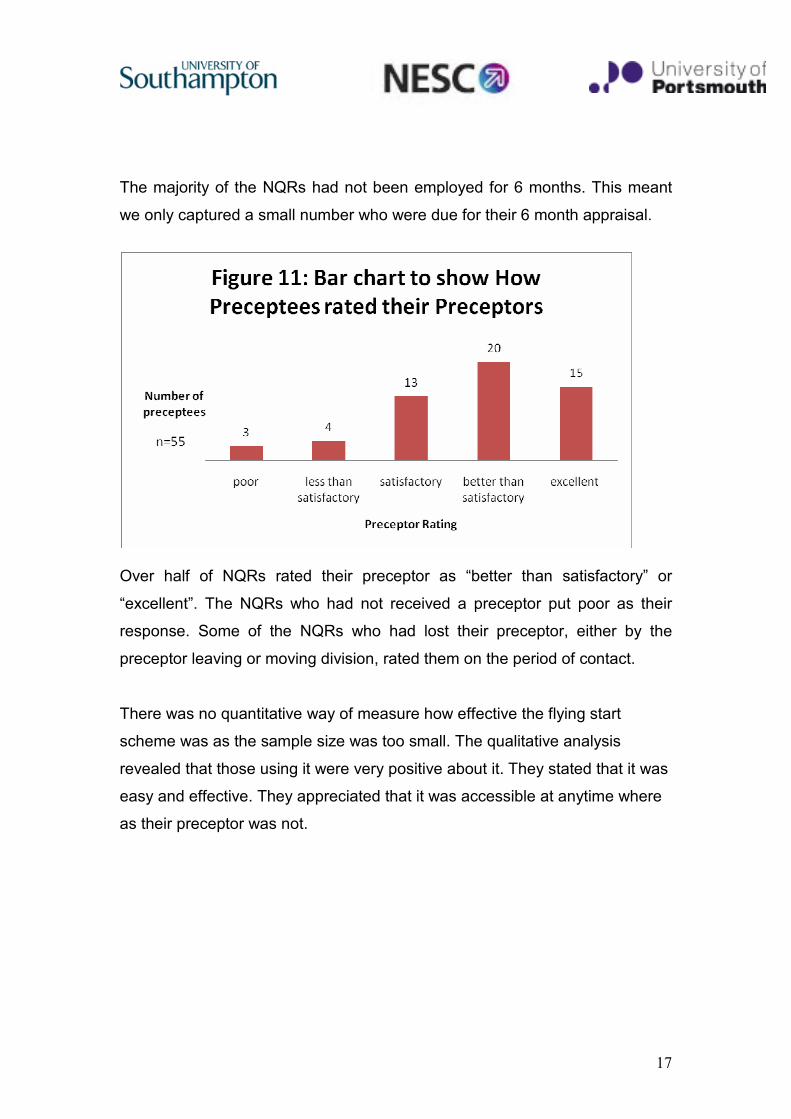
The pie chart above demonstrates NQRs did not always have regular
meetings with their preceptor. NQRs stated that they found it difficult to make
their preceptors understand their feelings. Some mentioned they would like to
attend more informal meetings in groups or would like to get involved in a
network with other staff members at the same stage as themselves.
