Embed Size (px)
Citation preview

www.thelancet.com/oncology Vol 15 February 2014 e90
Review
International variations in childhood cancer in indigenous populations: a systematic reviewPatricia C Valery, Suzanne P Moore, Judith Meiklejohn, Freddie Bray
Although the cancer burden in indigenous children has been reported in some countries, up to now, no international comparison has been made. We therefore aimed to assess the available evidence of the burden of childhood cancer in indigenous populations. We did a systematic review of reports on cancer incidence, mortality, and survival in indigenous children worldwide. Our fi ndings highlight the paucity of accessible information and advocate the pressing need for data by indigenous status in countries where population-based cancer registries are established. The true extent of disparities between the burden in the indigenous community needs to be measured so that targeted programmes for cancer control can be planned and implemented.
IntroductionThere are an estimated 300–500 million indigenous people worldwide.1 The prevailing understanding of the term indigenous is that no formal universal defi nition is necessary because one defi nition will be either overinclusive or underinclusive, making sense in some societies but not in others.1 Nevertheless, the present understanding of the term indigenous used by the UN is that provided by José Martínez Cobo.2 As described by the International Work Group for Indigenous Aff airs (IWGIA), the term includes self-identifi cation, acceptance by the community, historical continuity with pre-settler societies, strong link with land, practice of unique traditions, and social, cultural, economic, and political characteristics that are distinct from those of the dominant societies in which the individual lives.2 Some populations are undisputedly recognised as indigenous (eg, Maori in New Zealand), but for others that consider themselves indigenous, their claim is not always recognised (eg, some ethnic groups in Africa).
International variations in the incidence of childhood cancer have been documented extensively,3–6 as have diff erences by ethnic origin and indigenous status in some countries such as the USA,7,8 UK,9 Australia,10 and New Zealand.11,12 However, data for childhood cancer mortality by ethnic origin are scarce and incon sistent.8,13–15 The eff ect of ethnic origin and socio economic status on the survival of children with cancer has been investigated in the UK,16,17 USA,8,18,19 and New Zealand,20 albeit with inconsistent results.
Although some studies have been done on the burden of childhood cancer in indigenous children in specifi c countries, international comparisons have not been reported. The diff erences across and within countries might have been aff ected by quality and accuracy of the cancer statistics—eg, when recording of indigenous identifi ers is incomplete in registry or population data,10 or the completeness of the cancer diagnosis and reporting is inadequate. We aimed to assess the available evidence of the burden of childhood cancer in indigenous populations.
Data collectionWe did a systematic review and included studies reporting cancer incidence, mortality, and survival in indigenous
children worldwide, published between Jan 1, 1980, and May 31, 2013. We chose Jan 1, 1980, as a cutoff because of diff erences in diagnostic practices and treatments and classifi cation of cancer types in older reports, and the logistics of retrieving very old publications that are usually not available online. For incidence and mortality, we included studies that used data from population-based or hospital-based registries, and that reported crude, age-specifi c, or age-adjusted incidence, or mortality rates or provided suffi cient information to enable their calculation.
One author (PCV) searched online peer-reviewed journal articles indexed in PubMed, Medline, CINAHL, and SciELO. We selected citations including neoplasms in the medical subject headings terms, or cancer; and incidence, mortality, or survival; and child, childhood, infant, or children; and “population groups” in the medical subject headings terms, or indig*, ethn*, Aborigin*, Maori*, Mapuche, Alaska*, Inuit, Indian*, native, or Africa* in either the title or abstract. We complemented the search by manual review of the references of retrieved articles. We identifi ed populations as indigenous if they met the criteria described provided by the Martínez Cobo report and the IWGIA.2 We considered up to 283 indigenous terms for inclusion in the aforementioned list. The appendix describes the rationale for choosing the specifi c indigenous terms.
Two investigators (PCV and JM) independently reviewed all titles; we assessed those judged to be potentially helpful. The following selection criteria were then applied: availability of an abstract; use of primary data; and published in English, Spanish, French, or Portuguese language. We selected abstracts with relevant content for full manuscript review. PCV and JM independently reviewed manuscripts; SPM adjudicated disagreements. We excluded reviews and editorials and reports for which incidence, mortality, or survival were not reported or calculable. Reports that contained mostly adult data were included if rates were reported (or calculable) separately for children. In addition to crude rates, the selected studies used several diff erent standard populations to adjust for the eff ects of age. To ensure valid comparisons across studies, we did a sensitivity analysis to study the potential eff ect of
Lancet Oncol 2014; 15: e90–103
Menzies School of Health Research, Charles Darwin University, Darwin, NT, Australia (P C Valery PhD, J Meiklejohn MAppSc); and Section of Cancer Information, International Agency for Research on Cancer, Lyon, France (P C Valery, S P Moore PhD, F Bray PhD)
Correspondence to: Dr Patricia C Valery, Menzies School of Health Research, Spring Hill, Brisbane, QLD 4000, [email protected]
For more on the IWGIA see http://www.iwgia.org/iwgia
See Online for appendix

e91 www.thelancet.com/oncology Vol 15 February 2014
Review
diff erent weightings on the relative magnitude of the age-standardised incidence rates for ages 0–14 years (appendix).
With the US data obtained from the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) programme, we compared incidence rates for all cancers adjusted to the world standard population with those adjusted to the 1970 and 2000 US populations. We estimated that if age-standardised incidence rates for the diff erent standards presented (US 1970 and 2000 populations) were adjusted solely to the world standard population, age-standardised incidence rates would be maximally higher by 5%; these age-standardised incidence rates were 3% higher than the corresponding crude rates.
Additional incidence and mortality data for Australia were obtained from the report by Valery and colleagues10 and the Australian Paediatric Cancer Registry. Population estimates were obtained from the Australian Bureau of Statistics.21 We obtained incidence (2000–09), mortality data (1990–2009), and corresponding population estimates for the USA from the SEER programme. Data for incidence (2005–09) and mortality (1998–2002), and corresponding population estimates for New Zealand Maoris were obtained from New Zealand Heath Statistics. We obtained incidence data and population estimates for Nigeria from Junaid and colleagues.22
To compare rates between these populations, we calculated age-standardised rates (adjusted to the world standard population) for ages 0–14 years (unless otherwise stated) from nine countries and expressed per million per year.23 We used the Poisson approximation method of calculation of standard error to calculate 95% CIs.24 We used a descriptive approach to compare reports.
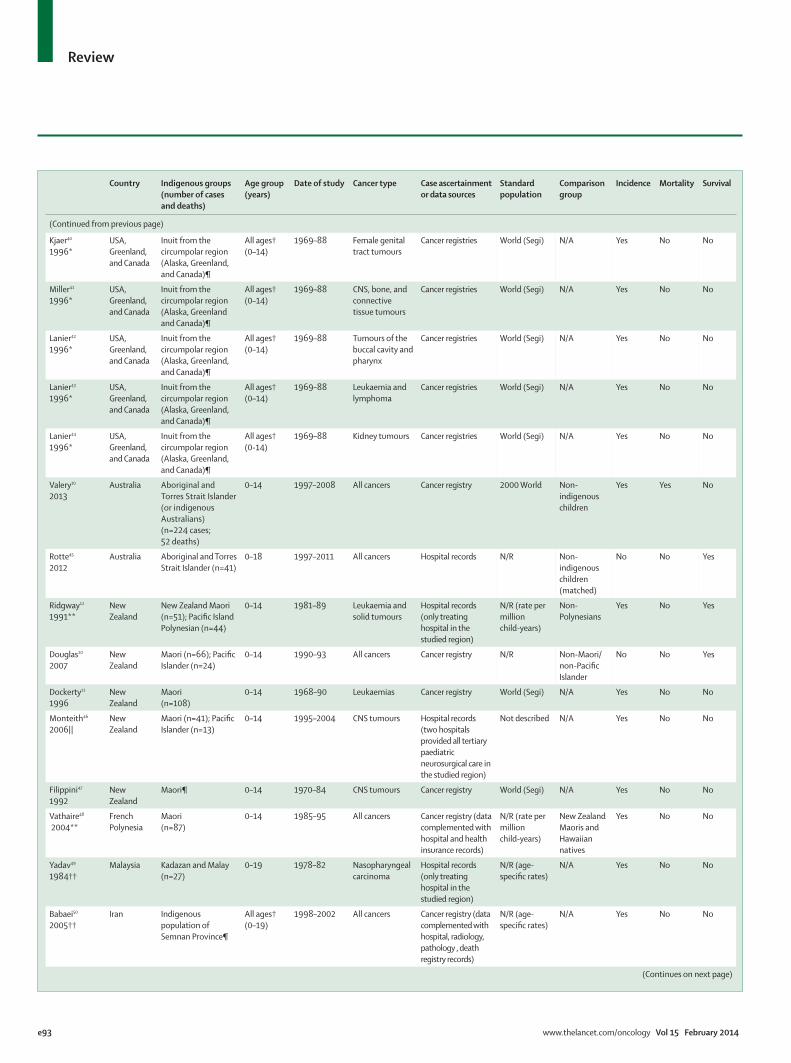
FindingsThe initial search yielded 3048 reports: 41 were relevant for our Review. We found three additional studies after reviewing the reference lists of relevant articles (fi gure 1, table 1). We included indigenous children from three main regions: Native Americans (American Indians, Alaska natives, and Hawaiians) in the USA, indigenous children from the Asia–Pacifi c region (Indigenous Australians, Maori, and Pacifi c Islanders in New Zealand and French Polynesia), and from selected African countries. In six studies,12,46,49,54,55,58 cases were ascertained from hospitals; these hospitals provided all paediatric cancer care in the studied region and reference population estimates were available. Age-specifi c incidence rates (age 0–4, 5–9, 10–14, and 15–19 years) were reported in ten studies.27,39,40–44,49–51
IncidenceAll cancers combinedOverall incidence of childhood cancers in indigenous children was reported in six US studies8,25–29 (table 1); four of these studies8,26,28,29 each reported more than 100 cases (table 2). The remaining two studies25,27 included small numbers of American Indians (table 2). We noted no signifi cant diff erences in overall incidence between Hawaiian,26,28 American Indian, 29 and Alaska native children29 and white children from the USA. Lanier and colleagues8 reported no signifi cant diff erence in overall incidence between white children from the USA and Alaska natives, whereas incidence in American Indians was 30% lower.8 Comparisons with white children were not done for the remaining two studies.
