Embed Size (px)
Citation preview

Potmftw
tedcrpfmplfiopdt
S
a
d
1
e
©
0
d
J Oral Maxillofac Surg67:31-39, 2009, Suppl 3
Interpositional Osteotomy for PosteriorMandible Ridge Augmentation
Michael S. Block, DMD,* Christopher J. Haggerty, DDS, MD†
This report reviewed the published data concerning different methods for vertical augmentation of theposterior mandible for implant placement. The main purpose was to compare and contrast the differenttreatment methods, with a more detailed review of the use of the interpositional osteotomy to verticallyaugment the posterior mandible. After the data review, we present a case illustrating this method. On thebasis of the data review, the use of the interpositional osteotomy might be the method of choice forselect patients.© 2009 American Association of Oral and Maxillofacial Surgeons
J Oral Maxillofac Surg 67:31-39, 2009, Suppl 3TPa
ncsbadc
uIdct
oprttdpmmdpbsc
atients often request fixed dental implant restorationf missing posterior teeth in the mandible, defined forhe present report as the region posterior to theental foramen. This region has obvious limitations
or implant placement, including bone deficiency andhe presence of the inferior alveolar nerve (IAN)ithin the body of the mandible.After the teeth are removed, a continuous resorp-
ive process of the alveolar ridge occurs that is accel-rated by denture wear1 and is the most pronounceduring the first 12 months after the extractions.2,3 Theontinuing resorption of alveolar bone will eventuallyesult in less than ideal bone superior to the IAN,reventing dental implant placement without per-
orming augmentation of alveolar bone height. Aug-entation of the bone superior to the IAN shouldrovide sufficient bone for implant placement and
ong-term successful restoration of missing teeth withxed implant borne prostheses. All suggested meth-ds should consider patient-related issues, includingain, swelling, sensory nerve disturbances, the inci-ence of graft failure and resorption, and the func-ional restoration long term.
*Private Practice, Metairie, LA.
†Private Practice, Kansas City, MO; Former Resident, Louisiana
tate University School of Dentistry, New Orleans, LA.
Drs Block and Haggerty state no financial arrangement or affili-
tion with a corporate organization or a manufacturer of a product
iscussed in this article.
Address correspondence and reprint requests to Dr Block:
10 Veterans Memorial Blvd, Suite 112, Metairie, LA 70005;
-mail: [email protected]
2009 American Association of Oral and Maxillofacial Surgeons
278-2391/09/6711-0305$36.00/0
loi:10.1016/j.joms.2009.07.008
31
echniques Available, Historicalerspective, Advantagesnd Limitations
NERVE REPOSITIONING
Repositioning of the IAN consists of exposing theerve from a lateral approach with its release from theanal, and moving it laterally from the cancellouspace, allowing implants to be placed to the inferiororder of the posterior mandible. Surgical exposurend moving the nerve laterally results in a high inci-ence of sensory nerve disturbance and an excessiverown-to-root ratio of the prosthesis.4-11
SHORT IMPLANTS
One question is whether short implants can besed when no more than 5 mm of bone is above theAN. Mechanical studies using cylindrical implants ofifferent width and lengths have indicated that me-hanical pull-out resistance is inversely proportionalo the length of an implant, but not its diameter.12,13
Previous reports have indicated that more failuresccurred in the posterior mandible with short im-lants.14 Short implants lead to a poor crown-to-rootatio and compromised the results of the final pros-hesis, depending on the type of prosthesis used andhe interarch distance.15,16 On the basis of the evi-ence available regarding the success with short im-lants, the shortest implant length for the posteriorandible was traditionally recommended to be 10m.16 However, recent improvements in implantesign, especially in thread specifications, and im-rovements in implant surface characteristics, haveeen shown to be effective for implants 8 mm orhorter in length for the posterior mandible, afterompletion of evidence-based clinical series with
ong-term follow-up.
