Embed Size (px)
Citation preview

International Randomized Trials in Orthopaedic Oncology:
Joining Forces and Shifting the Paradigm
Michelle Ghert, MD, FRCSC
Center for Evidence-Based Orthopaedics
McMaster University


Disclosure
• Committee Chair: Orthopaedic Research Society• Committee Member: Musculoskeletal Tumor Society• Grand Funding: OREF, MSTS, PSI, CCSRI, MSA• Private Funding: Manherz Family Donation
Overview
• Learning Process• Take Home Points:
Trials require: 1. The right question
2. Centralized infrastructure
3. Collaborative network

Where the Process Started

Strong Pull to 'The Dark Side’

First ever Department of Clinical Epidemiology Chairman: Dr. David Sackett
Dr. David SackettM.S. from Harvard Epidemiology
Mentor
Dr. Gordon GuyattCoined the term “Evidence-Based Medicine”
Mentor
Dr. Mohit BhandariUnparalleled transformation in orthopaedic researchProspective international randomized controlled trials
Mentor
Clinical Epidemiology: Absorbed through osmosis

“Elephant in Paris” moment
CTOS 2010

Will it work?
• Trials require: 1. The right question
2. Centralized infrastructure
3. Collaborative network

Challenges to Prospective Research

Current Evidence in Orthopaedic Oncology
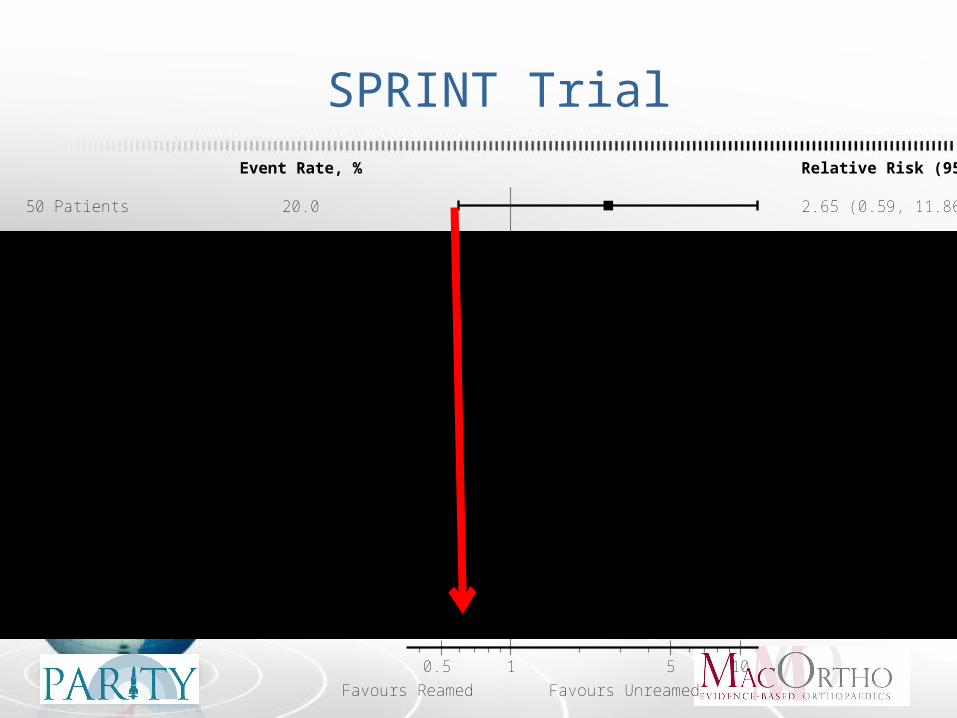
SPRINT Trial
Favours Reamed Favours Unreamed
1 5 100.5
Event Rate, % Relative Risk (95% CI)
50 Patients 20.0 2.65 (0.59, 11.86)
100 Patients 24.3 2.14 (0.84, 5.43)
200 Patients 18.1 1.08 (0.53, 2.20)
300 Patients 18.1 1.04 (0.58, 1.85)
400 Patients 18.4 1.07 (0.65, 1.76)
500 Patients 17.2 0.92 (0.58, 1.47)
600 Patients 15.8 0.81 (0.51, 1.26)
700 Patients 15.3 0.73 (0.48, 1.12)
800 Patients 14.7 0.65 (0.43, 0.99)
900 Patients 14.7 0.57 (0.40, 0.87)
1000 Patients 14.1 0.63 (0.43, 0.91)
1100 Patients 14.0 0.66 (0.46, 0.94)
1226 Patients 13.7 0.65 (0.46, 0.93)
Favours Reamed Favours Unreamed
1 5 100.5
Event Rate, % Relative Risk (95% CI)
50 Patients 20.0 2.65 (0.59, 11.86)
100 Patients 24.3 2.14 (0.84, 5.43)
200 Patients 18.1 1.08 (0.53, 2.20)
300 Patients 18.1 1.04 (0.58, 1.85)
400 Patients 18.4 1.07 (0.65, 1.76)
500 Patients 17.2 0.92 (0.58, 1.47)
600 Patients 15.8 0.81 (0.51, 1.26)
700 Patients 15.3 0.73 (0.48, 1.12)
800 Patients 14.7 0.65 (0.43, 0.99)