Figure 10
n=44
17
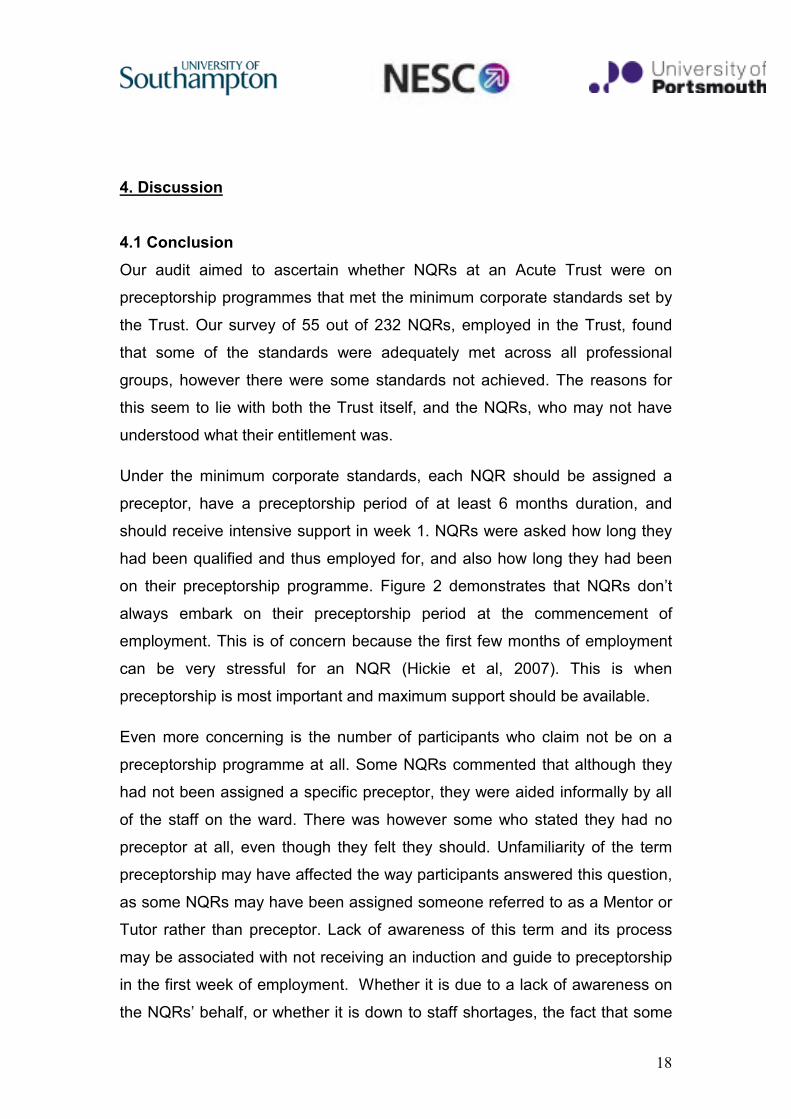
The majority of the NQRs had not been employed for 6 months. This meant
we only captured a small number who were due for their 6 month appraisal.
Over half of NQRs rated their preceptor as “better than satisfactory” or
“excellent”. The NQRs who had not received a preceptor put poor as their
response. Some of the NQRs who had lost their preceptor, either by the
preceptor leaving or moving division, rated them on the period of contact.
There was no quantitative way of measure how effective the flying start
scheme was as the sample size was too small. The qualitative analysis
revealed that those using it were very positive about it. They stated that it was
easy and effective. They appreciated that it was accessible at anytime where
as their preceptor was not.
18
4. Discussion
4.1 Conclusion
Our audit aimed to ascertain whether NQRs at an Acute Trust were on
preceptorship programmes that met the minimum corporate standards set by
the Trust. Our survey of 55 out of 232 NQRs, employed in the Trust, found
that some of the standards were adequately met across all professional
groups, however there were some standards not achieved. The reasons for
this seem to lie with both the Trust itself, and the NQRs, who may not have
understood what their entitlement was.
Under the minimum corporate standards, each NQR should be assigned a
preceptor, have a preceptorship period of at least 6 months duration, and
should receive intensive support in week 1. NQRs were asked how long they
had been qualified and thus employed for, and also how long they had been
on their preceptorship programme. Figure 2 demonstrates that NQRs don’t
always embark on their preceptorship period at the commencement of
employment. This is of concern because the first few months of employment
can be very stressful for an NQR (Hickie et al, 2007). This is when
preceptorship is most important and maximum support should be available.
Even more concerning is the number of participants who claim not be on a
preceptorship programme at all. Some NQRs commented that although they
had not been assigned a specific preceptor, they were aided informally by all
of the staff on the ward. There was however some who stated they had no
preceptor at all, even though they felt they should. Unfamiliarity of the term
preceptorship may have affected the way participants answered this question,
as some NQRs may have been assigned someone referred to as a Mentor or
Tutor rather than preceptor. Lack of awareness of this term and its process
may be associated with not receiving an induction and guide to preceptorship
in the first week of employment. Whether it is due to a lack of awareness on
the NQRs’ behalf, or whether it is down to staff shortages, the fact that some

19
NQRs perceive that they are working without support does need to be
explored further.