ugcahcmamaaIpstubbtpm
tO4aucvd3lcd
ffsgmd
skpt
onghtt
wfpgtsi
PW
atpnpwptvmcatm
wsiihfmt
ttsaf13
famsraWptbp
32 INTERPOSITIONAL OSTEOTOMY
ONLAY GRAFT PROCEDURES
Grafting bone on the superior surface of the resid-al alveolar cortical bone is accomplished by firstaining access to the cortical bone, placing and se-uring a bone graft to the region to be augmented,nd closing the soft tissue. Various graft materialsave been used, including iliac crest cortical andancellous bone, calvarial bone, symphyseal and ra-us bone, and banked bone, including both allograft
nd xenograft. The grafts have included blocks ofaterial, particulate material with membrane cover-
ge, or combinations of both. The advantage of usingn onlay graft is avoidance of direct damage to theAN, ease of placement of the graft, and immediateostoperative vertical augmentation. However, inci-ion breakdown over the graft can result in a reduc-ion of the long-term augmentation, especially whensing grafts composed predominantly of corticalone.1,17-20 Grafts composed of corticocancellousone blocks from the iliac crest resorb rapidly duringhe remodeling process; hence, the implants must belaced in a timely manner, typically between 3 and 4onths after iliac crest block augmentation.Bone resorption resulting in loss of bone augmen-
ation height has been reported by Cordaro et al.18
nlay block grafts from either the ramus or chin lost1.5% of height during the first 6 months. Bell et al1
ccessed the severely atrophic edentulous mandiblesing an extraoral approach and placed corticocan-ellous block grafts from the posterior ileum. Theertical bone height increased in the posterior man-ible from 5 to 8 mm; however, after 4 to 6 months,mm of bone was lost in the posterior mandible (23%
oss). Because of vertical bone resorption in theseases, implants were placed only in the anterior man-ible.Proussaefs et al19 and Proussaefs and Lozada20 per-
ormed intraorally harvested autogenous block graftsor vertical alveolar ridge augmentation. Their resultshowed a vertical augmentation at 1 month after sur-ery of 5.75 mm and a vertical augmentation at 4 to 6onths after surgery of 4.75 mm. The total bone loss
uring the first 6 months was 17.4%.Pikos21 used block grafts harvested from intraoral
ites to augment the posterior mandible 6 mm. Pi-os21 allowed 5 months for graft healing before im-lant placement and reported 0% to 20% graft resorp-ion provided no flap dehiscence occurred.
Chiapasco et al15 reported using either distractionsteogenesis (DO) methods or rigidly fixated autoge-ous block onlay grafts from the ramus. The DOroup showed an average increase in the verticaleight of the mandible of 5.3 mm versus 4.6 mm forhe onlay group. The results of their study showed
hat DO had a clinically similar bone response to that lith traditional onlay grafting. No differences wereound in bone resorption after the implants werelaced.17 Perry et al22 also compared DO and onlayrafting. The results in a canine model were similar tohose from the study by Chiapasco15 and showed noignificant difference between DO and onlay graft-ng.22
articulate Bone Augmentationith Membranes
The use of particulate bone with membrane cover-ge allows for both horizontal and vertical augmenta-ion of the mandible. The membrane is designed torevent infiltration of the particulate graft with con-ective tissue and allow bone to infiltrate into thearticulate graft mass rather than connective tissue,ith the formation of bone sufficient to support im-lants and, through implant functional loading, retainhe bone that has formed.23 A total of 3 to 6 mm ofertical bone augmentation has been reported.23,24 Aodified technique using dental implants left supra-
restal as “tent poles” with graft material packedround the implants resulted in stable bone forma-ion, especially when a titanium-reinforced titaniumembrane was used.23
One of the major concerns with particulate boneith membrane is that postoperative bone graft re-
orption is inhibited only as long as the membrane isn place but begins to resorb once the membranes removed.25-27 Therefore, numerous investigatorsave advocated leaving the membranes in place
or 9 months before exposure and implant place-ent23,24,28 or leaving the membrane in place for up
o 12 months.29
The main disadvantage of the use of membranes ishe premature exposure of the membrane throughhe mucosa. The subsequent infection of the graftedite will inhibit bone formation.15,16,29 The percent-ge of premature membrane exposure has rangedrom 0% to 37.5% (Rasmusson et al,25 0%; Tinti et al,29
3.6%; Artzi et al,24 20%; and Chiapasco et al,15
7.5%).The use of metallic mesh has been advocated to
orm and retain a particulate graft for vertical ridgeugmentation. Boyne et al30 used mesh to form a newaxillary ridge in patients with anterior combination
yndrome and others with an atrophic maxillaryidge. When the mesh did not become exposed earlyfter placement, the bone formation was predictable.hen the mesh became exposed during the healing
rocess, it required removal, which, depending onhe interval from placement, resulted in good or poorone ridge augmentation. The use of smaller meshores and more flexible mesh for posterior mandibu-
ar ridge augmentation has shown excellent results,

bccgmtt
sgtmttschrtafthh
i2bgtttoTap
fhlwssrrabtsstOi
bb
hduomosht
ibst
mpprewbtrgg
higrtrimTotwbaaotgtgrrcs
BLOCK AND HAGGERTY 33
ut the exposure of the mesh is still a factor toonsider.31 The use of a mesh-type material with aombination of graft materials, such as allograft, xeno-raft, synthetic scaffolds, and growth factors (boneorphogenetic protein, platelet-derived growth fac-
or) might have potential use for vertical ridge forma-ion, as new evidence becomes available.
