Embed Size (px)
Citation preview

Author's Accepted Manuscript
Interpretation of Visceral Duplex ScanningPrior to and Following Intervention forChronic Mesenteric Ischemia
Kelley Hodgkiss-Harlow M.D.
PII: S0895-7967(13)00027-6DOI: http://dx.doi.org/10.1053/j.semvascsurg.2013.11.005Reference: YSVAS50419
To appear in: ĆSemin Vasc Surg
Cite this article as: Kelley Hodgkiss-Harlow M.D., Interpretation ofVisceral Duplex Scanning Prior to and Following Intervention forChronic Mesenteric Ischemia, ĆSemin Vasc Surg , http://dx.doi.org/10.1053/j.semvascsurg.2013.11.005
This is a PDF file of an unedited manuscript that has been accepted forpublication. As a service to our customers we are providing this earlyversion of the manuscript. The manuscript will undergo copyediting,typesetting, and review of the resulting galley proof before it is published inits final citable form. Please note that during the production process errorsmay be discovered which could affect the content, and all legal disclaimersthat apply to the journal pertain.
www.elsevier.com/locate/engana-
bound

1
Seminars in Vascular Surgery
Interpretation of Vascular Laboratory Testing
Interpretation of Visceral Duplex Scanning Prior to and Following Intervention for
Chronic Mesenteric Ischemia
Kelley Hodgkiss-Harlow M.D.
From the Division of Vascular Surgery, Kaiser Permanente, San Diego, CA
Keywords: visceral duplex, chronic mesenteric ischemia, ultrasound; surveillance, endovascular
therapy, stent-angioplasty
Address correspondence to: Kelley Hodgkiss-Harlow MD [email protected] AND Dennis Bandyk MD [email protected]
ABSTRACT
Duplex ultrasound testing has evolved to be a clinically useful modality for the evaluation of chronic
mesenteric ischemia (CMI) due to visceral artery origin atherosclerosis. Patients with known or
suspected CMI can be scanned to identify stenosis or occlusion of the celiac, superior mesenteric, and
inferior mesenteric arteries. Testing requires expertise in abdominal ultrasound imaging and arterial
duplex scan interpretation, as well as a fundamental understanding of visceral artery hemodynamics and
collateral pathways created as a result of occlusive lesions. Duplex testing can also be utilized to evaluate
functional patency following visceral artery bypass grafting procedures or endovascular stent angioplasty,
Repair site stenosis can be reliably identified which assists in decision-making regarding the need for re-

2
intervention to treat or prevent recurrent gut ischemia. Visceral duplex testing of a bypass graft or stent
angioplasty site that shows peak systolic velocity (PSV) >300 cm/s with end-diastolic velocities >50 to 70
cm/s, or a damped velocity spectra within a bypass graft and low (<40 cm/s) PSV should be considered
for interrogation by visceral angiography to confirm or exclude severe (>70%) stenosis. Visceral duplex
testing should be considered a screening diagnostic modality that compliments clinical assessment of
CMI both prior to and following open surgical or endovascular visceral artery interventions.
In the mid-80s, Dr. Eugene Strandness and colleagues at the University of Washington initiated
clinical investigations with color duplex ultrasound to characterize the hemodynamics of the splanchnic
(celiac artery, superior mesenteric artery [SMA], inferior mesenteric artery [IMA]) circulation. Testing in
patients with normal and abnormal visceral arteries confirmed the value of duplex scanning as a screening
study for the evaluation of chronic mesenteric ischemia (CMI).1-2 Duplex interpretation criteria were
further refined by Moneta et al from Oregon Health Science University and Zwolak et al from Dartmouth
and correlated with angiography to verify a diagnostic accuracy of 85-90% for the detection of >70%
visceral artery stenosis and the diagnosis of CMI.3-5 Threshold velocity criteria (peak systolic velocity
[PSV]; end-diastolic velocity, EDV) can be used to predict < or >50% and >70% diameter- reducing (DR)
stenosis of the celiac and the SMA. Duplex spectral waveform changes produced by atherosclerotic
disease in fasting and postprandial conditions were also characterized from testing of both healthy
subjects and symptomatic patients with confirmed CMI. Prospective studies were also conducted to
confirm duplex diagnostic accuracy by angiographic verification of disease severity.3-6 The addition of an
EDV threshold in conjunction with elevated PSV was found to improve the sensitivity, the specificity,
and the accuracy rates of visceral duplex testing in the detection of >50% DR stenosis.,7
The presence of multiple visceral artery involvement, i.e. concomitant celiac and SMA occlusive
disease and/or anatomic anomalies (right hepatic artery origin from SMA) influences diagnostic accuracy.
Overestimation of stenosis severity due to compensatory collateral flow conditions is an important test
limitation artifact which has led some vascular groups to not rely on or trust duplex findings. In a patient
presenting with sitophobia (fear of eating) and weight loss caused by CMI, the SMA is always diseased,