The majority of NQRs are receiving the appropriate intensive support in the
first week of employment. 9% did not, and analysis of written comments
suggest that this may be due to the fact that they trained at the Acute Trust,
thus were familiar with the Trust standards, policies and procedures. The
minimum corporate standards state that each NQR is to receive intensive
support in week 1 (linked to induction period, including a guide to
preceptorship). All NQRs should receive intensive training in their first week
regardless of their training background.
NQRs are entitled to 1.5 days per month of teaching/study time, which can be
either formally taught/directed study or 1:1 supervision in practice. Figure 4
shows that the majority of NQRs did not receive their 1.5 days per month.
These findings may not be a true reflection of current practice as it is evident
from the additional comments that many NQRs were receiving at least one
study day. Allocated meetings with their preceptor were recognised as study
time by the preceptor, but NQRs were unaware of this. In conclusion, many
NQRs may in fact be receiving their study entitlement, as the minimum
corporate standards state, as teaching can take a number of forms. This
needs to be reinforced to NQRs.
The majority of NQRs were aware that they had competencies to complete,
and this did not appear to be an area of concern for anyone. Competencies
and progress reviews are linked with the appraisal cycle. Very few NQRs
were due for their appraisal, so are unable to comment on whether this was
being done in a timely manner.
More than half of NQRs do not have regular meetings with their preceptors to
review progress. This is despite the fact that the vast majority of NQRs rated
their preceptor as satisfactory or above (See figure 10), which would indicate
that they have a good working relationship. With some NQRs commenting
20
that they found it difficult to express their feelings to their preceptor, it would
seem that encouraging more regular, structured contact may improve
communication and a feeling of support. Some NQRs lost their preceptor
when they left the ward or Trust. In such a situation it is imperative that a new
preceptor is assigned so as to ensure the NQR receives their full 6 months of
preceptorship.
Of the very small sample size of participants on the Flying Start Scheme all
the feedback was positive and showed that it was a useful tool. This may not
be a valid representation however as there are 15 NQRs in total on the
scheme but due to annual leave they were difficult to audit.
4.2 Recommendations
The data collected indicates that NQRs who commence their employment
outside of the main recruitment period are less likely to receive an adequate
form of preceptorship. Adequate by our definition is a programme that
adheres to the minimum corporate standards. This issue needs to be
addressed immediately, and it is recommended that every NQR who begins
employment outside of the main recruitment period(s) is to have an
appointment with a member of their administrative team within two weeks of
the commencement of their employment. This aims to ensure that a) they
have been assigned a preceptor, and b) they have also actively started their
preceptorship programme. It is imperative that they are made aware of ALL of
the corporate standards. Ideally there should be a designated person within
each division who would monitor NQR enrolment and continued participation
on the preceptorship programme.
Misinterpretation by NQRs of what constitutes study days could account for a
portion of the sample not meeting this particular standard. Clearer assignment
of study days and emphasis that a NQR doesn’t have to leave a clinical
21
setting to be taking part in a study day may lead to different responses in a
future re-audit.
The audit captured a range of different professions, and the findings enabled
the analysis of how broadly the preceptorship programme was being utilised.
If a re-audit was to take place however, information on participant divisions
should be obtained to explore the benefit of additional funding. This could give
an indication of whether the reach of the preceptorship programme is related
to how much money each division allocates to it.
4.3 Action planning
Study Days
It is recommended that NQRs are allocated additional study time, and that a
new protocol is established to ensure study days are documented to meet the
monthly allocation. Ideally study time should be relevant to the NQR’s
respective field.
Assignment of Preceptors
The assignment of preceptors to NQRs should coincide with the
commencement of employment.
Duration of Preceptorship
The minimum 6 month period of preceptorship needs to fulfilled by every NQR.
If, for some reason, a preceptor is unable to perform their duty for reasons
such as annual leave, then an alternate preceptor must be assigned.