INLAY–INTERPOSITIONAL PROCEDURES
Creating a horizontal osteotomy of an edentulousection of the mandible or maxilla with creation of aap between the segments has a long history in eden-ulous patients. When performed in the posteriorandible superior to the IAN, excellent stability of
he vertical augmentation has been achieved, al-hough the vertical augmentation is limited by thetretch of the soft tissue. DO has been used to in-rease the height of the ridge, because both soft andard tissue genesis occurs, deceasing the limitationsesulting from the soft tissue envelope. The lengthyime to achieve distraction of the superior segmentnd the occasional need for hard tissue grafting be-ore implant placement makes this method less attrac-ive for many patients. All the mentioned proceduresave specific indications and contraindications thatave been discussed.The concept of interpositional or “sandwich” graft-
ng is based on the theory that bone placed betweenpieces of pedicled bone with internal cancellous
one will undergo rapid and complete healing andraft incorporation.32,33 In 1966, Barros Saint Pas-eur34 described the interpostitional bone graftingechnique. Barros Saint Pasteur34 described a 2-stageechnique that involved a mandibular horizontal oste-tomy from the retromolar pad inferior to the IAN.hree weeks later, the cephalic portion was raisednd either plaster of Paris or a bovine allograft waslaced as an interpositional graft.34-36
Schettler37,38 proposed the “sandwich-technique”or vertical augmentation of the mandible, involving aorizontal osteotomy of the mandible, leaving the
ingual soft tissue attachments. The cephalic boneas raised, and autogenous grafting material was in-
erted in the defect, healing with minimal bone re-orption, regardless of the interpositional graft mate-ial used. At 30 months of follow-up, Schettler37,38
eported no bone resorption with autogenous bonend a 1-mm decrease in vertical height with bone-ank bone. Schettler and Hottermann39 then revisitedhe studies by Schettler using a rabbit model. The datahowed well-vascularized grafts after 6 weeks. Noignificant differences were seen histologically be-ween the autogenous and homologous bone grafts.39
ther studies also demonstrated rapid and complete
ncorporation when the grafted material was placed getween 2 corticocancellous segments of the mandi-le.32,33,40
A classic osteotomy method to augment the verticaleight of the anterior and posterior edentulous man-ible was introduced by Harle,41,42 and further eval-ated and modified by Stoelinga et al.43,44 The visorsteotomy involved a parasagittal osteotomy of theandible from body to body,41 with the lingual plate
f bone raised superiorly and pedicled to the lingualoft tissue. After 3 years, 36% vertical height relapsead occurred, and the average increase in height tohe anterior mandible was 7.8 mm.42
The classic sagittal visor osteotomy was modified tonclude a horizontal osteotomy in the anterior mandi-le, with autogenous bone placed within the interpo-itional gap. After 1 year, 20% of the vertical augmen-ation of the mandible had resorbed.43,44
A series was reported in which the IAN was re-oved from the canal, with a horizontal osteotomyerformed, including the ridge from the retromolarad to the retromolar pad, with the alveolar boneaised superiorly and immediately grafted with autog-nous corticocancellous bone and circum-mandibularire fixation.45 A vestibuloplasty was performed afterone healing, typically 12 to 16 weeks after the os-eotomy. After 8.8 months of follow-up, Frost et al45
eported graft resorption of 26.1% in the autogenousroup. All patients were reported to have some de-ree of neurosensory disturbances.45
Interpositional osteotomies in the alveolar boneeal with rapid vascularization and bone remodeling
n the bone gap.32 After 12 weeks, the interpositionalrafts were almost indistinguishable from the sur-ounding native bone. After 4 weeks, the lacunae ofhe grafted bone were empty, as expected. The mar-ow spaces contained cellular fibrous tissue contain-ng blood vessels. Signs of active osteogenesis with
inimal bone resorption were found in all specimens.he cranial segment was vital in all animals, and mostf the lacunae contained osteocytes. Attachment ofhe cranial segment to the graft was observed. At 12eeks, the grafts were fully incorporated into theone of the mandible. The lacunae of the graft werell empty, although new bone had been deposited onll surfaces of the graft. Little or no resorption hadccurred during the first 12 weeks. It was concludedhat with interpositional grafts, the osteocytes of theraft do not survive; however, the graft was wellolerated, and new bone quickly formed around theraft. The grafted bone was connected to the sur-ounding bone by new mineralized tissue. The supe-iorly repositioned bone segment maintained its vas-ular supply, demonstrating that the mobilizedegment received adequate circulation from the lin-
ual soft tissue pedicle to maintain its vitality.