3
either occluded or severely stenotic (>70% DR). Duplex testing can aid in the evaluation of these patients
by providing objective hemodynamic evidence of abnormal SMA and celiac artery branch vessel blood
flow. Visceral artery duplex interrogation should be viewed as screening diagnostic test that compliments
clinical evaluation and computed tomography (CT) or digitial subtraction angiography (DSA) imaging
studies. In this review, the application of duplex ultrasound in diagnosis of CMI and surveillance of
arterial interventions for patency and restenosis is detailed with attention to test interpretation criteria.2-12
Visceral Duplex Testing and Interpretation Criteria
Atherosclerotic lesions of visceral arteries typically develop at or near the origin. Duplex imaging of the
pararenal aorta is best performed in the morning after an overnight fast which minimizes presence of
bowel gas to optimize conditions for the vascular technologist to identify and interrogate the visceral
arteries. A slight reversed Trendelenburg or head elevated position can be helpful for para-aorta segment
imaging. Identification of renal arteries and the left renal vein anterior to the aorta are reliable landmarks
to then image cephaled to the origins of the SMA and celiac artery. Both transverse and sagittal scan
planes should be used to image the celiac trunk and SMA origins and acquire Doppler-angle corrected
velocity spectra. Velocity spectra should be recorded from the origin and mid-SMA, celiac artery trunk,
hepatic artery, and if possible splenic artery. Often a Doppler angle of 0 to 30 degrees is required to
acquire velocity spectra from the celiac artery origin. Disease classification is based on measurements of
PSV, end-diastolic velocity (EDV), and changes in the SMA velocity spectral waveform from a fasting to
post-prandial state (Table 1). Significant (≥70% DR) stenosis, i.e. pressure-, flow-reducing lesion, is
associated with color power Doppler lumen reduction and imaging with elevated blood flow velocity;
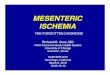
PSV > 275-300 cm/s, and EDV >45-55 cm/s (Figure 1). The spectral waveform at and immediately
distal to the stenosis should demonstrates turbulence which abates further downstream when damping of
the velocity waveform occurs (Figure 2). Use of mesenteric-aortic PSV ratio >3 is also predictive of
>50% DR stenosis. AbuRhama et al6 reported PSV threshold of 400 cm/s for >70% SMA stenosis
(overall accuracy of 85%) ; and 320 cm/s for >70% stenosis of the celiac artery origin (overall accuracy