Designated Preceptorship Supervisor
Another recommendation is that within each division there is a designated
person to oversee the preceptorship programme. This person would be
22
responsible for ensuring that each NQR receives the adequate support and
encouragement they are entitled to.
Preceptor Meetings
It is recommended that meetings with preceptors should be more regular and
in a more informal manner to give NQRs an opportunity to express various
issues they may be experiencing during their preceptorship.
Network for NQRs
It is suggested a network is available for NQRs to contact each other and
share various problems, as well as solutions for their clinical experiences. An
online group or weekly meetings within the Acute Trust may be suitable.
Flying Start
It is recommended that in a future re-audit those on the Flying Start
programme should be compared with those who are not. This is in order to
verify the success of the scheme.
23
References
Ashurst,A .(2008) Career development: the preceptorship process. Nursing
and Residential Care 10:307-309
Clinical Audit Support Centre (2010) What is clinical audit?
http://www.clinicalauditsupport.com/what_is_clinical_audit.html (Accessed on:
5th March 2010)
Doh (2003)The NHS Confidentiality Code of Practice. London: Department of
Health.
DoH (2004) Agenda for change: final agreement. London, Department of
Health.
DoH (2008) High Quality Care For All. NHS Next Stage Review Final Report.
London, Department of Health.
DoH (2009) Preceptorship Framework for Nursing. London, Department of
Health.
East Kent Clinical Audit Service (2010) Clinical Audit Cycle.
http://www.ekclinicalauditservice.nhs.uk (Accessed on: 5th March 2010)
Hickie S, Lyttle CP and Harris LE (2007) Structured learning for newly
qualified nurses. Nursing Times 103: 28-29.
Irvine, S. and Irvine, D. (1997) Making sense of audit. Radcliffe Medical
Press, 2nd edn. Abingdon, UK.
NICE (2002) Principles for Best Practice in Clinical Audit. Radcliffe Medical
Press. Abingdon, UK
24
Appendices
Appendix 1
Minimum corporate standards: Preceptorship
• Each newly qualified assigned a preceptor.
• Preceptorship period to be a minimum of 6 months.
• Each newly qualifier to receive intensive support in week 1 (linked to
induction period to include guide to preceptorship)
• Each newly qualifier to be supported for one and a half days per month
in either formal taught/directed study or 1:1 supervision in practice.
• “Flying start” programme to be piloted in line with the national
programme on a separate cohort of New Qualifiers in Unscheduled
Care Division.
• Competency programmes to reflect the `Practioner, Partner, Leader`
model.
• Competency programmes must meet the minimum required KSF.
• Preceptorship competencies and progress reviews to be linked into
existing appraisal/review cycle.
• Assigned preceptors to meet the skills defined in the SCSHA
Preceptorship Framework (preferably existing mentors)

25
Appendix 2
Questionnaire for NQRs
We are a group of students investigating the efficacy of the preceptorship
programme for NQRs in health care. Throughout our data collection and
storage confidentiality will be maintained. Questionnaires will be destroyed
at the end of the project and staff have the right to refuse to participate.
Please circle appropriate answers where applicable.
1) What is you professional group?
……………………………………………………...
2) How long have you been qualified?
……………………………………………………...
3) Have your been assigned a preceptor?
………………………………………………………
4) How long have you been on your preceptorship programme?
………………………………………………………..
5) Did you receive intensive support in week one of employment?
Yes / No
6) Are you getting 1 ½ study days per month?
Yes / No
7) How are your study days constructed?
0) formal teaching
1) directed study
2) one to one supervision in practice
3) other please specify

26
…………………………………………………………………………
8)
a) Do you have competencies to complete?
b) Do you or your preceptor have regular meeting to review progress?
c) Have you had your 6 month appraisal or is it booked?
9) How you rate your preceptor?
1) Poor
2) Less than satisfactory
3) Satisfactory
4) Better than satisfactory
5) Excellent
10) Are you a participant of the flying start programme?
If yes please specify the benefits
……………………………………………………………….……………………
…………………………………………………………………………………….
11) Would you make any future recommendations to improve the
preceptorship programme?
………………………………………………………………………………………
………………………………………………………………………………………





