In the Asia–Pacifi c region, age-standardised incidence rates in indigenous children from Australia,10 New Zealand,12 and French Polynesia48 ranged from 85 per million per year to 125 per million per year. Compared with non-indigenous Australians, indigenous children were 36% less likely to be diagnosed with cancer (p<0·001) than were non-indigenous children, with incidence signifi cantly lower for leukaemias, CNS, renal, and bone tumours.10 Overall incidence was similar for Maori, Pacifi c Islander Polynesian, and non-Polynesian children12 (table 2). Compared with New Zealand Maoris and natives from Hawaii, Maori from French Polynesia had 20% fewer cancers (p<0·05). Vathaire and colleagues48 reported a standardised incidence ratio (SIR) of 0·8 (95% CI 0·7–1·0) for natives of French Polynesia compared with New Zealand Maoris and an SIR of 0·8 (0·6–1·0) when compared with natives from Hawaii. Incidences for New Zealand Maoris and natives from Hawaii were not reported.
Four African studies reported overall childhood cancer incidence in indigenous children. Rates for Namibia and Nigeria ranged from 47 cases per million children in Herero52 to 198 cases per million in Yoruba boys.22 Crude rates were available for Zimbabwe and Mali; incidence rates for African children in Harare53 and for children from several ethnic groups in
For more on SEER see http://seer.cancer.gov/seerstat/
3048 titles identified and screened for eligibility
479 potentially eligible abstracts assessed in more detail
2569 titles excluded 168 no abstract 1431 title not relevant 970 duplicate titles
179 potentially eligible articles assessed in more detail
44 eligible articles included in the review
300 abstracts excluded (content not relevant)
138 articles excluded 128 content not relevant 10 articles could not be sourced
3 articles found through manual review of references of retrieved articles
Figure 1: Summary of the eligibility criteria for inclusion in the Review
For New Zealand Heath Statistics see http://www.health.govt.nz/?nz-health-
statistics

www.thelancet.com/oncology Vol 15 February 2014 e92
Review
Country Indigenous groups (number of cases and deaths)
Age group (years)
Date of study Cancer type Case ascertain ment or data sources
Standard population
Comparison group
Incidence Mortality Survival
Duncan25
1986USA New Mexican
American Indians (n=38)
0–14 1970–82 All cancers Cancer registry 1970 USA N/A Yes No No
Goodman26
1989USA Hawaiians
(n=173)0–14 1960–84 All cancers Cancer registry World (Segi) White
children in the USA
Yes No No
Norsted27
1989*USA Native Americans
(n=11)All ages† (0–14)
1974–83 All cancers Cancer registry NR (age-specifi c rates)
N/A Yes No No
Lanier8 2003 USA Alaska natives (n=131 cases; 23 deaths) and New Mexican American Indians (n=148)
0–19 Incidence: Alaska natives 1969–96; New Mexican American Indians 1973–96; mortality: Alaska natives 1979–96
All cancers Cancer registry, and death data from the bureau of statistics
1970 US White children in the USA
Yes Yes Yes
Wenceslao28
2006USA Hawaiians
(n=379)0–19 1975–2000 All cancers Cancer registry World (Segi) White
children in the USA
Yes No No
Pollack14
2007USA Alaska natives and
American Indians (41 deaths)
0–19 1990–2004 All cancers Death data from the bureau of statistics
2000 US N/A No Yes No
Li29
2008USA Alaska natives and
American Indians (n=273)
0–19 2001–003 All cancers Cancer registry 2000 US N/A Yes No No
Goodman30
1989USA Hawaiians
(n=59)0–14 1960–84 Leukaemia Cancer registry World (Segi) White
children in the USA
Yes No No
Foucar31
1991USA New Mexican
American Indians (n=28)
0–19 1969–86 Leukaemias Cancer registry and hospital records
N/R Hispanic and non-Hispanic white children
No No Yes
Kadan-Lottick32 2003
USA Alaska natives and American Indians (n=61)
0–19 1973–99 Acute lymphoblastic leukaemia
Cancer registry N/R White children in the USA
No No Yes
Goggins33
2012USA Alaska natives and
American Indians (n=116)
0–19 1988–2008 Acute lymphoblastic leukaemia
Cancer registry N/R White children in the USA
No No Yes
Berkow34
1983‡USA New Mexico Navajo
Indians(n=6)
0–7 1966–81 Retinoblastoma Cancer registry, health records, and death certifi cate data
N/R(crude rates)
N/A Yes No No
Walsh35
2008USA Alaska natives and
American Indians (n=6)
0–14 1992–2004 Testicular germ tumours
Cancer registry 2000 US N/A Yes No No
Henderson36
2011USA American Indians
(n=28)0–19§ 2001–09 Neuroblastoma Hospital records N/R White
children in the USA
No No Yes
Johnson37
2011USA Alaska natives and
American Indians (n=118)
0–19 1985–2005 Extracranial solid tumours
Cancer registry N/R White children in the USA
No No Yes
McMahon38
2011USA Alaska natives
(n=17)All ages†(0–19)
1969–2008 Liver tumours Cancer registry and hepatocellular carcinoma surveillance programme
Not described N/A Yes No No
Prener39
1996*USA, Greenland, and Canada
Inuit from the circumpolar region (Alaska, Greenland, and Canada)¶
All ages†(0–14)
1969–88 Male genital tract tumours
Cancer registries World (Segi) N/A Yes No No
(Continues on next page)
e93 www.thelancet.com/oncology Vol 15 February 2014
Review
Country Indigenous groups (number of cases and deaths)
Age group (years)
Date of study Cancer type Case ascertain ment or data sources
Standard population
Comparison group
Incidence Mortality Survival
(Continued from previous page)
Kjaer40
1996*USA, Greenland, and Canada
Inuit from the circumpolar region (Alaska, Greenland, and Canada)¶
All ages†(0–14)
1969–88 Female genital tract tumours
Cancer registries World (Segi) N/A Yes No No
Miller41
1996*USA, Greenland, and Canada
Inuit from the circumpolar region (Alaska, Greenland and Canada)¶
All ages†(0–14)
1969–88 CNS, bone, and connective tissue tumours
Cancer registries World (Segi) N/A Yes No No
Lanier42
1996*USA, Greenland, and Canada
Inuit from the circumpolar region (Alaska, Greenland, and Canada)¶
All ages†(0–14)
1969–88 Tumours of the buccal cavity and pharynx
Cancer registries World (Segi) N/A Yes No No
Lanier43
1996*USA, Greenland, and Canada
Inuit from the circumpolar region (Alaska, Greenland, and Canada)¶
All ages†(0–14)
1969–88 Leukaemia and lymphoma
Cancer registries World (Segi) N/A Yes No No
Lanier44
1996*USA, Greenland, and Canada
Inuit from the circumpolar region (Alaska, Greenland, and Canada)¶
All ages†(0-14)
1969–88 Kidney tumours Cancer registries World (Segi) N/A Yes No No
Valery10
2013Australia Aboriginal and
Torres Strait Islander (or indigenous Australians) (n=224 cases; 52 deaths)
0–14 1997–2008 All cancers Cancer registry 2000 World Non-indigenous children
Yes Yes No
Rotte45
2012Australia Aboriginal and Torres
Strait Islander (n=41)0–18 1997–2011 All cancers Hospital records N/R Non-
indigenous children (matched)
No No Yes
Ridgway12
1991**New Zealand
New Zealand Maori (n=51); Pacifi c Island Polynesian (n=44)
0–14 1981–89 Leukaemia and solid tumours
Hospital records (only treating hospital in the studied region)
N/R (rate per million child-years)
Non-Polynesians
Yes No Yes
Douglas20
2007New Zealand
Maori (n=66); Pacifi c Islander (n=24)
0–14 1990–93 All cancers Cancer registry N/R Non-Maori/non-Pacifi c Islander
No No Yes
Dockerty11
1996New Zealand
Maori(n=108)
0–14 1968–90 Leukaemias Cancer registry World (Segi) N/A Yes No No
Monteith46
2006||New Zealand
Maori (n=41); Pacifi c Islander (n=13)
0–14 1995–2004 CNS tumours Hospital records (two hospitals provided all tertiary paediatric neurosurgical care in the studied region)
Not described N/A Yes No No
Filippini47
1992New Zealand
Maori¶ 0–14 1970–84 CNS tumours Cancer registry World (Segi) N/A Yes No No
Vathaire48
2004**French Polynesia
Maori(n=87)
0–14 1985–95 All cancers Cancer registry (data comple mented with hospital and health insurance records)
N/R (rate per million child-years)
New Zealand Maoris and Hawaiian natives
Yes No No
Yadav49
1984††Malaysia Kadazan and Malay
(n=27)0–19 1978–82 Nasopharyngeal
carcinomaHospital records(only treating hospital in the studied region)
N/R (age-specifi c rates)
N/A Yes No No
Babaei50
2005††Iran Indigenous
population of Semnan Province¶
All ages†(0–19)
1998–2002 All cancers Cancer registry (data comple mented with hospital, radiology, pathology , death registry records)
N/R (age-specifi c rates)
N/A Yes No No
(Continues on next page)

www.thelancet.com/oncology Vol 15 February 2014 e94
Review
Bamako ranged from 96 cases per million to 156 cases per million.61 Comparison of incidences between indigenous and non-indigenous children were only
available for Namibia where 10% of cases were non-indigenous. Incidences were not signifi cantly diff erent; the only exceptions were higher rates of osteosarcoma
Country Indigenous groups (number of cases and deaths)
Age group (years)
Date of study Cancer type Case ascertain ment or data sources
Standard population
Comparison group
Incidence Mortality Survival
(Continued from previous page)
Mouratova51 2003*
Uzbekistan Kazakhs (n=59) and Karakalpaks (n=22)
0–14 1978–99 Retinoblastoma Cancer registry N/R (age-specifi c rates)
N/A Yes No No
Wessels52
1996Namibia Wambo, Kavango,
and Herero(n=120)
0–14 1983–88 All cancers Cancer registry(data comple-mented with hospital, death certifi cates, and pathology records)