4
of 85%). Receiver operator curve analysis indicated PSV was better than end-diastolic velocity in
predicting >70% stenosis. An interpretable study is possible in >80% of individuals with excessive bowel
gas being the primary reason for a sub-optimal study.
To induce a post-prandial state, the patient is asked to drink 8 oz. a protein calorie supplement as a test
meal with duplex testing repeated within 30 minutes to identify changes in the SMA velocity spectra, i.e.
PSV and EDV increase. If an SMA stenosis is present further damping of the mid- downstream SMA
spectral waveform will occur; and indicates an increase in the systolic pressure gradient across the
stenosis has developed. A test meal produces no change in IMA flow and minimal elevation in celiac
PSV; unless that artery is providing compensatory collateral flow. Using this protocol, visceral duplex
testing has the ability to verify hemodynamic changes associated with eating, and provide justification for
additional visceral artery imaging, including angiography with pressure gradient measurement across
imaged stenosis. While post-prandial testing with administration of a test meal is not routinely
performed, but we have found this maneuver to be helpful in study interpretation. This is particularly
relevant following endovascular intervention when elevated PSV (>200 cm/s) is recorded from the stent-
angioplasty site. The presence of in-stent stenosis based on duplex PSV threshold criteria is common (20-
50% incidence) due to incomplete stent expansion, myointimal thickening, or compensatory collateral
flow if the celiac artery occlusive disease is present. The higher rate of SMA stent stenosis compared to
other (celiac, renal) artery stents makes duplex scanning is an ideal, noninvasive monitoring technique
following endovascular therapy.8-11
Visceral duplex testing is also useful for intraoperative assessment of artery repair by endarterectomy or
bypass grafting, and in diagnosis of median arcuate compression syndrome. For intraoperative testing, a
10-15 MHz linear array transducer should be used to image the repair and record velocity spectra.
Transducer placement directly over the arterial repair with multiplane B-mode, color and power Doppler
imaging is necessary identifying lumen abnormality and confirm a widely patent repair. Velocity spectra
are recorded at corrected Doppler angle of 60 degrees or less using a small (1-2 mm) pulsed Doppler
sample volume positioned in the centerstream flow. Visceral artery repairs can be tortuous requiring

5
imaging in both sagittal and transverse planes using B-mode, color and power Doppler to identify lumen
reduction and sites of flow turbulence. Common technical abnormalities detected include stenosis,
residual plaque, and platelet thrombus. The detection of lumen defect and PSV >200 cm/s are criteria for
a technical problems and should prompt revision of the artery repair. The Mayo Clinic vascular group
reported an 8% incidence of duplex-detected technical errors with routine intraoperative assessment.
Normal duplex testing, including after repair of an identified abnormality was associated with decreased
graft related complications, including thrombosis (1-4% incidence) and death.
The diagnosis of median arcuate ligament syndrome is based primarily on duplex imaging of the celiac
axis although cases of concomitant involvement of the SMA have been reported. The finding of a focal
elevation of PSV, i.e. stenosis, at the celiac artery origin that increases further with deep exhalation is
diagnostic for median arcuate syndrome. Damping of the velocity spectral waveform in the hepatic and
splenic artery indicates a hemodynamically significant stenosis is present. Individuals with median
arcuate syndrome have transient compression of the celiac artery origin by the diaphragmatic ligaments
during exhalation that is relieved by descent of the diaphragm with inhalation. The hemodynamics of
celiac, hepatic and splenic artery blood flow is one of low-resistance with antegrade flow throughout
systole and diastole; blood flow characteristic of the liver and spleen. Blood flow hemodynamics will be
altered by celiac axis occlusion or high-grade stenosis. Compensatory collateral flow from SMA
branches, primarily the gastroduodenal and pancreaticoduodenal arteries, may results in flow reversal in
the common hepatic artery with damping of the velocity spectra, i.e. pulsus tardus waveform. Flow in the
hepatic and splenic arteries will remain antegrade.
Duplex imaging of the SMA should be performed from its origin to as far distal as possible to accurately
lesion extent and assess distal velocity spectra. The normal fasting SMA velocity spectra is triphasic, i.e.
high-resistance flow pattern with antegrade flow in systole. Flow resistance decreases with eating
producing monophasic velocity spectra with antegrade flow throughout the pulse cycle but minimal
elevation in PSV. If the right hepatic artery originates from the SMA (an anatomic variant in 5-10% of
individuals), the “normal” fasting SMA flow is low resistance. The presence of celiac artery occlusive