taeomprtaosavmb
fitsBarafilpifiem
mc
rgmbccatmbmcsfr
cadAmpwaBnwTgss
N
O
P
D
I
B
34 INTERPOSITIONAL OSTEOTOMY
The visor osteotomies have been abandoned owingo the risk nerve damage and lack of bone retentionfter grafting.36,46,47 The high resorption rate of thesearly bone grafting procedures resulted from numer-us factors. Most early visor and sandwich osteoto-ies received vestibuloplasties. The disruption of theeriosteum of the grafted sites resulted in continuedesorption of the grafted area.47 Maloney et al47 foundhat by not performing a follow-up vestibuloplastyfter performing the Stoelinga-styled “3-piece osteot-mies,” less bone resorption occurred. A second rea-on for the bone loss could be attributed to the largerea of periosteal separation from the bone and theery large movement of bone, ranging from 10 to 20m, which might have gone beyond the effective
lood supply to the bone.These early grafting techniques used wire or suture
xation of the segments and grafts. Micromotion ofhe grafted area disrupts the vascular ingrowth andlows the osteogenic capabilities of the grafted area.one grafts secured both rigidly and nonrigidly inreas of low motion and high motion showed that theigidly fixed grafts maintained 56% of their volumefter 14 weeks compared with 46% for nonrigidlyxed grafts.48 When grafts were placed into areas of
ow motion versus areas of high motion and com-ared, only the high-motion sites showed significantly
mproved survival for the rigidly fixated group. Rigidxation exerts its most profound effects during thisarly phase of healing and should be used to eliminateovement of the graft during the early healing phase.When performing an interpositional osteotomy andoving the mobilized alveolar bone segment verti-
ally, the clinician must decide on the optimal mate-
Table 1. PROCEDURE COMPARISON FOR POSTERIOR M
Procedure
VerticalAugmentationLimits (mm) Main Adv
erve repositioning 0 Implant length canof ability to engagborder; stable boimplant
nlay grafting 7-10 Simple access, easedonor source: mahip
articulate bonewith membrane
5-8 Minimal morbidity,donor site
istractionosteogenesis
5-10 Genesis of soft tissubone augmentatio
nterpositionalosteotomy
4-8 One-stage procedurallograft; no dono
lock and Haggerty. Interpositional Osteotomy. J Oral Maxillofac Surg 2009.
ial to graft the defect. Cancellous/particulate marrowrafts have shown more rapid vascularization andore osteogenic activity compared with autogenous
lock grafts.49-52 Burchardt49 demonstrated that can-ellous grafts tend to repair completely with time, butortical grafts remain as a mixture of both necroticnd viable bone. Canzona et al53 studied the resorp-ion rates in inlay and onlay bone grafting in adultongrel dogs and concluded that inlay grafts survive
etter than do onlay grafts. Schettler and Hotter-ann39 believed that less bone resorption would oc-
ur with interpositional grafts because the graft isurrounded by bone and periosteum on all sides,acilitating a rapid vascular connection with the sur-ounding tissues.
INFLUENCE OF IMPLANTS ON BONEGRAFT RESORPTION
The rate of resorption of the grafted site decreasesonsiderably after implant placement.1,54 Bell et al1
ugmented both the anterior and the posterior man-ible with iliac bone using an extraoral approach.fter 6 months, implants were placed in the anteriorandible between the mental foramen but not in theosterior mandible. Vertical bone graft resorptionas found in the posterior nonimplant-supported
rea but not in the anterior implant-supported bone.reine and Branemark54 conducted a study on a ca-ine model in which autogenous composite graftsere placed containing integrated titanium implants.he results indicated that implant placement into arafted area results in graft persistence and implanttability. They concluded that implant placement canlow the resorption process. After the bone grafts had
BLE
Main Disadvantage
g becauseriorlong
High risk of neurosensory disturbance; longcrown/implant ratio for prosthesis
ation,, cranium,
Incision breakdown results in graft loss;graft resorption significant
or no Technically sensitive, incision breakdown ishigh with inexperienced clinicians,interval from graft to implant can be 9 mo
ellent Interval from start of distraction to implants,might need additional grafting; morbidityfrom distraction device
t can bemorbidity
Can be technically difficult; limitation ofaugmentation height because of soft tissuestretch
ANDI
antage
be lone infe
ne for
of fixndible
small
e, excn
e; grafr site

sp
stempv
“maonowbmolsrpppwfsl
tcatg
svrtl
Fr
B 2009.
Fi
BLOCK AND HAGGERTY 35
tabilized, the loss of the bone surrounding the im-lants was less than 0.1 mm/year.In long bones, the removal of load-bearing results in
ignificant bone remodeling, including endosteal, in-racortical, and, to a lesser extent, periosteal remod-ling.55 Without a load-bearing stimulus, the boneass declines, resulting in disuse osteoporosis. Ahysiologic dynamic strain or load is required to pre-ent the decline in bone mass after tooth extraction.In 2006, Jensen56 reported on interpositional or
sandwich” osteotomies in the posterior edentulousandible before implant placement. Jensen56 was
ble to achieve up to 8 mm of vertical augmentationf the posterior mandible using the sandwich tech-ique. The preoperative bone height was 3 to 7 mmf bone above the IAN canal. Horizontal osteotomiesere created 2 mm above the IAN canal. The lingual-ased flap was stretched superiorly 4 to 8 mm. Ainiplate was used for rigid fixation. A cortical wedge
f bone from the external oblique ridge and particu-ate autograft were placed in the interpositional graftite. After 4 months of healing, the miniplates wereemoved, and short implants (8 to 11 mm) werelaced. The implants were loaded 3 to 4 months afterlacement. The average vertical augmentation of theosterior mandible achieved with Jensen’s techniqueas 6 mm. Bone resorption was 0 to 1 mm at a
ollow-up of 1 to 4 years. Marchetti et al57 reportedimilar results, using autogenous cancellous particu-ate bone as the graft.