World (Segi) All childhood cancer cases
Yes No No
Junaid22
1988‡‡Nigeria Yoruba (n=183 boys,
n=99 girls)All ages†(0–14)
1960–69 All cancers Cancer registry Not described N/A Yes No No
Chokunonga53
2000§§¶¶Zimbabwe African children
(n=80 boys, n=65 girls)
All ages†(0–14)
1993–95 All cancers Cancer registry Parkin 1997 (IARC vol 143)
N/A Yes No No
Makata54
1996‡Kenya Several ethnic
groups; Luo (n=261) and Luhya (n=104)
0–14 1979–94 Solid tumours Hospital records (three hospitals received all surgical biopsy specimens in the studied region)
N/R(crude rates)
N/A Yes No No
Mwanba55
2004Kenya Several ethnic
groups; Luo (n=282) and Luhya (n=231)
All ages†(0–15)
1988–97 Burkitt’s lymphoma
Hospital records(one referral and seven provincial hospitals that treated all cancer cases in the studied region)
All childhood cancer cases
Yes No No
Davidson56
2006South Africa Blacks
(n=79)0–19 1979–2003 Wilms’ tumour Hospital records N/R White and
coloured children from South Africa
No No Yes
Stefan57
2009South Africa Blacks
(n=78)0–14 1986–2006 Hodgkin’s
lymphomaHospital records N/R White and
coloured children from South Africa
No No Yes
Macdougal58 1986‡
South Africa Black children(n=78; ALL n=41; ANLL n=37)
0–14 1974–82 Leukaemia Hospital records(two referral hospitals that treated all children with leukaemia in the studied region)
N/R(crude rates)
White and coloured children from South Africa
Yes No Yes
Hesseling59
1995South Africa and Namibia
Black children(n=12)
0–14 1983–93 Leukaemia Hospital records N/R White children
No No Yes
Hesseling60
1999South Africa and Namibia
Black children(n=15)
0–14 1983–97 Neuroblastoma Hospital records N/R White children
No No Yes
Bayo61
1990†¶¶Mali Several ethnic groups
(n=37)All ages†(0–14)
1987–88 All cancers Cancer registry(data comple-mented with hospital records and death certifi cates)
N/R(crude rates were calculable)
N/A Yes No No
ASIR=age-standardised incidence rate. N/A=comparison data not available. N/R=not relevant. IARC=International Agency for Research on Cancer. *Age-standardised incidence rates for children aged 0–14 years were calculated based on reported age-specifi c rates. †Mostly adult data but some information for children available. ‡Crude incidence rates only. §Reported as “included children and young adults”, assumed to be age 0–19 years. ¶Number of indigenous children with cancer not reported. ||Incidence seemed to be age-standardised but details not included in Methods. **Incidence presented per child-years. ††Age-standardised incidence rates for children aged 0–19 years were calculated based on reported age-specifi c rates. ‡‡Included here because most of the population in Iaban are Yoruba people and the registry separated Ibadan from non-Ibadan residents for calculation of rates. §§Included here because most of the population (96%) are black Africans. ¶¶Enough information to calculate crude incidence rates.
Table 1: Studies included in the literature review

e95 www.thelancet.com/oncology Vol 15 February 2014
Review
in Kavango children and CNS tumours in children from Herero.52
Figure 2 shows the age-standardised incidence rates of all childhood cancers by indigenous group plotted alongside the timeline when cases were diagnosed (data were presented from reports in which incidence for all cancers was based on 44 cases or more). Data from indigenous children in the USA, New Zealand, and Australia whose cancer was diagnosed in 2000 or later suggested the age-standardised incidence rates ranged from 92 to 123 per million per year (fi gure 2).
We further examined the types of cancers reported in indigenous populations from the studies that reported all cancer incidence, if cancer types were listed. In the USA, Australia, New Zealand, and French Polynesia, childhood leukaemias, lymphomas, and CNS tumours represent 48–66% of all cases of cancer (fi gure 3). In Nigeria, the lymphoma group alone represented 62% (more than two-thirds of children had Burkitt’s lymphoma), whereas in Namibia, a similar number of leukaemias, lymphomas, CNS, sympathetic nervous system, renal tumours, and retinoblastoma (75% of all cases) were reported. In Alaska natives during 1969–96, liver tumours (22·6 per million per year) were the second most common tumour group.
LeukaemiaIncidence of leukaemia was reported by indigenous status in fi ve large US studies8,26,28–30 (table 3). For acute lymphoid leukaemias and acute non-lymphoid
leukaemias combined, no signifi cant diff erences were reported in incidence in American Indians, Alaska natives, and Hawaiians compared with white children from the USA.28–30 Age-standarised incidence rates for acute lymphoid leukaemia, acute myeloid leukaemia, and acute non-lymphoid leukaemias were also reported in some studies (table 3).
In the Asia–Pacifi c region, age-standardised incidence rates for leukaemia ranged from 28·3 per million per year to 47·8 per million per year (table 3). Compared with non-Maori children from New Zealand, rates of acute lymphoid leukaemias were 73% lower (age-standardised incidence rate per 100 000 children per year were 2·65 for Maori and 3·56 for non-Maori children) and rates of acute non-lymphoid leukaemias rates were 84% higher (age-standardised incidence rate per 100 000 children per year were 1·55 for Maori and 0·83 for non-Maori children) in Maori children.11 Maori children in French Polynesia (SIR 0·5)48 and Indigenous Australians (SIR 0·43)10 had signifi cantly lower rates of acute lymphoid leukaemias than did non-indigenous counterparts, but no signifi cant diff erences were recorded for acute myeloid leukaemia. In Nigeria, leukaemia ranked second among the most common cancers,22 whereas in Namibia, it ranked sixth in Wambo children.52
Tumours of the brain and CNSAge-standardised incidence rates of CNS tumours were reported for the US region, and in the Asia–Pacifi c
Indigenous group Cancer type Indigenous incidence (per million per year)
Indigenous boys incidence
Indigenous girls incidence
Comparative incidence (per million per year)
Comparative boys incidence
Comparative girls incidence
Duncan25 American Indians All cancers ·· 75·5 78·0 138·6 for non-Hispanic white children, 108·5 for Hispanic white children
·· ··
Goodman26 Hawaii Natives All cancers ·· 132 140 ·· ·· ··
Norsted27 American Indians All cancers ·· 171 75 ·· ·· ··
Lanier8 American Indians (New Mexico) All cancers 108·7 ·· ·· 153·9 ·· ··
Lanier8 Alaska natives All cancers 147·3 ·· ·· 153·9 ·· ··
Wenceslao28 Hawaii natives All cancers ·· 168·4 159·4 ·· 161·5 167·2
Li29 Alaska natives and American Indians All cancers 97·3 ·· ·· 173·2 ·· ··
Valery10 Indigenous Australians All cancers 99·5 ·· ·· ·· ·· ··
Ridgway12 New Zealand Maori Leukaemia and solid tumours 92·6 ·· ·· 89 ·· ··
Ridgway12 Pacifi c Island Polynesian Leukaemia and solid tumours 85·2 ·· ·· 89 ·· ··
Vathaire48 Maori All cancers 125 ·· ·· ·· ·· ··
Junaid22 Yoruba All cancers ·· 198·5 111·7 ·· ·· ··
Wessels52 Wambo All cancers 58·7 ·· ·· 75 ·· ··
Wessels52 Kavango All cancers 64 ·· ·· 75 ·· ··
Wessels52 Herero All cancers 47 ·· ·· 75 ·· ··
Chokunonga53 African All cancers ·· 125 96 ·· ·· ··
Bayo61 Several ethnic groups All cancers ·· 156 96 ·· ·· ··
Table 2: Age-standardised incidence rates for all cancers

www.thelancet.com/oncology Vol 15 February 2014 e96
Review
region, with some data available from Africa (table 3). The cumulative incidence rate of CNS tumours in New Zealand Maori children was 373 cases per million children during 1970–84.47
In American Indians and Indigenous Australians, incidence of CNS tumours was lower than that of their non-indigenous counterparts, whereas for Alaska natives and Maori from French Polynesia and New Zealand, incidence was similar. Compared with white children from the USA, for boys the incidence of astrocytoma in Hawaiian children was 69% lower.26 In Africa, age-standardised incidence rates were only available for Namibia and Nigeria; rates were less than nine cases per million.22,52 In indigenous children of Semnan Province, Iran, age-standardised incidence rates were 16 for boys and 12 for girls.50
RetinoblastomaAge-standarised incidence rates for retinoblastoma were available from four studies.8,22,51,52 Lanier and colleagues8 reported incidences of 6·8 per million per year in American Indians and 7·4 per million per year in Alaska natives. In Uzbekistan,51 Kazakh children had an incidence of 27 per million per year and Karakalpaks, 26 per million per year. In Namibia,52 the incidence of retinoblastoma was 7·5 per million per year, and in Nigeria,21 there was an incidence of 6·5 per million per year for boys, and 8·7 per million per year for girls. Additionally, a small US study34 reported an incidence in American Indians of one in 6550 livebirths (six cases). Incidence rates in the USA were 2·5 to three times higher than those expected in the general population.8,34 Only a few cases were reported in the Australian,10 French Polynesian,48 and New Zealand12 studies. Makata and colleagues54 reported a crude incidence rate of retinoblastoma for several ethnic groups in Kenya (0·5 per million per year in Luo and 1·2 per million per year in Luhya).
