-
7/26/2019 interpretasi x ray
1/4
INTENSIVE CARE SERVICE
NURSING POLICY & PROCEDURES
NAME OF POLICY: CHEST XRAY INTERPRETATION
GOAL: TO SAFELY AND EFFECTIVELY ACCESS AND INTERPRET
CHEST FILMS.
Introduction: Chest x-rays are a commonly used tool in the ICU.
They can provide
confirmation of clinical observations, show anatomical
landmarks, confirm placement of lines,
tubes, catheters and leads. They are also used to monitor
changes in the lung pathology.
Procedure:
Using the PACs x-ray viewer correctly identify the patient, date
and time that you wish
to access
Note the view of the film, either AP or PA. In ICU the x-ray is
taken using a mobile x-ray
machine at the bedside. The view that is taken is known as an AP
(Anterior Posture) view.
An x-ray taken in the radiology department with the patient
standing independently is a
PA (Posterior Anterior) view. The main difference between the
two views is the AP (taken
in the unit with mobile x-ray machine) is not as sharp, and the
anatomical landmarks are
magnified. I.e. the heart appears larger and the mediastinum
appears widened. This is due
to the change in distance from the x-ray plate to the machine.
In ICU the distance is
approximately 90cm as apposed to 180 cm when taken in
radiology.
Patient position.Chest X-rays are usually taken with the patient
in the erect position.
Supine films alter the position and shape of the mediastinal
structures and may make
pleural effusions and a pneumothorax more difficult to
identify.
Check to see how the x-ray has been exposedas this may alert you
to problems. If the x-
ray has been under or over exposed lung pathology may not be as
easily identified. To
determine if the x-ray is correctly exposed you should be able
to identify the tear drop
appearance of the spinal process, and the outline of the
vertebral column through the heart
shadow but not the intervertebral spaces.
Inspiratory or Expiratorychest x-ray. When a person inspires the
diaphragm drops andthe lungs expand. It is therefore important to
take the x-ray when the maximum amount of
lung is visible i.e. on inspiration. By counting the visible
ribs you can determine when the
film was taken. In the normal lung you should be able to count
10 Posterior and 6 Anterior
ribs if the x-ray was taken on inspiration. Occasionally an
erect x-ray is taken in expiration
specifically to help identify a pneumothorax (which looks larger
on an inspiratory film).
Orientation.How to get your bearings. You need to identify that
the clavicles are
symmetrical (the spinous processes should be mid-way between the
two clavicular heads),
the trachea is midline and all of the structures in the thoracic
cage are visible. If these
structures can not be seen it may mean that the patient was
positioned poorly for x-ray. As
a rule the trachea should be midline if not there may be areas
of collapse, mass or
pneumothorax. Identify the normal structures on the x-ray, eg
the heart, clavicles, ribs and spinal
processes. By doing this you are identifying the four densities
bone or metal, fat, water
ROYAL PRINCE ALFRED HOSPITAL INTESNIVE CARE SERVICE
-
7/26/2019 interpretasi x ray
2/4
and air. Bone or metal are the most dense, they absorb the
largest amount of x-ray and so
appear white on the film. Fat is less dense and appears off
white, eg breast tissue. Water is
also less dense than bone, it appears as off white/grey. Eg
Blood in the heart and vessels.
Air is the least dense, appearing almost black on x-ray, eg.
lung tissue.
While identifying the different structuresand different
densities observe the following:-
The heart should be visible in the left anterior mediastinal
cavity. It should be less than
half the width of the chest wall on a PA film and slightly
larger on an AP film. Anincrease in the cardiac shadow may mean
congestive heart failure, pericardial effusion or
pulmonary oedema. The lung fields and bronchi are not usually
visible except for the
lung markings in the periphery. Abnormal findings in the lung
fields can include air
bronchograms the difference in density between air filled
bronchi and adjacent areas of
consolidation. Patchy infiltrates or streaky densities could
mean pneumonia or atelectasis
while fluffy infiltrates or Kerley B lines show pulmonary
oedema. Look also for
collapse, consolidation and air or fluid in the pleural space.