There are limitations to interpositional grafting forhe mandible (Table 1). Interpositional grafting onlyorrects vertical defects, not horizontal defects. Annatomic limitation also exists to the amount of ver-ical gain that can be achieved with interpositional
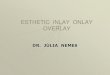
IGURE 1. Preoperative views showing presence of healthy anteriestorations without removal of her anterior teeth.
lock and Haggerty. Interpositional Osteotomy. J Oral Maxillofac Surg
rafting. This anatomic limitation is the stretch of theB2
oft tissue attachments to the pedicled mobilized al-eolar segment of bone, which can typically only beaised 5 to 8 mm. Undue strain on the lingual softissue pedicle by vertically repositioning the mobi-ized bone can lead to a compromised blood flow,
with bilateral posterior edentulism. Patient desired bilateral fixed
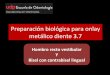
IGURE 2. Cone-beam cross-section computed tomography scan show-ng nerve canal high on ridge with 5.5 mm of bone coronal to canal.
or teeth
lock and Haggerty. Interpositional Osteotomy. J Oral Maxillofac Surg009.

iglorcdapa
C
ditrtse
Fdmcssdl5
B 2009.
36 INTERPOSITIONAL OSTEOTOMY
ncision breakdown, graft loss, and/or acceleratedraft resorption. By diligently respecting the anatomicimitations of the soft tissues, avoiding excessive peri-steal reflection, diligently applying the principles ofigid fixation, placing endosteal implants early in theonsolidation phase, dynamically loading the en-osteal implants, and using particulate grafts in theppropriate cases, interpositional grafting is a safe,redictable method of achieving 5 to 8 mm of verticalugmentation in the posterior mandible (Figs 1-11).
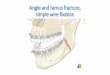
IGURE 3. Surgical procedure. Vestibular incision made with veissection performed until mental foramen identified. Periosteal incaintaining attachments on superior aspect of crest. At proposedutting device used to create osteotomy through labial and linguauperior segment. Careful raising of superior bone segment resuegment. Screw size was 1.2 mm in diameter, keeping screw profiesired position and secured to inferior portion of mandible. Unic
ingual portion of cortices to prevent sharp edges of bone. Interpo00-�m mineralized bone. After graft had been carefully placed,
lock and Haggerty. Interpositional Osteotomy. J Oral Maxillofac Surg
ase Studies
The patient presented with an intact anterior man-ible dentition in excellent health, with bilateral miss-
ng posterior teeth. She desired fixed restoration ofhe missing teeth and had had problems wearing aemovable partial denture. Her posterior maxillaryeeth were in the proper plane of occlusion withoutupraeruption. Her posterior interocclusal space wasxcessive. A cone-beam computed tomography scan
elease, 1 tooth anterior to edge of edentulous site. Mucosal-onlyade superior to foramen. Periosteum reflected inferiorly, carefullyl osteotomy sites, periosteum was minimally reflected. Piezotomeand in 2 vertical sites. Cuts were completed, resulting in mobile5 to 7 mm of bone augmentation. Small plate used to stabilizesmall. Plate was secured to superior segment first, then raised to
screws were used, not bicortical screws. Care was taken to alignl gap was grafted with particles of allograft, specifically, 350 ton was closed with resorbable sutures using tapered needles.
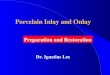
FIGURE 4. Two panoramic im-ages showing preoperative andpostoperative views.
Block and Haggerty. InterpositionalOsteotomy. J Oral Maxillofac Surg2009.
rtical rision mvertical bonelted inle very
orticalsitionaincisio

iaioiem
ptrtfTalimtgw
otdMbntrtw
hcp
Fo
B2
Fi
B2
Ft
B2
Fto
BLOCK AND HAGGERTY 37
ndicated 5 mm of bone superior to the IAN bilater-lly. The treatment options presented to the patientncluded a new removable partial denture, extractionf her remaining anterior teeth, with placement of 5
mplants for a fixed hybrid or fixed removable “sparkrosion”-type prosthesis, or interpositional osteoto-ies to vertically augment the posterior mandible.The cone-beam cross-section computed tomogra-
hy images were used to plan the procedure. Afterhe patient signed a consent form informing her of theisks of sensory nerve damage, failure to achieve ver-ical dimension, failure of the graft to consolidate, andailure of the implants, she was prepared for surgery.he patient was sedated for the procedure. Localnesthesia was administered into the vestibule of theeft and right posterior mandible. After a satisfactorynterval had elapsed for hemostasis, an incision was
ade in the unattached gingiva at least 10 mm lateralo the junction of the attached and unattached gin-iva. Anteriorly, the vestibular incision was joinedith a vertical incision made to the interdental areas
IGURE 5. Left posterior mandible 5 months after interpositionalsteotomy.
lock and Haggerty. Interpositional Osteotomy. J Oral Maxillofac Surg009.