6
disease (atherosclerosis or median arcuate ligament compression) can alter SMA flow hemodynamics due
to compensatory collateral flow; a condition which can lead to overestimation of stenosis severity. The
most accurate indicator of severe SMA stenosis is the presence of damping of the distal SMA waveform
in a fasting state which becomes less pulsatile after a test meal.
Duplex scanning of bypass grafts to the SMS is facilitated by knowing the origin of the conduit from the
supraceliac aorta (antegrade bypass) or iliac artery (retrograde bypass). Once identified, the bypass graft
is imaged along its length for lumen or color Doppler flow abnormality with particular attention to
proximal and distal anastomotic sites. Recording of a midgraft spectral waveform and volume flow
measurement can facilitate the diagnosis of graft stenosis and disease progression as often complete graft
imaging is difficult. The blood flow characteristics in retrograde and antegrade visceral bypass grafts are
similar; PSV in the graft in the range of 150-200 cm/s for a 6 mm dia. PTFE conduit. The volume flow is
in the range of 1-1.5 L/min for retrograde iliac-SMA bypasses.
Duplex testing after endovascular therapy
Duplex testing after endovascular intervention is possible in the majority of patients in part
because of the weight loss associated with CMI and the relative ease of SMA imaging. If an interpretable
study was obtained prior to endovascular intervention, the patency and hemodynamics of the angioplasty
site(s) can be assessed and compared. Stent deployment and balloon dilation across a visceral artery
stenosis delivers radial forces to expand the lumen and maintain a larger diameter. After angioplasty,
both positive (stent expansion) and negative (wall recoil, myointimal hyperplasia, arcuate ligament
compression) remodeling occurs with the potential for lumen caliber changes. The in-stent stenosis
which develops in 20-40% of patients after SMA or celiac angioplasty is caused by myointimal
hyperplasia and can be detected and stenosis graded using duplex ultrasound. Use of power Doppler
imaging in conjunction with pulsed Doppler flow analysis can identify stent lumen reduction and its
associated increase in PSV, but notably cannot identify stent fracture. A “normal” stent angioplasty site is
associated with widely patent color flow lumen, non-disturbed velocity spectra, PSV<250 cm/s and a
PSV ratio of < 2 along the stent length and relative to the distal artery. Elevation of PSV >300 cm/s with

7
EDV>100 cm/s has correlated with a >70% DR stenosis. The stented arterial segment is associated with
a decrease in wall compliance producing a compliance mismatch with the native artery and may account
for the elevated velocities seen at an angioplasty site compared with a surgical bypass anastomosis.11
AbuRhama et al reported PSV criteria of 400 cm/s for >70% in stent stenosis with a sensitivity of 100%
and overall accuracy of 97%. When borderline velocity criteria for stenosis are recorded, testing after a
meal should be performed. Duplex testing after visceral interventions is a screening study and should be
used as an adjunct to clinical assessment; when abnormal, angiographic assessment with measurement of
pressure gradient across a duplex-detected stenosis is recommended.
If the SMA provides collateral flow to an occluded celiac artery origin, the stent PSV may be more
elevated than if the celiac artery is patent and nonstenotic. Duplex testing after a test meal is useful in
determining the significance of an elevated stent PSV—if damping of the arterial spectral waveform
develops after eating, a clinical significant stenosis is likely to be confirmed by angiography and pressure
gradient measurement. Several anatomic conditions negatively affect the clinical application and the
diagnostic accuracy of visceral duplex testing, such as obesity; fortunately, obesity is not commonly
associated with CMI. Normal anatomic variants, such as a right hepatic origin from the SMA, will alter
normal arterial patterns in the fasting state. Collateral flow due to multivessel involvement can lead to
overestimation of stenosis severity if disease classification is based on PSV alone. Inaccuracies in
velocity measurement may also occur when vessel tortuosity is present since may be difficult to
impossible to achieve a Doppler angle of insonation <60°.
Surveillance After Visceral Artery Intervention
After visceral artery intervention, patients should be enrolled in a surveillance program that includes color
duplex scanning of the mesenteric arteries and the arterial repair or bypass. Duplex scan criteria for >70%
recurrent stenosis involving the celiac, superior or inferior mesenteric arteries, angioplasty site, or a
bypass graft was a PSV more than 300 cm/s, EDV more than 50 cm/s, and post-stenotic turbulence. A
clearly visualized vessel with no color Doppler flow or velocity spectra signal characterizes an occluded
vessel, angioplasty site, or bypass graft. Velocity spectra of the mid-SMA and distal SMA are evaluated