900 Patients 14.7 0.57 (0.40, 0.87)
1000 Patients 14.1 0.63 (0.43, 0.91)
1100 Patients 14.0 0.66 (0.46, 0.94)
1226 Patients 13.7 0.65 (0.46, 0.93)
Favours Reamed Favours Unreamed
1 5 100.5
Event Rate, % Relative Risk (95% CI)
50 Patients 20.0 2.65 (0.59, 11.86)
100 Patients 24.3 2.14 (0.84, 5.43)
200 Patients 18.1 1.08 (0.53, 2.20)
300 Patients 18.1 1.04 (0.58, 1.85)
400 Patients 18.4 1.07 (0.65, 1.76)
500 Patients 17.2 0.92 (0.58, 1.47)
600 Patients 15.8 0.81 (0.51, 1.26)
700 Patients 15.3 0.73 (0.48, 1.12)
800 Patients 14.7 0.65 (0.43, 0.99)
900 Patients 14.7 0.57 (0.40, 0.87)
1000 Patients 14.1 0.63 (0.43, 0.91)
1100 Patients 14.0 0.66 (0.46, 0.94)
1226 Patients 13.7 0.65 (0.46, 0.93)
Favours Reamed Favours Unreamed
1 5 100.5
Event Rate, % Relative Risk (95% CI)
50 Patients 20.0 2.65 (0.59, 11.86)
100 Patients 24.3 2.14 (0.84, 5.43)
200 Patients 18.1 1.08 (0.53, 2.20)
300 Patients 18.1 1.04 (0.58, 1.85)
400 Patients 18.4 1.07 (0.65, 1.76)
500 Patients 17.2 0.92 (0.58, 1.47)
600 Patients 15.8 0.81 (0.51, 1.26)
700 Patients 15.3 0.73 (0.48, 1.12)
800 Patients 14.7 0.65 (0.43, 0.99)
900 Patients 14.7 0.57 (0.40, 0.87)
1000 Patients 14.1 0.63 (0.43, 0.91)
1100 Patients 14.0 0.66 (0.46, 0.94)
1226 Patients 13.7 0.65 (0.46, 0.93)
Favours Reamed Favours Unreamed
1 5 100.5
Event Rate, % Relative Risk (95% CI)
50 Patients 20.0 2.65 (0.59, 11.86)
100 Patients 24.3 2.14 (0.84, 5.43)
200 Patients 18.1 1.08 (0.53, 2.20)
300 Patients 18.1 1.04 (0.58, 1.85)
400 Patients 18.4 1.07 (0.65, 1.76)
500 Patients 17.2 0.92 (0.58, 1.47)
600 Patients 15.8 0.81 (0.51, 1.26)
700 Patients 15.3 0.73 (0.48, 1.12)
800 Patients 14.7 0.65 (0.43, 0.99)
900 Patients 14.7 0.57 (0.40, 0.87)
1000 Patients 14.1 0.63 (0.43, 0.91)
1100 Patients 14.0 0.66 (0.46, 0.94)
1226 Patients 13.7 0.65 (0.46, 0.93)
Favours Reamed Favours Unreamed
1 5 100.5
Event Rate, % Relative Risk (95% CI)
50 Patients 20.0 2.65 (0.59, 11.86)
100 Patients 24.3 2.14 (0.84, 5.43)
200 Patients 18.1 1.08 (0.53, 2.20)
300 Patients 18.1 1.04 (0.58, 1.85)
400 Patients 18.4 1.07 (0.65, 1.76)
500 Patients 17.2 0.92 (0.58, 1.47)
600 Patients 15.8 0.81 (0.51, 1.26)
700 Patients 15.3 0.73 (0.48, 1.12)
800 Patients 14.7 0.65 (0.43, 0.99)