IGURE 6. Right side of the posterior mandible 5 months afternterpositional osteotomy.
lock and Haggerty. Interpositional Osteotomy. J Oral Maxillofac Surg009.
B2
f the teeth anterior to the edentulous site. A full-hickness flap was developed and combined with theissection made from the lateral vestibular incision.ucosa-only dissection was performed sharply andluntly to isolate the nerve branches of the mentalerve. The periosteum was incised above the forameno avoid damage to the nerve. The periosteum waseflected only inferiorly, maintaining the periosteumo the superior aspect of the ridge. No lingual mucosaas elevated.A piezotome cutting tip was used to create the
orizontal osteotomy above the IAN canal. The verti-al cuts were made with minimal elevation of theeriosteum. The osteotomy cuts were made through
IGURE 7. The restorative dentist (D. Michael Shannon) made aemplate using the diagnostic setup of the planned restoration.
lock and Haggerty. Interpositional Osteotomy. J Oral Maxillofac Surg009.
IGURE 8. A crestal incision was made, and periosteum reflectedo expose plate. Note excellent bone formation within gap ofsteotomy. The plate was then removed.
lock and Haggerty. Interpositional Osteotomy. J Oral Maxillofac Surg009.

ttpccvtgwtswwlw
Tac
anafip
R
Fn
B2
B2
B2
38 INTERPOSITIONAL OSTEOTOMY
he lingual cortical bone. Osteotomes were not usedo prevent shearing of the lingual bone. A finger waslaced over the lingual mucosa to feel the piezotomeutting blade exit the bone but not the lingual mu-osa. The segment was mobilized passively and ele-ated to the extent of the soft tissue attachments. Ifhe floor of mouth is high, the elevation can bereater than if the floor of mouth is low. The segmentas elevated, and a small bone plate was attached first
o the superior mobilized segment of the crest. Thecrew size was usually 1.2 or 1.5 mm. After the plateas secured to the mobilized segment, the segmentas elevated and oriented to minimize bone irregu-
arities on the lingual mucosa, and the final screwsere placed in the inferior mandibular intact bone.
IGURE 9. Right side showing excellent bone formation and intactewly augmented mandibular ridge.
lock and Haggerty. Interpositional Osteotomy. J Oral Maxillofac Surg009.
FIGURE 10. Three implants in position in the left posterior mandible.
lock and Haggerty. Interpositional Osteotomy. J Oral Maxillofac Surg009.
he space was grafted with a freeze-dried mineralizedllograft. After the graft was placed, the incision waslosed without tension.The patient was instructed to consume a liquid diet
nd was given antibiotics. Antibacterial rinses wereot started until 3 days after surgery. After 3 months,new computed tomography scan was taken to con-rm bone consolidation, and the implants werelaced in a routine manner.
eferences1. Bell RB, Blakey GH, White RP, et al: Stages reconstruction of
the severely atrophic mandible with autogenous bone graft andendosteal implants. J Oral Maxillofac Surg 60:1135, 2002
2. Maloney F, Tideman H, Stoelinga PJW, et al: Interpostitionalbone-grafting of the atrophic edentulous mandible: A review.Aust Dent J 30:211, 1985
3. Tallgren A: The continued reduction of the residual alveolarridges in complete denture wearers: A mixed longitudinalstudy covering 25 years. J Prosthet Dent 27:120, 1972
4. Davis H, Rydevik B, Lundborg G, et al: Mobilization of theinferior alveolar nerve to allow placement of osseointegratedfixtures, in Worthington P, Branemark P-I (eds): AdvancedOsseointegration Surgery: Applications in the Maxillofacial Re-gion. Chicago: Quintessence, 1992, pp 129-144
5. Proussaefs P: Vertical alveolar ridge augmentation prior toinferior alveolar nerve repositioning: A patient report. Int J OralMaxillofac Implants 20:296, 2005
6. Friberg B, Ivanoff CJ, Lekholm U: Inferior alveolar nerve trans-positioning in combination with Branemark implant treatment.Int J Periodontics Restorative Dent 12:440, 1992
7. Haers PE, Sailer HF: Neurosensory function after lateralizationof the inferior alveolar nerve and simultaneous insertion ofimplants. Oral Maxillofac Surg Clin North Am 7:707, 1994
8. Kan JYK, Lozada JL, Goodacre CJ, et al: Endosseous implantplacement in conjunction with inferior alveolar nerve transpo-sition: An evaluation of neurosensory disturbance. Int J OralMaxillofac Implants 12:463, 1997
9. Kan JYK, Lozada JL, Boyne PJ, et al: Mandibular fracture afterendosseous implant placement in conjunction with inferior
FIGURE 11. Two implants placed into the right side of the mandible.