8
for flow velocity waveform damping due to proximal occlusive disease and inadequate collateral arterial
flow. If duplex testing is equivocal because of poor visualization of the intervention site, angiographic
imaging of the visceral PTA site or surgical repair should be considered. Angiographic criteria for a
significant visceral artery stenosis is >50% DR and a systolic pressure gradient >10 mm Hg at baseline
flow or after flow augmentation with intra-arterial papaverine (30 mg).
Currently, there is no consensus on which velocity criteria should be used to define high-grade recurrent
disease. Most large vascular series propose periodic clinical reassessment of the patient with a focus to
uncover recurrent symptoms of intestinal angina, such as meal intolerance, pain, diarrhea, dyspepsia, and
weight loss before considering a need for reintervention. While intuitively this seems like a rational
course of action, caution against complacency must be considered as most investigators have reported
high-mortality rates in individuals who develop acute mesenteric ischemia after revascularization. Among
reported series of mesenteric revascularizations, clinical follow-up alone inaccurately predicted graft
occlusion and was associated with a sensitivity as low as 33%.8
The management of asymptomatic high-grade stenosis after both open and endovascular repair remains
undefined. Fortunately, the embolic potential of myointimal hyperplasia associated with surgical or
endovascular intervention is uncommon. Progressive stenosis of the original atherosclerotic lesion or
restenosis/occlusion of the splanchnic repair remains the most common cause of recurrent symptoms
among treated patients. Since recurrent symptoms are associated with intervention failure and increase the
risk for gut necrosis, a more aggressive approach toward treating endovascular stent stenosis is
appropriate in these patients. In asymptomatic patients, we have reserved intervention to vessels showing
progressive repair site stenosis >70% DR as shown by duplex ultrasound, followed by confirmatory
angiographic imaging with pressure gradient measurement. Re-intervention using endovascular therapy is
usually successful, reduces PSV at the stenosis site, and is associated with continued relief of gut
ischemia.
Testing at 6-month intervals has been sufficiently frequent to detect developing stenosis after
intervention. An audit of 69 procedures (31 surgical and 38 endovascular) which treated 84 visceral