Other cancersIncidence of liver tumours in Alaska natives ranged from a peak of 30 cases per million children during 1984–88 to no cases during 1999–2008 (p<0·001).38 The age-standardised incidence rate of testicular (germ cell) tumours in American Indian and Alaska native boys in the USA was 2·8 per million per year.35 Rates of germ cell tumours (boys and girls) for American Indians was 13·5 per million per year,8 for Alaska natives 10·4 per million per year,8 and for Indigenous Australians 4·5 per million per year.10 Very few cases were reported for New Zealand Maori and Pacifi c Islander Polynesians,12 Wambo, Kavango, and Herero children in Namibia,52 and Yoruba children in Nigeria.22
Regarding Kaposi’s sarcoma, Makata and colleagues54 reported crude incidence rates for several ethnic groups in Kenya (1·5 cases in Luo and 0·4 cases in Luhya per million children per year). Crude incidence rates were also available for African children in Harare (34 cases per million children per year).53 Bayo and colleagues61
reported eight paediatric cases of Kaposi’s sarcoma in a study that reported more than 700 adult cases of cancer; neither childhood age-specifi c information nor incidence rates were reported.
In Inuit populations from Alaska, Canada, and Greenland, age-standardised incidence rates were calculated from reports of mostly adult data: penis and testis both had an incidence of 3 per million per year;39 ovarian cancer had an incidence of 5 per million per year;40 kidney (boys 6, girls 3);44 bone (boys 6, girls 5);41 connective tissue (boys 5, girls 3);41 Hodgkin’s lymphoma (boys 6, girls zero);43 non-Hodgkin lymphoma (boys 11, girls 2);43 and tumours of the salivary glands (boys 2, girls 5) and pharynx (boys 3, girls 0).42
In Luo children in Kenya, crude incidence rates of Burkitt’s lymphoma were 13 per million per year and in Luhya children, 14 per million per year; cases in these ethnic groups were over-represented compared with all cases (p=0·0003).55 In Malaysia, the age-standardised incidence rate of nasopharyngeal carcinoma in Malay children was 1 per million per year for both boys and girls,
0
10
20
30
40
50
60
70
80
90
100
110
120
130
140
150
160
170
180
190
200
210
Yoruba (Nigeria
)*
American In
dian girls (N
ew Mexico
)*25
Hawaiian girls
28
Alaska natives/A
merican In
dians (USA)
Age-
stan
dard
ised
incid
ence
rate
per
mill
ion
109
97
147
7678
156
140
168159
130
92
102
132
59
Hawaiian boys2
6
Hawaiian girls
26
American In
dian boys (New M
exico)*
25
Alaska natives*
8
Wambo (Namibia)5
2
American In
dian (New M
exico)*
8
Hawaiian boys2
8
Alaska natives/A
merican In
dians (USA)†
29
Aboriginal and Torre
s
Strait I
slands (A
ustralia
)
Maori (New Zealand)
1960s 1970s 1980s 1990s 2000s
Figure 2: Age-standardised incidence rates of all childhood cancers by indigenous group plotted alongside the timeline when cases were diagnosedMid timepoint was used and data were presented from reports in which incidence for all cancers was based on 44 cases or more. In red, age-standardised incidence rates were adjusted to the Segi World Standard Population23 (those with 95% CI were calculated from raw data). In purple, age-standardised incidence rates were adjusted to the US population. Numbers refer to study reference. *Rates adjusted to the 1970 US population. †Rates adjusted to the 2000 US population.

e97 www.thelancet.com/oncology Vol 15 February 2014
Review
and in Kadazan children, 31 per million per year for boys and 24 per million per year for girls.49
MortalityIn three studies,8,10,14 age-standardised mortality for all cancers in indigenous children was reported (fi gure 4). In the USA, the age-standardised mortality for American
Indian and Alaska native children was 20 per million children per year, signifi cantly lower than the corresponding rates for white children (30·1 per million per year) and black children (29·3 per million per year).14 Findings of an earlier report8 showed that the age-standardised mortality for Alaska native children was 28·6 per million per year versus 37·3 cases per million per year in white children, and this diff erence was not signifi cant (mortality data were not reported for American Indians). In Australia, cancer-specifi c age-standardised mortality for indigenous children was 22·9 per million per year, whereas corresponding mortality rates for non-indigenous children were similar.10 Findings from Pollack and colleagues’ study14 for American Indian and Alaska native children showed an age-standardised mortality rate of 20 per million per year from 1990–2004; new data for 1990–2009 showed an age-standardised mortality rate of 16·7 per million per year.
SurvivalFor all childhood cancers combined, 5-year survival for indigenous children in the USA, New Zealand, and Australia ranged from 60% to 64%; comparisons with
0 10 20 30 40 50 60 70 80 90 100
Yoruba (Nigeria)
Wambo (Namibia)
Maori (French Polynesia)
Maori and Pacific Islanders (NZ)
Indigenous Australians
Hawaiians (USA)
American Indians (USA)
Alaska Natives (USA)
(%)
LeukaemiasLymphoma
CNS tumoursSNS tumours*
Retinoblastoma*Renal*
Liver tumour*†Bone*
Soft tissue*Germ cell tumours*
CarcinomaOther tumours
Figure 3: Distribution of cancer types (proportion of total cases) by indigenous groupSNS=sympathetic nervous system. NZ=New Zealand. *If less than 10% of the total cases these were grouped as other tumours. †Except for Alaska natives, for all groups less than 2% of the total cases were liver cancer.
Indigenous group Cancer type Indigenous incidence (per million per year)
Indigenous boys incidence
Indigenous girls incidence
Comparative incidence (per million per year)
Comparative boys incidence
Comparative girls incidence
Lanier8 American Indians (New Mexico)
LeukaemiaALLAMLCNS
35·125·0
7·612·3
········
········
37·027·76·227·0
········
········
Lanier8 Alaska natives LeukaemiaALLAMLCNS
38·626·5
6·620·3
········
········
37·027·76·227·0
········
········
Wenceslao28 Hawaiian natives LeukaemiaALL
····
44·131·7
45·531·3
····
43·332·3
46·139·3
Goodman30 Hawaiian natives LeukaemiaALL
····
34·025·2
47·320·7
····
····
····
Lanier43 Inuit Leukaemia 42 35
Li29 Alaska natives and American Indians
LeukaemiaCNS
32·413
····
····
46·230·8
····
····
Duncan25 American Indians Leukaemia (n=11) ·· 23·8 19·8 ·· 43·8 31·8
Miller41 Inuit CNS ·· 35 30 ·· ·· ··
Vathaire48 Maori LeukaemiaALLANLLCNS
··192023
········
········
········
········
········
Dockerty11 Maori ALLANLL
26·515·5
····
····
35·68·3
····
····
Valery10 Indigenous Australians
LeukaemiaCNS
28·325·7
····
····
····
····
····
Babaei50 Semnan Province Leukaemia ·· 9 15
Wessels52 Wambo LeukaemiaCNS
6·18·9
····
····
3015
····
····
Junaid22 Yoruba LeukaemiaCNS
18·3··
··5·5
····
····
····
····
ALL=acute lymphoblastic leukaemia. AML=acute myeloid leukemia. ANLL=acute non-lymphocytic leukaemia.