lock and Haggerty. Interpositional Osteotomy. J Oral Maxillofac Surg009.
alveolar nerve transposition: A patient treatment report. IntJ Oral Maxillofac Implants 12:655, 1997

1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
4
4
5
5
5
5
5
5
5
5
BLOCK AND HAGGERTY 39
0. Bovi M: Mobilization of the inferior alveolar nerve with simul-taneous implant insertion: A new technique. Case report. Int JPeriodontics Restorative Dent 25:375, 2005
1. Jensen OT, Nock D: Inferior alveolar nerve repositioning inconjunction with placement of osseointegrated implants: Acase report. Oral Surg Oral Med Oral Pathol 63:263, 1987
2. Block MS, Delgado A, Fontenot MG: The effect of diameter andlength of hydroxylapatite coated dental implants on ultimatepull out force in dog alveolar bone. J Oral Maxillofac Surg48:174, 1990
3. Block MS, Kent JN: Cylindrical HA-coated implants, eight yearobservations. Compend Contin Educ Dent Suppl 15:526, 1993
4. Jaffin RA, Berman CL: The excessive loss of Branemark fixturesin type IV bone: A 5 year analysis. J Periodontol 62:2, 1991
5. Chiapasco M, Romeo E, Casentini P, et al: Alveolar distractionosteogenesis vs. vertical guided bone regeneration for thecorrection of vertically deficient edentulous ridges: A 1-3 yearprospective study on humans. Clin Oral Implants Res 15:82,2004
6. Simion M, Baldoni M, Rossi P, et al: A comparative study of theeffectiveness of e-PTFE membranes with and without earlyexposure during the healing period. Int J Periodontics RestDent 14:167, 1994
7. Chiapasco M, Zaniboni M, Rimondini L: Autogenous onlaybone grafts vs. alveolar distraction osteogenesis for the correc-tion of vertically deficient edentulous ridges: A 2-4 year pro-spective study on humans. Clin Oral Implants Res 18:432, 2007
8. Cordaro L, Amade DS, Cordaro M: Clinical results of alveolarridge augmentation with mandibular block bone grafts in par-tially edentulous patients prior to implant placement. Clin OralImplants Res 13:103, 2002
9. Proussaefs P, Lozada J, Kleinman A, et al: The use of ramusautogenous block grafts for vertical alveolar ridge augmenta-tion and implant placement: A pilot study. Int J Oral MaxillofacImplants 17:238, 2002
0. Proussaefs P, Lozada J: The use of intraorally harvested autog-enous block grafts for vertical alveolar ridge augmentation: Ahuman study. Int J Periodontics Restorative Dent 25:351, 2005
1. Pikos MA: Mandibular block autografts for alveolar ridge aug-mentation. Atlas Oral Maxillofac Surg Clin 13:91, 2005
2. Perry M, Hodges N, Hallmon W, et al: Distraction osteogenesisversus autogenous onlay grafting. Part I: Outcome of implantintegration. Int J Oral Maxillofac Implants 20:695, 2005
3. Simion M, Trisi P, Piattelli A, et al: Augmentation using amembrane technique associated with osseointegrated im-plants. Int J Periodont Rest Dent 14:497, 1994
4. Artzi Z, Dayan D, Alpern Y, et al: Augmentation using xeno-genic material supported by a configuring titanium mesh: Clini-cohistopathologic and histochemical study. Int J Oral Maxillo-fac Implants 18:440, 2003
5. Rasmusson L, Meridith N, Kahnberg KE, et al: Effects of barriermembranes on bone resorption and implant stability in onlaybone grafts. Clin Oral Implants Res 10:267, 1999
6. Jensen OT, Greer RO, Jonsson L, et al: Vertical guided bone-graft augmentation in a new canine mandibular model. IntJ Oral Maxillofac Implants 10:335, 1995
7. Gordh M, Alberius P, Johnell O, et al: Osteopromotive mem-branes enhance onlay integration and maintenance in the adultrat skull. Int J Oral Maxillofac Surg 27:67, 1998
8. Buser D, Dahlin C, Schenk R: Guided Bone Regeneration inImplant Dentistry. Chicago: Quintessence Publishing, 1994
9. Tinti C, Parma-Benfenati S, Ridge V: Augmentation: Surgicalprotocol and retrospective evaluation of 48 consecutively in-serted implants. Int J Periodont Rest Dent 18:435, 1998
0. Boyne PJ, Cole MD, Stringer D, et al: A technique for osseousrestoration of deficient edentulous maxillar ridges. J Oral Max-illofac Surg 43:87, 1985