9
arteries at the University of South Florida over a 12-year period confirmed no asymptomatic SMA
occlusion developed using biannual surveillance. Asymptomatic celiac artery repair occlusion developed
in 4 patients after open (n = 2) or endovascular (n = 2) intervention, therefore duplex ultrasound
surveillance is used primarily as a screening study in asymptomatic patients. Any recurrence of symptoms
suggestive of CMI with elevated in-stent or mesenteric bypass velocities (SMA: PSV > 300 cm/s, EDV >
50 cm/s; celiac artery PSV > 250 cm/s, EDV > 45 cm/s) should prompt angiographic confirmation of
restenosis. For patients with asymptomatic CMI with elevated in-stent or graft anastomotic velocities,
serial studies are compared with attention to changes of stent structure, development of intimal
hyperplasia, and changes in collateral or downstream mesenteric velocities. In the asymptomatic patient,
the finding of a lesion with poststenotic turbulence, a PSV >300 cm/s, and EDV >50 cm/s in the SMA is
an indication to consider angiographic evaluation. Angiography is also recommended when stent
migration or changes in mesenteric bypass volume flow or graft PSV are identified. A PSV increase
>150 cm/s on serial testing was associated with the development of either clinical symptoms or an
angiographic stenosis with a resting systolic pressure-gradient >15 mm Hg. Stenosis in a celiac or IMA
repair may also be clinically important especially in patients with SMA occlusion or stenosis.
Duplex surveillance after mesenteric revascularization resulted in 3-year primary patency rates of 62%
after endovascular therapy and 82% after surgical bypass, P < .01. Secondary interventions for duplex-
detected stenosis produced similar primary-assisted patency rates (95% and 92%) in surviving patients.
The benefit of duplex surveillance was most evident after endovascular therapy, with 25% of stent-
angioplasty sites developing progressive in-stent stenosis necessitating a secondary endovascular
reparative procedure. In 15 patients who underwent 21 secondary interventions, the preprocedural duplex
study identified a stenosis with a mean PSV of 530 ± 89 and EDV of 168 ± 67 cm/s.
The finding of a PSV in the range of 300 cm/s or higher has been observed after angiographically
successful SMA stent-angioplasty. Duplex testing is a screening study and when there is progressive
increase in PSV and EDV suggesting in-stent stenosis, it is a clinical decision to proceed with
confirmatory angiography and possible intervention. In some patients with stent stenosis, treatment

10
options are limited because of medical comorbidities, disease location, and patient preferences. Currently,
30 patients are enrolled in our surveillance program, and in one-half, a SMA angioplasty site with a PSV
>300 cm/s has been recorded. The mean PSV of 23 SMA stent-angioplasty sites with no secondary
intervention was 368 ± 78 cm/s. If a stenotic lesion is progressive on serial testing or the patient develops
any intestinal angina, we proceed to visceral angiography.
Summary
The clinical application of visceral duplex ultrasound has been established for both the diagnosis of CMI
and the evaluation of open and endovascular repairs for visceral artery occlusive disease. Surveillance
guidelines are similar to testing after carotid intervention and lower limb bypass grafting; including an
initial study to exclude residual stenosis followed by interval testing at 6 mo. intervals for repair site
failure. The velocity criteria that accurately predicts stenosis of a mesenteric revascularization continues
to evolve but PSV >300 cm/s with distal damping is abnormal. Since clinical follow-up of patients with
CMI may be insensitive to the development of repair site stenosis, it is reasonable to apply duplex testing
to improve the vascular diagnostic in patients with vague abdominal symptoms and to improve procedure
outcomes after intervention.

11
References
1. Nicholls SC, Kohler TR, Martin RL, Strandness DE Jr. Use of hemodynamic parameters in the
diagnosis of mesenteric insufficiency. J Vasc Surg. 1986;3:507-510.
2. Jagar KA, Fortner GS, Thiele BI, Strandness DE Jr. Noninvasive diagnosis of intestinal angina. J Clin
Ultrasound. 1984;12:588-591.
3. Moneta GI, Taylor DC, Helton WS, Mulholland MW, Strandness DE Jr. Duplex ultrasound
measurement of postprandial intestinal blood flow: effect of meal com- position. Gastroenterology.
1988;95:1294-1301.
4. Moneta GL, Lee RW, Yeager RA, Taylor LM, Porter JM. Mesenteric duplex scanning: a blinded
prospective study. J Vasc Surg. 1993;17:79-86.
5. Zwolak R, Fillinger M, Walsh D, et al. Mesenteric and celiac duplex scanning: a validation study. J
Vasc Surg. 1998;27:1078-1088.
6. AbuRhama AF, Stone PA, Srivastava M, et al. Mesenteric/celic duplex interpretation criteria revisited.
J Vasc Surg 2012;55:428-436.
7. Perko MJ, Just S, Schroeder TV. Importance of diastolic velocities in the detection of celiac and
mesenteric artery dis- ease by duplex ultrasound. J Vasc Surg. 1997;26: 288-293.
8. Liem TK, Segall JA, Wei W, Landry GJ, Taylor LM, Moneta GL. Duplex scan characteristics of
bypass grafts to mesenteric arteries. J Vasc Surg. 2007;45:922-928.
9. Landis MS, Rajan DK, Simons ME, Hayeems EB, Kachura JR, Sniderman KW. Percutaneous
management of chronic mesenteric ischemia: outcomes after intervention. J Vasc Interv Radiol.
2005;16:1319-1325.
10. Mitchell EL., et al. Duplex criteria for native superior mesenteric artery stenosis overestimate
stenosis in stented superior mesenteric arteries. J Vasc Surg 2009;50:335-340.
11. AbuRhama AF, Mousa AY, Stone PA, et al. Duplex velocity criteria for native celiac/superior
mesenteric artery stenosis vs in-stent stenosis. J Vasc Surg 2012;55:730-738..