Table 3: Age-standardised incidence (per million per year) for leukaemias and CNS tumours

www.thelancet.com/oncology Vol 15 February 2014 e98
Review
their non-indigenous counterparts varied (table 4). In the USA, 5-year survival in Alaska natives was signifi cantly lower than in white children,8 whereas in New Zealand, 5-year survival did not signifi cantly vary by indigenous status.20 For all childhood cancers, relative 5-year survival for Alaska natives was 60% and signifi cantly (p<0·05) lower than white children (70%). The unadjusted cause-specifi c 5-year survival probabilities by ethnic origin in New Zealand were 67% (95% CI 62–72) for non-Maori and non-Pacifi c children, 64% (52–75) for Maori children and 62% (43–82) for Pacifi c Island children; p values were not reported, but 95% CIs overlap. In Australia, overall survival in Aboriginal children did not diff er signifi cantly from their matched controls.45
The median overall survival of leukaemia in American Indian children in the USA was signifi cantly lower than in non-Hispanic and Hispanic white children.31 The median overall survival for American Indian boys was 8 months, for American Indian girls 37 months, Hispanic white boys 40 months, Hispanic white girls 72 months, non-Hispanic white boys 36 months, and for non-Hispanic white girls 140 months (p=0·0104). In a later study,32 American Indians and Alaska natives had an 80% higher risk of death from acute lymphoid leukaemias than did white children, and in the most recently reported study, American Indians and Alaska natives were twice as likely to die from acute lymphoid leukaemias than were white children.33 In New Zealand, disease-free survival for New Zealand Maori or Pacifi c Island Polynesians with acute lymphoblastic leukaemia was lower than that for non-Polynesians (68·1% for non-Polynesians, 63·6% for New Zealand Maoris, and 20% for Pacifi c Island Polynesians, combined event-free survival 42·3%, p<0·01),12 whereas in another study of acute lymphoid leukaemias, survival was not signifi cantly diff erent according to indigenous status.20 In South Africa, 5-year survival of acute lymphoid leukaemias for black children was signifi cantly lower than for white children.58,59
Survival data by indigenous status was also available for several other common childhood cancers. In the USA, 5-year survival from extracranial solid tumours for Alaska natives and American Indians was similar to that for white children,37 whereas 5-year survival of neuroblastoma was signifi cantly lower for American Indians than for white children.36 No survival diff erences were reported in neuroblastoma by indigenous status in South Africa and Namibia.60 In black South African children, 5-year survival of Wilms’ tumour56 and overall event-free survival of Hodgkin’s lymphoma57 were similar to their non-indigenous counterparts. In New Zealand, survival of solid tumours did not vary by indigenous status.12
DiscussionThis study comprehensively reports for the fi rst time the burden of cancer in indigenous children worldwide. Generally, childhood cancer is relatively rare worldwide, with age-standardised incidence rates ranging from
70 to 160 per million children aged 0–14 years per year.4,62 Although the incidence of cancer in indigenous children varies greatly between the groups studied, indigenous children in the USA, Australia, New Zealand, and French Polynesia generally have similar cancer profi les, and leukaemias, lymphomas, and CNS tumours represent a quarter of all diagnosed cases. In Africa, incidence of leukaemia in indigenous children ranged from six to 18 cases per million children, and in the USA, from 28 to 48 per million children, whereas two-thirds of the cancer cases were lymphomas in indigenous children in Nigeria.
Compared with non-indigenous children, indigenous children had similar or lower incidences (20–36% lower) of all cancers combined, although the distribution of cancer types in indigenous children was more similar to non-indigenous children within their own country than to other indigenous groups. For example, among the mainly white populations of developed economies such as the USA, Australia, and New Zealand, about a third of all childhood cancers are leukaemias, whereas in sub-Saharan Africa, the incidence is much lower.4,5,63 In high-resource settings, CNS tumours are often the second most common cancer in children, accounting for 20–25% of all childhood cancers, but arise less frequently in developing countries—eg, CNS tumours account for less than 5% of all cancers in certain African populations.4,5 We recorded similar patterns of leukaemia and CNS tumours in indigenous children and non-indigenous children within their own country.
0
10
20
30
40
50
60
1980s 1990s 2000s
Age-
stan
dard
ised
mor
talit
y ra
te p
er m
illio
n
20
29
39
24
17
Alaska natives*
8
Alaska natives/
American In
dians
(>50 states)†
29
Alaska natives/
American In
dians (USA)
Aboriginal and Torre
s
Strait I
slands (A
ustralia
)
Maori (New Zealand)
Figure 4: Age-standardised mortality of all childhood cancers by indigenous group plotted alongside the timeline when deaths were ascertained (mid timepoint was used)In red, age-standardised mortality rates were adjusted to the Segi World Standard Population23 (those with 95% CI were calculated from raw data). In purple, age-standardised mortality rates were adjusted to the US population. Numbers refer to study reference. *Rates adjusted to the 1970 US population. †Rates adjusted to the 2000 US population.

e99 www.thelancet.com/oncology Vol 15 February 2014
Review
Occurrence of childhood lymphomas is more complex. For example, Burkitt’s lymphoma arises worldwide with most cases occuring in Africa. The incidence of this lymphoma is associated with specifi c environmental factors (eg, malaria, Epstein-Barr virus, and mosquito-borne arboviruses).64–66 Incidence of Burkitt’s lymphoma in indigenous children is high in countries in the so-called lymphoma belt of Africa (eg, Nigeria22 and Kenya55), and similar to what is seen in non-indigenous populations.
Continuing along the same theme, the global variations in liver cancer incidence are indicative of the underlying burden of chronic hepatitis, cirrhosis, with diabetes emerging as a possible risk factor.67–70 Liver cancer is rare in children in Europe and North America, but more common in parts of Africa, Asia, and Melanesia. The high incidence of liver tumours reported in Alaska native
children was also recorded in the young adult Alaskan population.71 After an immunisation programme against hepatitis B was instituted in Alaska, rates of childhood liver cancer decreased markedly.38
Few data are available for childhood cancer mortality and survival by indigenous status. Supplementing existing sources with new data, mortality for all cancers ranged from 17 per million per year to 39 per million per year in the USA, Australia, and New Zealand. Comparisons between indigenous and non-indigenous children were only available for the USA and Australia; similar cancer mortality rates were reported.8,10,14 By contrast, cancer survival was generally lower for indigenous compared with non-indigenous children. This fi nding was reported in most studies of survival of leukaemia and other cancer groups including extracranial
Cancer type 5-year survival
Indigenous children Comparison group
Lanier8 2003 All cancers 60% for Alaska natives 70% for white children from the USA (p<0·05)
Rotte45 2012 All cancers About 50% for Indigenous Australian children About 75% for matched non-indigenous children (diff erence not signifi cant)
Douglas20 2007 All cancers 64% (95% CI 52–75) for Maori children; 62% (95% CI 43–82) for Pacifi c Island children
67% (95% CI 62–72) for non-Maori and non-Pacifi c children; for Maori children adjusted HR* 0·98 (95% CI 0·64–1·50); for and Pacifi c Island children adjusted HR* 1·01 (95% CI 0·53–1·89)
Douglas20 2007 Acute lymphoblastic leukaemia
62% (95% CI 35–88) for Maori children; 80% (95% CI 45–100) for Pacifi c children
71% (95% CI 62–80%) for non-Maori and non-Pacifi c children; compared with non-Maori and non-Pacifi c children, for Maori children HR† 1·09 (95% CI 0·45–2·62); for Pacifi c Island children HR† 0·99 (95% CI 0·24–4·16)
Foucar31 1991 Leukaemias About 18% for American Indian boys; about 40% for American Indian girls; median survival: 8 months for boys, 37 months for girls
Median survival: 36 months for non-Hispanic white boys, 140 months for non-Hispanic white girls (p=0·0104)
MacDougal58 1986‡
Leukaemias Acute lymphoblastic leukaemia 32% for black children; acute non-lymphoid leukaemias 10% for black children
Acute lymphoblastic leukaemia 72% for white children (p=0·0001); acute non-lymphoid leukaemias 18% for white children (p>0·05)
Hesseling59 1995 Leukaemias 17% for black children 63% for white children; 38% for coloured children; white vs black children (p<0·01)
Kadan-Lottick32 2003
Acute lymphoblastic leukaemia
54% for Alaska natives and American Indians 69% for all US children; 70% for US white children; compared with white children from the USA, for Alaska natives and American Indians adjusted HR§ 1·8 (95%CI 1·2–2·6)
Goggins33 2012 Acute lymphoblastic leukaemia
71% for Alaska natives and American Indians 83% for all US children; 87% for US white children; compared with white children from the USA, for Alaska natives and American Indians adjusted HR ¶ 2·18 (95% CI 1·46–3·26)
Ridgway12 1991 Solid tumours Disease-free survival for all solid tumours combined for Polynesians was 60·7%
Disease-free survival for all solid tumours combined for non-Polynesians was 66·0% (not signifi cant)
Ridgway12 1991 Leukaemias Disease-free survival for acute lymphoblastic leukaemia for Polynesians was 42%; 5-year survival was roughly 42%
Disease-free survival for acute lymphoblastic leukaemia for non-Polynesians was 68% (p=0·01); 5-year survival for acute lymphoblastic leukaemia was roughly 68%; for acute non-lymphoblastic leukaemia, no signifi cant survival diff erence was found
Henderson36 2011
Neuroblastoma 39% (95% CI 13–64) for Native Americans 75% for white children (95% CI 72–77); compared with white children from the USA, for Native Americans crude HR 3·00 (p=0·001) and adjusted HR‡ 2·05 (p=0·02)
Hesseling60 1999 Neuroblastoma Overall survival for black children with stage III-IV was 20%
Overall survival for white children survival with stage III–IV was 53%, and for children mixed-ethnic origin was 0% (p=0·007 for mixed vs white children; p>0·05 for black children vs white children); no survival by ethnic orign for stages I–II or all stages combined
Johnson37 2011 Extracranial solid tumours
72% for Alaska natives and American Indians 71% for white children, 71% black children, 72% Asia Pacifi c Islander; the comparison Alaska native and American Indian vs white children was not statistically signifi cant; when stratifi ed by sex, for Alaska natives and American Indians HR 1·4 (95% CI 0·91–2·13) and for girls HR 1·04 (95% CI 0·54–2·02)
Davidson56 2006 Wilms’ tumour 72·9% for black South African children 91·1% for white children; 84% for mixed-race children (p=0·13); excluding children with stage IV disease from the analysis, there was no statistically signifi cant diff erence between groups
Stefan57 2009 Hodgkin’s lymphoma
Disease-free survival for black children was 79% Disease-free survival for white children was 68%, and for coloured children 84% (p=0·35)
HR=hazard ratio.*Adjusted for sex, age at diagnosis, place of treatment, and diagnostic distribution.† Adjusted for sex and age at diagnosis.‡Adjusted for risk group. §Adjusted for age, treatment era, and sex. ¶Adjusted for age, sex, year of diagnosis, and Surveillance, Epidemiology, and End Results registry.