1. Louis PJ, Gutta R, Said-Al-Naief N, et al: Reconstruction of themaxilla and mandible with particulate bone graft and titaniummesh for implant placement. J Oral Maxillofac Surg 66:235,2008
2. Frame JW, Brady CL, Browne RM, et al: Augmentation of theedentulous mandible using bone graft and hydroxyapatite: A
comparative study in dogs. Int J Oral Surg Suppl 10:88, 19813. Frame JW, Browne RM, Brady CL: Biologic basis for interposi-tional autogenous bone grafts to the mandible. J Oral Maxillo-fac Surg 40:407, 1982
4. Barros Saint Pasteur J: Plastic restoration of the alveolar crest ofthe mandible. Acta Odontol Venez 4:3, 1966
5. Barros Saint Pasteur J: Plastic reconstruction of the alveolarcrest: Clinico-surgical investigation. Acta Odontol Venez 8:168,1970
6. Egbert M, Stoelinga P, Blijdorp P, et al: The “three-piece”osteotomy and interpositional bone graft for augmentation ofthe atrophic mandible. J Oral Maxillofac Surg 44:680, 1986
7. Schettler D: Sandwich-technique with cartilage transplant forraising the alveolar process in the lower jaw. Fortschr KieferGesichts Chir 20:61, 1976
8. Schettler D: Spatergebnisse der absoluten kieferkammerho-hung im atrophischen Unterkiefer durch die “sandwichplas-tik.” Dtsch Zahnarztle Z 37:132, 1982
9. Schettler D, Hottermann W: Clinical and experimental resultsof a sandwich-technique for mandibular alveolar ridge augmen-tation. J Maxillofac Surg 5:199, 1977
0. Canzona JE, Grand NG, Waterhouse JP: Autogenous bone graftsin augmentation of the edentulous canine mandible. J Oral Surg34:879, 1976
1. Harle F: Visor osteotomy to increase the absolute height of theatrophied mandible: A preliminary report. J Maxillofac Surg3:257, 1975
2. Harle F: Follow-up investigation of surgical correction of theatrophic alveolar ridge by visor osteotomy. J Maxillofac Surg7:283, 1979
3. Stoelinga JPW, Tideman H, Berger JS, et al: Interpostitionalbone-graft augmentation of the atrophic mandible: A prelimi-nary report. J Oral Surg 36:30, 1978
4. Stoelinga PJW, de Koomen HA, Tideman H, et al: A reappraisalof the interposed bonegraft augmentation of the atrophic man-dible. J Maxillofac Surg 11:107, 1983
5. Frost DE, Gregg JM, Terry BC, et al: Mandibular interpositionaland onlay bone grafting for the treatment of mandibular bonydeficiency in the edentulous patient. J Oral Maxillofac Surg40:353, 1982
6. Sugar A, Hopkins R: A sandwich mandibular osteotomy: Aprogress report. Br J Oral Surg 20:168, 1982
7. Maloney F, Steolinga PJW, Tideman H, et al: Recent develop-ments in interpositional bone-grafting of the atrophic mandi-ble. J Maxillofac Surg 13:14, 1985
8. Lin KY, Bartlett SP, Yaremchuk MJ, et al: The effect of rigidfixation on the survival of onlay bone grafts: An experimentalstudy. Plast Resonstr Surg 86:449, 1990
9. Burchardt H: The biology of bone graft repair. Clin OrthopRelat Res 174:28, 1983
0. Marciani RD, Conty AA, Synhorst JB, et al: Cancellous bonemarrow grafts in irradiated dog and monkey mandibles. J OralSurg 47:17, 1979
1. Hammack BL, Enneking WF: Comparative vascularization ofautogenous and homogenous bone transplants. J Bone JointSurg (Am) 42:811, 1960
2. Enneking WF, Eady JL, Burchardt H: Autogenous cortical bonegrafts in the reconstruction of segmental skeletal defects.J Bone Joint Surg (Am) 62:1039, 1980
3. Canzona JE, Grand NG, Waterhouse JP: Autogenous bone graftsin augmentation of the edentulous canine mandible. J Oral Surg34:879, 1976
4. Breine U, Branemark PI: Reconstruction of the alveolar jawbone. Scand J Plast Reconstr Surg 14:23, 1980
5. Rubin CT, Lanyon LE: Regulation of bone formation by applieddynamic loads. J Bone Joint Surg Am 66:397, 1984
6. Jensen OT: Alveolar segmental “sandwich” osteotomies forposterior edentulous mandibular sites for dental implants.J Oral Maxillofac Surg 64:471, 2006
7. Marchetti C, Trasarti S, Corinaldesi G, et al: Interpositionalbone grafts in the posterior mandibular region: A report on six
patients. Int J Periodontics Restorative Dent 27:547, 2007