900 Patients 14.7 0.57 (0.40, 0.87)
1000 Patients 14.1 0.63 (0.43, 0.91)
1100 Patients 14.0 0.66 (0.46, 0.94)
1226 Patients 13.7 0.65 (0.46, 0.93)
Favours Reamed Favours Unreamed
1 5 100.5
Event Rate, % Relative Risk (95% CI)
50 Patients 20.0 2.65 (0.59, 11.86)
100 Patients 24.3 2.14 (0.84, 5.43)
200 Patients 18.1 1.08 (0.53, 2.20)
300 Patients 18.1 1.04 (0.58, 1.85)
400 Patients 18.4 1.07 (0.65, 1.76)
500 Patients 17.2 0.92 (0.58, 1.47)
600 Patients 15.8 0.81 (0.51, 1.26)
700 Patients 15.3 0.73 (0.48, 1.12)
800 Patients 14.7 0.65 (0.43, 0.99)
900 Patients 14.7 0.57 (0.40, 0.87)
1000 Patients 14.1 0.63 (0.43, 0.91)
1100 Patients 14.0 0.66 (0.46, 0.94)
1226 Patients 13.7 0.65 (0.46, 0.93)
Favours Reamed Favours Unreamed
1 5 100.5
Event Rate, % Relative Risk (95% CI)
50 Patients 20.0 2.65 (0.59, 11.86)
100 Patients 24.3 2.14 (0.84, 5.43)
200 Patients 18.1 1.08 (0.53, 2.20)
300 Patients 18.1 1.04 (0.58, 1.85)
400 Patients 18.4 1.07 (0.65, 1.76)
500 Patients 17.2 0.92 (0.58, 1.47)
600 Patients 15.8 0.81 (0.51, 1.26)
700 Patients 15.3 0.73 (0.48, 1.12)
800 Patients 14.7 0.65 (0.43, 0.99)
900 Patients 14.7 0.57 (0.40, 0.87)
1000 Patients 14.1 0.63 (0.43, 0.91)
1100 Patients 14.0 0.66 (0.46, 0.94)
1226 Patients 13.7 0.65 (0.46, 0.93)
Favours Reamed Favours Unreamed
1 5 100.5
Event Rate, % Relative Risk (95% CI)
50 Patients 20.0 2.65 (0.59, 11.86)
100 Patients 24.3 2.14 (0.84, 5.43)
200 Patients 18.1 1.08 (0.53, 2.20)
300 Patients 18.1 1.04 (0.58, 1.85)
400 Patients 18.4 1.07 (0.65, 1.76)
500 Patients 17.2 0.92 (0.58, 1.47)
600 Patients 15.8 0.81 (0.51, 1.26)
700 Patients 15.3 0.73 (0.48, 1.12)
800 Patients 14.7 0.65 (0.43, 0.99)
900 Patients 14.7 0.57 (0.40, 0.87)
1000 Patients 14.1 0.63 (0.43, 0.91)
1100 Patients 14.0 0.66 (0.46, 0.94)
1226 Patients 13.7 0.65 (0.46, 0.93)
Favours Reamed Favours Unreamed
1 5 100.5
Event Rate, % Relative Risk (95% CI)
50 Patients 20.0 2.65 (0.59, 11.86)
100 Patients 24.3 2.14 (0.84, 5.43)
200 Patients 18.1 1.08 (0.53, 2.20)
300 Patients 18.1 1.04 (0.58, 1.85)
400 Patients 18.4 1.07 (0.65, 1.76)
500 Patients 17.2 0.92 (0.58, 1.47)
600 Patients 15.8 0.81 (0.51, 1.26)
700 Patients 15.3 0.73 (0.48, 1.12)
800 Patients 14.7 0.65 (0.43, 0.99)
900 Patients 14.7 0.57 (0.40, 0.87)