Table 4: Cancer survival by indigenous status (5-year survival or otherwise stated)

www.thelancet.com/oncology Vol 15 February 2014 e100
Review
solid tumours, neuroblastoma, and a US study in which survival of all cancers was reported. In a few studies, similar cancer survival by indigenous status was reported (eg, black vs white children from South Africa or coloured children had similar 5-year survival of Wilms’ tumour).57 In Australia and New Zealand, overall cancer survival was lower in indigenous compared with non-indigenous children; however, diff erences were not signifi cant.20,45
Navigation through the health-care system for cancer care can be a diffi cult and traumatic experience, especially in indigenous people who might not always be familiar or understand modern, evidence-based health-care systems, which are often very diff erent from traditional indigenous medicines.72,73 Cultural and cross-cultural issues might play a part in treatment compliance.74,75 Although treatment refusal is often infrequent in paediatric oncology,76 published reports have treatment adherence ranging from 41% to 98%.77,78 In particular, treatment abandonment is a major cause of treatment failure in low-income countries.79,80 As far as we are aware, information about treatment refusal, treatment abandonment, and compliance in indigenous children diagnosed with cancer is not available.
Some cancer registries (eg, in Australia, New Zealand, and the USA) have complete population coverage for incidence and careful follow-up of mortality, whereas in other, lower-resource areas, availability tends to be more restricted and of variable quality. Such diversity in the availability, completeness, and validity of the data from diff erent sources over time means that the comparison of rates should be interpreted with caution in view of these circumstances and the prospects of varying registry practices, including potential diff erences in disease coding and classifi cation. However, we did attempt to ensure valid comparative analyses in those countries where additional data were acquired by adjusting rates with the world standard population,23 whereas fi ndings of a sensitivity analysis showed a minimum bias was induced on comparison of age-adjusted rates based on use of diff erent standard populations in diff erent studies (appendix). Lastly, random variation is inherent in these analyses because some estimates were based on small numbers of cases.
We found few reports outlining the cancer incidence, mortality, or survival in indigenous children in countries where large indigenous groups reside such as in South America or the circumpolar region (eg, in the Saami and Nenets populations). In one study81 cancer was reported in indigenous children in Canada, although not separately for First Nations, Inuit, and Metis children. Generally, childhood cancer has been an under-recognised issue in indigenous populations worldwide. In low-income and medium-income countries, the implementation of cancer registration is diffi cult in view of insuffi cient health-care services and competing demands for fi nite health resources.82 However, where population-based cancer registration is available, no routine collection of
indigenous status in health data exists (eg, Inuit in Greenland or Denmark)81 and collection by registries is hampered by a lack of accurate and complete ethnic origin data, essential for measurement and monitoring of ethnic disparities. In many Latin American countries, where 10% of the population is indigenous,83 data for cancer in indigenous people are especially scarce.
Data from a systematic review84 of cancer patterns and causes in indigenous people in Latin American countries suggested a very limited availability of cancer registry data; of 26 countries included, three recorded indigenous status (Brazil, Guatemala, and Guyana). Data for indigenous children were not available. Furthermore, indigenous people are assigned based on their self-reported knowledge of an indigenous language85 or by phenotype (skin colour and physical characteristics, such as Brazil).86 More valid ways to register indigenous status need to be developed. As highlighted by Goss and colleagues,87 Latin American countries are poorly equipped to deal with the increasing cancer incidence and disproportionately high mortality.87 In many areas in South America, access to cancer care is impaired by inadequate health-system infrastructure. An important barrier to cancer care aff ecting indigenous people in this region is the fact that people often reside in rural or remote areas with poor access to health services (eg, no cancer screening or long waits, poor diagnostic testing, and long waits for follow-up care and treatment).
An important fi rst step towards improvement of cancer detection and care in the indigenous populations is to include indigenous status in cancer registry data. In population-based cancer registries in which data is collected for indigenous status, there should be active encouragement to make use and publish relevant results. In this respect, the International Agency for Research on Cancer (IARC) and the International Association of Cancer Registries (IACR) have a role in the promotion and facilitation of such activities. Indeed, the IARC has done extensive studies of childhood cancer incidence worldwide,88 and its publications provide a comprehensive source of information about childhood cancer epi-demiology. However, despite receiving information from many population-based tumour registries, most data held at IARC do not contain information about indigenous status. The only exceptions are the USA and New Zealand. Hence, we chose to do a systematic review of published literature rather than using data from the IARC databases.
A limitation of this study is the many cases for which indigenous status was not specifi ed or incorrectly classifi ed.89,90 Although we aimed to assess all available evidence on the burden of cancer in indigenous children, we might have missed some reports (eg, reports of specifi c indigenous groups not specifi ed as such in the Medical Subject Headings terms, title, or abstract) whereas others might have included small proportions of non-indigenous children or children from other indigenous groups in their estimates—eg, Junaid and colleagues’22 report of

e101 www.thelancet.com/oncology Vol 15 February 2014
Review
cancer in Yoruba children in Nigeria. We also acknowledge that certain populations might conceivably have been considered for inclusion in this review (eg, Taiwanese aborigines and Andamaman Islanders in India), but lack of evidence or contentious defi nitions of indigeneity rendered this impractical, as would the requirement to search through the names of more than 5000 indigenous population groups for relevant literature (eg, IWGIA).
Our review included diverse types of indigenous groups. In high-income countries where indigenous groups are a minority group (eg, Maori people in New Zealand), diff erences in cancer incidence and outcome might be related to access to health care, poverty, sociocultural factors, or genetic factors. In low-income and middle-income countries, these populations often form a large proportion of the general population (eg, indigenous population of Semnan Province, Iran) or represent the majority (eg, black people in South Africa). Diff erences in incidence and outcome for those might be related to the aforementioned factors; however, these eff ects can mask large disparities in access to cancer diagnosis (under-diagnosis, misdiagnosis, or both) and under-reporting.91 The sources of errors in estimation of childhood cancer in low-income countries include inaccurate population estimates, errors in case ascertainment, and incorrect initial diagnoses.91 Additionally, diff erences in reported versus true rates of childhood cancer will vary by cancer type. Most solid tumours usually present with a visible mass, and are more likely to be diagnosed and recorded. Under-reporting of haematological cancers (eg, leukaemias) might happen because of health infra-structure defi cits coupled with a set of signs and symptoms that resemble those of infection, and early death might precede cancer diagnosis.92
Studies of childhood cancer in diff erent regions and ethnic groups can provide clues to causes, identify biological diff erences,91 and suggest genetic or environmental exposures that aff ect cancer risk or outcomes. The excess of Burkitt’s lymphoma64–66 and Kaposi’s sarcoma93 in sub-Saharan Africa are examples of associations with specifi c environmental factors; malaria, Epstein-Barr virus, and mosquito-borne arboviruses in Burkitt’s lymphoma, and the HIV epidemic in Kaposi’s sarcoma. The decrease in incidence of Burkitt’s lymphoma and concomitant increase in acute lymphoblastic leukaemia in the Gaza strip coincided with a period of rapid socioeconomic development, linking the occurrence of these cancers with socioeconomic factors.94 Furthermore, identifi cation of the high incidence of cancer types in a particular region (eg, retinoblastoma in Honduras)95,96 or a population group (eg, liver tumours in Alaska natives) has helped to improve public health through identifi cation, and subsequent actions in prevention, early diagnosis, and treatment.
These data highlight the paucity of information available about the burden of childhood cancers in indigenous populations. Although the lower or similar
overall incidence burden from cancer recorded in indigenous children (compared with their non-indigenous counterparts) in countries with available data is encouraging, the results cover a small proportion of the indigenous children being diagnosed with cancer worldwide. We advocate the need for childhood cancer data by indigenous status in countries where population-based cancer registration is available. The IARC, IACR, and local cancer agencies play an important part in advocating for such data to be available. We also support the drive towards improved and increased coverage of cancer registration in low-income and middle-income countries.82 In view of the historic lack of data for cancer in indigenous children, an informative alternate approach has been to assess the patterns of cancer in population groups with a high proportion of indigenous people. Before reliable information about indigenous status in Queensland, Australia, were available, Coory and colleagues97 assessed cancer incidence in easily identifi able rural and remote communities in which most of the population was indigenous.
Data for cancer incidence, mortality, and survival can uncover the true extent of disparities in the cancer burden by indigenous status at the global, regional, and country level. Such indicators need to be routinely measured so that programmes of cancer control can be used to plan and implement targeted interventions where they are needed most. Especially with regards to disparities in survival, diff erences in treatment have been reported as contributing factors for the poor cancer prognosis in indigenous adults.98 Joint investigations of treatment, compliance, and patterns of care might help elucidate the specifi c factors that contribute to the survival diff erences, thus enabling modifi cations in tertiary prevention aimed at the improvement of outcomes in indigenous children diagnosed with cancer.