The diaphragmshould appear
rounded at the bottom of the lung fields with right side being 1
2cm higher than the left
due to the liver under the right hemidiaphragm. The heart lies
on the left hemidiaphragm.
Costaphrenic anglesshould appear clear and sharp, the presence
of a pleural effusion,
collapse and/or consolidation could be the reason for
obliteration of the angles. Observethe ribs for fractures,
osteoporosis, malignancy or other bony changes.
Note the placement of lines, tubes, catheters and leads.
Endotracheal tube 2 - 3cm above the carina
Nasogastric/ Orogastric tube tip and side holes must in the
stomach
Central Venous Catheter tip sits in the Superior vena cava
outside the right atrium
Tracheostomy tip should be half to two thirds from the stoma to
the carina
Intra Aortic Balloon Pump the distal tip should be visible in
the proximal descending
thoracic aorta, distal to the aortic notch and above the level
of the left main bronchus
Pacing leads usually sit at the apex of the right ventricle.
Pulmonary Artery Catheters pass through the right side of the
heart, main pulmonary
artery and a short way into the lung.
Lastly comparethe x-ray to previous films taken.
Bear in mind the following sites of commonly missed
pathology:
Lung apex
Lung periphery/pleura
Behind the heart
Costophrenic areas
Quick Steps
Correct patient, date and time PA or AP view
Erect or supine
ROYAL PRINCE ALFRED HOSPITAL INTESNIVE CARE SERVICE
-
7/26/2019 interpretasi x ray
3/4
Exposure
Inspiratory/Expiratory phase
Orientation get your bearings, identify densities, identify
structures
Identify lines and tubes
Look at mediastinum, lung, bones, soft tissues etc. in
systematic way
Compare
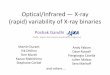
Posterior Anterior Chest View
REFERENCES:Bucher, L; Melander, S. 1999: Critical Care Nursing
1stEdition, 1999 pp 405 - 407Darovic, G. Shades of Grey:
Understanding chest X-rays, Nursing 98; 28 (7): 32cc1-32cc5Darovic,
G. Understanding chest X-rays, part II: How To Recognise Changes
Caused by Cardiac Disease, Nursing99; December: 32cc10
32cc11Darovic, G. Understanding chest X-rays, part III: How To
Recognise changes Caused by Pulmonary Problems,
Nursing 99; March: 32cc6 32cc7
Occupational Health and Safety: Universal precautions taken in
the preparation, administration of drug anddisposal of equipment
and sharps.
Cross Referenced: RPAH Occ. Health & Safety Manual and
Infection Control ManualNSW Infection Control Policy 98/99
Revised by: Vivienne East (CNS) July 2002Reviewed by: Chanelle
Innes (CNC)
Authorised by: Paul Phipps (Intensivist)
Revision July 2004
With the introduction of Powerchart online ordering, a clinical
agreement has been set up with the Director
of ICS and other Staff Specialists. Nursing Management, with the
agreement of the hospital executive, have
made arrangement that allows all permanently employed RPAH
Nursing Staff to place orders for a variety of
tests on their behalf. It is a Health Insurance Commission (HIC)
directive that all orders placed by nursing
staff are countersigned by the responsible MO within 14
days.
1. Trachea
2. Right Main Bronchus
3. Left Main Bronchus
4. Left Pulmonary Artery
5. Right Upper Lobe Pulmonary
Vein
6. Right Interlobar Artery
7. Right Lower and MiddleLobe Vein
8. Aortic Knob
9. Superior Vena Cava
10. Carina
ROYAL PRINCE ALFRED HOSPITAL INTESNIVE CARE SERVICE
-
7/26/2019 interpretasi x ray
4/4
ROYAL PRINCE ALFRED HOSPITAL INTESNIVE CARE SERVICE