12
Table 1. Visceral duplex ultrasound criteria for normal and stenotic celiac, SMA, and IMA flow.
Normal:
Celiac: PSV - (90-110 cm/s); low resistance flow pattern
SMA: PSV – (95-150 cm/s); high resistance flow pattern in fasting state with EDV>0
after meal
IMA: PSV – (90-180) cm/s; high resistance flow pattern
Diagnostic testing (Fasting)
<70% Stenosis:
Celiac: PSV<200 cm/s, EDV<55 cm/s; resistive index <0.75
SMA: PSV<300 cm/s, EDV<45 cm/s with diastolic flow reversal in distal SMA
IMA: PSV<200 cm/s, antegrade resistive flow (like SFA)
>70% Stenosis:
Celiac: PSV>200 cm/s, EDV>55 cm/s with retrograde common hepatic artery flow with
severe stenosis or celiac artery occlusion
SMA: PSV>300 cm/s, EDV>45 cm/s with loss of diastolic flow reversal
IMA: PSV>200 cm/s, antegrade flow with loss of diastolic flow reversal
Mesenteric-aorta ratio >3
Velocity Spectra Changes with Test Meal
Increase in PSV at sites of stenosis with damping of distal waveform – used most
frequently to assess the significance of SMA occlusive disease.

13
Figure 1. Duplex image and velocity spectra recorded from the origin of the superior mesenteric artery
with a >70% diameter reducing stenosis based on a eak systolic velocity of 388 cm/s and end-diastolic
velocity of 77 cm/s.

14
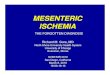
Figure 2. Duplex image and velocity spectra recorded from the distal superior mesenteric artery (SMA)
with an origin >70% diameter reducing stenosis. Note damped waveform configuration with slow
acceleration time and flow thru-out pulse cycle in a fasting state.

15
Review questions.
1. Ingestion of a test (fat/carbohydrate) meal during a visceral duplex scan produces:
A. An increase in SMA end-diastolic velocity (EDV)
B. A high resistance waveform in the celiac axis
C. An increased in SMA resistive index (RI)
D. No change in SMA peak systolic velocity
Answer:

16
2. Visceral duplex testing of the celiac artery after median arcuate ligament division and balloon
angioplasty demonstrates a peak systolic velocity of 168 cm/s; end-diastolic velocity of 46 cm/s.
The severity or residual stenosis in celiac artery is
A. 0% stenosis
B. <70% stenosis
C. >70% stenosis
D. >90% stenosis
Answer:

17
3. The duplex scan images of the superior mesenteric artery (SMA) after stent angioplasty
indicates
A. Stent compression
B. Stent migration
C. Stent thrombus
D. >70% in stent stenosis
Answer:

18
Answers to Questions:
1. A
2. B
3. D








![Challenges Encountered during the Treatment of Acute ...acute mesenteric ischemia is a great clinical challenge [1–6]. ... of acute mesenteric ischemia, occurring in 38 (92.68%)](https://img.pdfslide.us/doc/110x75/60f89ecd2be9754e8c1fff31/challenges-encountered-during-the-treatment-of-acute-acute-mesenteric-ischemia.jpg)

