ContributorsPCV and JM independently reviewed all manuscripts, and SPM
adjudicated disagreements. SPM assisted with data acquisition. PCV did
the data analysis and takes responsibility for the integrity and the
accuracy of the data. FB contributed to the study design and
interpretation of the data. PCV drafted the report and all authors
contributed to its editing and approved its fi nal version.
Confl icts of interestWe declare that we have no confl icts of interest.
AcknowledgmentsPCV was supported by an Australian Research Council Future Fellowship
(#FT100100511). SPM was supported by an International Agency for
Research on Cancer-Cancer Council Australia Postdoctoral Fellowship.
References 1 United Nations. State of the world’s indigenous peoples.
New York: Department of Economic and Social Aff airs, United Nations, 2009.
2 Cobo JM. Study of the problem of discrimination against indigenous populations. Final report submitted by the Special Rapporteur, Mr José Martínez Cobo. Vienna, Austria: United Nations Economic and Social Council, 1981.
3 Stiller CA. International patterns of cancer incidence in adolescents. Cancer Treat Rev 2007; 33: 631–45.
4 Stiller CA, Parkin DM. Geographic and ethnic variations in the incidence of childhood cancer. Br Med Bull 1996; 52: 682–703.

www.thelancet.com/oncology Vol 15 February 2014 e102
Review
5 Parkin DM, Stiller CA, Draper GJ, Bieber CA. The international incidence of childhood cancer. Int J Cancer 1988; 42: 511–20.
6 Stiller CA, Marcos-Gragera R, Ardanaz E, et al. Geographical patterns of childhood cancer incidence in Europe, 1988–1997. Report from the Automated Childhood Cancer Information System project. Eur J Cancer 2006; 42: 1952–60.
7 Breslow N, Olshan A, Beckwith JB, Moksness J, Feigl P, Green D. Ethnic variation in the incidence, diagnosis, prognosis, and follow-up of children with Wilms’ tumor. J Natl Cancer Inst 1994; 86: 49–51.
8 Lanier AP, Holck P, Ehrsam Day G, Key C. Childhood cancer among Alaska Natives. Pediatrics 2003; 112: e396.
9 McKinney PA, Feltbower RG, Parslow RC, Lewis IJ, Glaser AW, Kinsey SE. Patterns of childhood cancer by ethnic group in Bradford, UK 1974–1997. Eur J Cancer 2003; 39: 92–97.
10 Valery PC, Youlden DR, Baade PD, Ward LJ, Green AC, Aitken JF. Cancer incidence and mortality in Indigenous Australian children, 1997–2008. Pediatr Blood Cancer 2013; 60: 156–58.
11 Dockerty JD, Cox B, Cockburn MG. Childhood leukaemias in New Zealand: time trends and ethnic diff erences. Br J Cancer 1996; 73: 1141–47.
12 Ridgway D, Skeen JE, Mauger DC, Becroft DM. Childhood cancer among the Polynesian population. Cancer 1991; 68: 451–54.
13 Day GE, Lanier AP. Alaska native mortality, 1979–1998. Public Health Rep 2003; 118: 518–30.
14 Pollack L, Stewart S, Thompson T. Trends in childhood cancer mortality: United States, 1990–2004. MMWR Morb Mortal Wkly Rep 2007; 56: 1257–61.
15 Ministry of Health. Our Children’s Health: key fi ndings on the health of New Zealand children. Wellington, New Zealand: Ministry of Health, 1998.
16 McKinney PA, Feltbower RG, Parslow RC, et al. Survival from childhood cancer in Yorkshire, UK: eff ect of ethnicity and socio-economic status. Eur J Cancer 1999; 35: 1816–23.
17 Stiller CA, Bunch KJ, Lewis IJ. Ethnic group and survival from childhood cancer: report from the UK Children’s Cancer Study Group. Br J Cancer 2000; 82: 1339–43.
18 Children’s Oncology Group, Aplenc R, Alonzo TA, et al. Ethnicity and survival in childhood acute myeloid leukemia: a report from the Children’s Oncology Group. Blood 2006; 108: 74–80.
19 Linabery AM, Ross JA. Childhood and adolescent cancer survival in the US by race and ethnicity for the diagnostic period 1975–1999. Cancer 2008; 113: 2575–96.
20 Douglas NM, Dockerty JD. Survival by ethnicity for children diagnosed with cancer in New Zealand during 1990-1993. J Paediatr Child Health 2007; 43: 173–77.
21 Australian Bureau of Statistics. Experimental estimates of aboriginal and torres strait islander Australians, June 2006. Catalog no. 3238.0 2008. Cranberra, Australia: Commonwealth of Australia, 2006.
22 Junaid TA, Babalola BO. Ibadan Cancer Registry, 1960–1984. International incidence of childhood cancer. IARC scientifi c publication No 87. Lyon, France: International Incidence of Childhood Cancer, 1988.
23 Segi M. Cancer mortality for selected sites in 24 countries (1950–57). Sendai, Japan: Tohoku University of Medicine, 1960.
24 Boyle P, Parkin D. Statistical Methods for registries. In: Jensen OM, ed. Cancer registration: principles and methods. Lyon, France: International Agency for Research on Cancer, 1991. 126–58.
25 Duncan MH, Wiggins CL, Samet JM, Key CR. Childhood cancer epidemiology in New Mexico’s American Indians, Hispanic whites, and non-Hispanic whites, 1970–82. J Natl Cancer Inst 1986; 76: 1013–18.
26 Goodman MT, Yoshizawa CN, Kolonel LN. Ethnic patterns of childhood cancer in Hawaii between 1960 and 1984. Cancer 1989; 64: 1758–63.
27 Norsted TL, White E. Cancer incidence among native Americans of western Washington. Int J Epidemiol 1989; 18: 22–27.
28 Wenceslao S, Gotay CC, Cheung LW, White K. Patterns of childhood cancer in Hawai’i between 1975 and 2000. Hawaii Med J 2006; 65: 221–25.
29 Li J, Thompson TD, Miller JW, Pollack LA, Stewart SL. Cancer incidence among children and adolescents in the United States, 2001–2003. Pediatrics 2008; 121: e1470–77.
30 Goodman MT, Yoshizawa CN, Kolonel LN. Incidence trends and ethnic patterns for childhood leukaemia in Hawaii: 1960–1984. Br J Cancer 1989; 60: 93–97.
31 Foucar K, Duncan MH, Stidley CA, Wiggins CL, Hunt WC, Key CR. Survival of children and adolescents with acute lymphoid leukemia. A study of American Indians and Hispanic and non-Hispanic whites treated in New Mexico (1969 to 1986). Cancer 1991; 67: 2125–30.
32 Kadan-Lottick NS, Ness KK, Bhatia S, Gurney JG. Survival variability by race and ethnicity in childhood acute lymphoblastic leukemia. JAMA 2003; 290: 2008–14.
33 Goggins WB, Lo FF. Racial and ethnic disparities in survival of US children with acute lymphoblastic leukemia: evidence from the SEER database 1988–2008. Cancer Causes Control 2012; 23: 737–43.
34 Berkow RL, Fleshman JK. Retinoblastoma in Navajo Indian children. Am J Dis Child 1983; 137: 137–38.
35 Walsh TJ, Davies BJ, Croughan MS, Carroll PR, Turek PJ. Racial diff erences among boys with testicular germ cell tumors in the United States. J Urol 2008; 179: 1961–65.
36 Henderson TO, Bhatia S, Pinto N, et al. Racial and ethnic disparities in risk and survival in children with neuroblastoma: a Children’s Oncology Group study. J Clin Oncol 2011; 29: 76–82.
37 Johnson KA, Aplenc R, Bagatell R. Survival by race among children with extracranial solid tumors in the United States between 1985 and 2005. Pediatr Blood Cancer 2011; 56: 425–31.
38 McMahon BJ, Bulkow LR, Singleton RJ, et al. Elimination of hepatocellular carcinoma and acute hepatitis B in children 25 years after a hepatitis B newborn and catch-up immunization program. Hepatology 2011; 54: 801–07.
39 Prener A, Storm HH, Nielsen NH. Cancer of the male genital tract in Circumpolar Inuit. Acta Oncol 1996; 35: 589–93.
40 Kjaer SK, Nielsen NH. Cancer of the female genital tract in Circumpolar Inuit. Acta Oncol 1996; 35: 581–87.
41 Miller AB, Gaudette LA. Cancers of skin, bone, connective tissues, brain, eye, thyroid and other specifi ed and unspecifi ed sites in Inuit. Acta Oncol 1996; 35: 607–16.
42 Lanier AP, Alberts SR. Cancers of the buccal cavity and pharynx in Circumpolar Inuit. Acta Oncol 1996; 35: 545–52.
43 Lanier AP, Alberts SR. Malignant neoplasms of the lymphatic and haematopoietic system in Circumpolar Inuit. Acta Oncol 1996; 35: 601–06.
44 Lanier AP, Alberts SR. Kidney and bladder cancer in Inuit 1969–1988. Acta Oncol 1996; 35: 595–99.
45 Rotte L, Hansford J, Kirby M, et al. Cancer in Australian Aboriginal children: Room for improvement. J Paediatr Child Health 2013; 49: 27–32.
46 Monteith SJ, Heppner PA, Woodfi eld MJ, Law AJJ. Paediatric central nervous system tumours in a New Zealand population: a 10-year experience of epidemiology, management strategies and outcomes. J Clin Neurosci 2006; 13: 722–29.
47 Filippini G, Artuso A. International incidence of central nervous system tumors in children. Ital J Neurol Sci 1992; 13: 395–400.
48 Vathaire CC, De Vathaire F, Vu BL, et al. Childhood malignancies in French Polynesia during the 1985–1995 period. Trop Med Int Health 2004; 9: 1005–11.
49 Yadav M, Tan MK, Singh P, Dharmalingam SK. Nasopharyngeal carcinoma in Malaysians under the age of 20 years. Clin Oncol 1984; 10: 353–61.
50 Babaei M, Mousavi S, Malek M, et al. Cancer occurrence in Semnan Province, Iran: results of a population-based cancer registry. Asian Pac J Cancer Prev 2005; 6: 159–64.
51 Mouratova T. Retinoblastoma in Uzbekistan. Bull Soc Belge Ophtalmol 2003; 289: 63–69.
52 Wessels G, Hesseling PB. Unusual distribution of childhood cancer in Namibia. Pediatr Hematol Oncol 1996; 13: 9–20.
53 Chokunonga E, Levy LM, Bassett MT, Mauchaza BG, Thomas DB, Parkin DM. Cancer incidence in the African population of Harare, Zimbabwe: second results from the cancer registry 1993–1995. Int J Cancer 2000; 85: 54–59.
54 Makata AM, Toriyama K, Kamidigo NO, Eto H, Itakura H. The pattern of pediatric solid malignant tumors in western Kenya, east Africa, 1979–1994: an analysis based on histopathologic study. Am J Trop Med Hyg 1996; 54: 343–47.

e103 www.thelancet.com/oncology Vol 15 February 2014
Review
55 Mwanda OW, Rochford R, Moormann AM, Macneil A, Whalen C, Wilson ML. Burkitt’s lymphoma in Kenya: geographical, age, gender and ethnic distribution. East Afr Med J 2004; 81 (suppl 8): 68–77.
56 Davidson A, Hartley P, Desai F, Daubenton J, Rode H, Millar A. Wilms tumour experience in a South African centre. Pediatr Blood Cancer 2006; 46: 465–71.
57 Stefan DC, Stones D, Dippenaar A, Kidd M. Ethnicity and characteristics of Hodgkin lymphoma in children. Pediatr Blood Cancer 2009; 52: 182–85.
58 MacDougall LG. Acute childhood leukaemia in Johannesburg. Leuk Res 1985; 9: 765–67.
59 Hesseling PB, Wessels G, van Riet FA. The Tygerberg Hospital Children’s Tumour Registry 1983–1993. Eur J Cancer 1995; 31: 1471–75.
60 Hesseling PB, Ankone K, Wessels G, Schneider JW, Du Plessis L, Moore S. Neuroblastoma in southern Africa: epidemiological features, prognostic factors and outcome. Ann Trop Paediatr 1999; 19: 357–63.
61 Bayo S, Parkin DM, Koumare AK, et al. Cancer in Mali, 1987–1988. Int J Cancer 1990; 45: 679–84.
62 Stiller CA. Epidemiology and genetics of childhood cancer. Oncogene 2004; 23: 6429–44.
63 Baade PD, Youlden DR, Valery PC, et al. Trends in incidence of childhood cancer in Australia, 1983–2006. Br J Cancer 2010; 102: 620–26.
64 van den Bosch CA. Is endemic Burkitt’s lymphoma an alliance between three infections and a tumour promoter? Lancet Oncol 2004; 5: 738–46.
65 Sitas F, Pacella-Norman R, Carrara H, et al. The spectrum of HIV-1 related cancers in South Africa. Int J Cancer 2000; 88: 489–92.
66 Rickinson AB, Gregory CD. Burkitt’s lymphoma. Trans R Soc Trop Med Hyg 1988; 82: 657–59.
67 Lavanchy D. The global burden of hepatitis C. Liver Int 2009; 29 (suppl 1): 74–81.
68 Parkin DM, Bray F, Ferlay J, Pisani P. Estimating the world cancer burden: Globocan 2000. Int J Cancer 2001; 94: 153–56.
69 El-Serag HB, Hampel H, Javadi F. The association between diabetes and hepatocellular carcinoma: a systematic review of epidemiologic evidence. Clin Gastroenterol Hepatol 2006; 4: 369–80.
70 Richardson LC, Pollack LA. Therapy insight: Infl uence of type 2 diabetes on the development, treatment and outcomes of cancer. Nat Clin Pract Oncol 2005; 2: 48–53.
71 Weir HK, Jim MA, Marrett LD, Fairley T. Cancer in American Indian and Alaska Native young adults (ages 20–44 years): US, 1999–2004. Cancer 2008; 113 (suppl 5): 1153–67.
72 Shahid S, Thompson SC. An overview of cancer and beliefs about the disease in Indigenous people of Australia, Canada, New Zealand and the US. Aust N Z J Public Health 2009; 33: 109–18.
73 Montenegro RA, Stephens C. Indigenous health in Latin America and the Caribbean. Lancet 2006; 367: 1859–69.
74 Friedrich P, Ortiz R, Strait K, et al. Pediatric sarcoma in Central America: outcomes, challenges, and plans for improvement. Cancer 2013; 119: 871–79.
75 Luna-Fineman S, Barnoya M, Bonilla M, Fu L, Baez F, Rodriguez-Galindo C. Retinoblastoma in Central America: report from the Central American Association of Pediatric Hematology Oncology (AHOPCA). Pediatr Blood Cancer 2012; 58: 545–50.
76 Alessandri AJ. Parents know best: or do they? Treatment refusals in paediatric oncology. J Paediatr Child Health 2011; 47: 628–31.
77 Landier W. Age span challenges: adherence in pediatric oncology. Semin Oncol Nurs 2011; 27: 142–53.
78 Mancini J, Simeoni MC, Parola N, et al. Adherence to leukemia maintenance therapy: a comparative study among children, adolescents, and adults. Pediatr Hematol Oncol 2012; 29: 428–39.
79 Israels T, Ribeiro RC, Molyneux EM. Strategies to improve care for children with cancer in Sub-Saharan Africa. Eur J Cancer 2010; 46: 1960–66.
80 Mostert S, Arora RS, Arreola M, et al. Abandonment of treatment for childhood cancer: position statement of a SIOP PODC Working Group. Lancet Oncol 2011; 12: 719–20.
81 Kelly J, Lanier A, Santos M, et al, for the Circumpolar Inuit Cancer Review Working Group. Cancer among the circumpolar Inuit, 1989–2003. I. Background and methods. Int J Circumpolar Health 2008; 67: 396–407.
82 Valsecchi MG, Steliarova-Foucher E. Cancer registration in developing countries: luxury or necessity? Lancet Oncol 2008; 9: 159–67.
83 Hall G, Patrinos HA. Indigenous people, poverty, and human development in Latin America 1994–2004. New York: The World Bank, 2006: 221–40.
84 Moore SP, Forman D, Pineros M, Fernandez SM, Santos MO, Bray F. Cancer in indigenous people in Latin America and the Caribbean: a review. Cancer Med 2013; published online Dec 3. DOI:10.1002/cam4.134.
85 San Sebastian M, Hurtig AK. Cancer among indigenous people in the Amazon Basin of Ecuador, 1985-2000. Rev Panam Salud Publica 2004; 16: 328–33.
86 Okediji TO. The dynamics of race, ethnicity and economic development: the Brazilian experience. J Socio Econ 2004; 33: 201–15.
87 Goss PE, Lee BL, Badovinac-Crnjevic T, et al. Planning cancer control in Latin America and the Caribbean. Lancet Oncol 2013; 14: 391–436.
88 Steliarova-Foucher E, Stiller C, Lacour B, Kaatsch P. International Classifi cation of Childhood Cancer, third edition. Cancer 2005; 103: 1457–67.
89 Thompson SC, Woods JA, Katzenellenbogen JM. The quality of indigenous identifi cation in administrative health data in Australia: insights from studies using data linkage. BMC Med Inform Decis Mak 2012; 12: 133.
90 Shaw C, Atkinson J, Blakely T. (Mis)classifi cation of ethnicity on the New Zealand Cancer Registry: 1981–2004. N Z Med J 2009; 122: 10–22.
91 Howard SC, Metzger ML, Wilimas JA, et al. Childhood cancer epidemiology in low-income countries. Cancer 2008; 112: 461–72.
92 Cheng S, Pole JD, Sung L. Early deaths in pediatric acute leukemia: a population-based study. Leuk Lymphoma 2013; published online Nov 19. DOI:10.3109/10428194.2013.850685.
93 Amir H, Kaaya EE, Manji KP, Kwesigabo G, Biberfeld P. Kaposi’s sarcoma before and during a human immunodefi ciency virus epidemic in Tanzanian children. Pediatr Infect Dis J 2001; 20: 518–21.
94 Ramot B, Magrath I. Hypothesis: the environment is a major determinant of the immunological sub-type of lymphoma and acute lymphoblastic leukaemia in children. Br J Haematol 1982; 50: 183–89.
95 Rodriguez-Galindo C, Wilson MW, Chantada G, et al. Retinoblastoma: one world, one vision. Pediatrics 2008; 122: e763–70.
96 Leander C, Fu LC, Pena A, et al. Impact of an education program on late diagnosis of retinoblastoma in Honduras. Pediatr Blood Cancer 2007; 49: 817–19.
97 Coory M, Thompson A, Ganguly I. Cancer among people living in rural and remote Indigenous communities in Queensland. Med J Aust 2000; 173: 301–04.
98 Valery PC, Coory M, Stirling J, Green AC. Cancer diagnosis, treatment, and survival in Indigenous and non-Indigenous Australians: a matched cohort study. Lancet 2006; 367: 1842–48.