1000 Patients 14.1 0.63 (0.43, 0.91)
1100 Patients 14.0 0.66 (0.46, 0.94)
1226 Patients 13.7 0.65 (0.46, 0.93)
Favours Reamed Favours Unreamed
1 5 100.5
Event Rate, % Relative Risk (95% CI)
50 Patients 20.0 2.65 (0.59, 11.86)
100 Patients 24.3 2.14 (0.84, 5.43)
200 Patients 18.1 1.08 (0.53, 2.20)
300 Patients 18.1 1.04 (0.58, 1.85)
400 Patients 18.4 1.07 (0.65, 1.76)
500 Patients 17.2 0.92 (0.58, 1.47)
600 Patients 15.8 0.81 (0.51, 1.26)
700 Patients 15.3 0.73 (0.48, 1.12)
800 Patients 14.7 0.65 (0.43, 0.99)
900 Patients 14.7 0.57 (0.40, 0.87)
1000 Patients 14.1 0.63 (0.43, 0.91)
1100 Patients 14.0 0.66 (0.46, 0.94)
1226 Patients 13.7 0.65 (0.46, 0.93)
Favours Reamed Favours Unreamed
1 5 100.5
Event Rate, % Relative Risk (95% CI)
50 Patients 20.0 2.65 (0.59, 11.86)
100 Patients 24.3 2.14 (0.84, 5.43)
200 Patients 18.1 1.08 (0.53, 2.20)
300 Patients 18.1 1.04 (0.58, 1.85)
400 Patients 18.4 1.07 (0.65, 1.76)
500 Patients 17.2 0.92 (0.58, 1.47)
600 Patients 15.8 0.81 (0.51, 1.26)
700 Patients 15.3 0.73 (0.48, 1.12)
800 Patients 14.7 0.65 (0.43, 0.99)
900 Patients 14.7 0.57 (0.40, 0.87)
1000 Patients 14.1 0.63 (0.43, 0.91)
1100 Patients 14.0 0.66 (0.46, 0.94)
1226 Patients 13.7 0.65 (0.46, 0.93)
Favours Reamed Favours Unreamed
1 5 100.5
Event Rate, % Relative Risk (95% CI)
50 Patients 20.0 2.65 (0.59, 11.86)
100 Patients 24.3 2.14 (0.84, 5.43)
200 Patients 18.1 1.08 (0.53, 2.20)
300 Patients 18.1 1.04 (0.58, 1.85)
400 Patients 18.4 1.07 (0.65, 1.76)
500 Patients 17.2 0.92 (0.58, 1.47)
600 Patients 15.8 0.81 (0.51, 1.26)
700 Patients 15.3 0.73 (0.48, 1.12)
800 Patients 14.7 0.65 (0.43, 0.99)
900 Patients 14.7 0.57 (0.40, 0.87)
1000 Patients 14.1 0.63 (0.43, 0.91)
1100 Patients 14.0 0.66 (0.46, 0.94)
1226 Patients 13.7 0.65 (0.46, 0.93)
Favours Reamed Favours Unreamed
1 5 100.5
Event Rate, % Relative Risk (95% CI)
50 Patients 20.0 2.65 (0.59, 11.86)
100 Patients 24.3 2.14 (0.84, 5.43)
200 Patients 18.1 1.08 (0.53, 2.20)
300 Patients 18.1 1.04 (0.58, 1.85)
400 Patients 18.4 1.07 (0.65, 1.76)
500 Patients 17.2 0.92 (0.58, 1.47)
600 Patients 15.8 0.81 (0.51, 1.26)
700 Patients 15.3 0.73 (0.48, 1.12)
800 Patients 14.7 0.65 (0.43, 0.99)
900 Patients 14.7 0.57 (0.40, 0.87)
1000 Patients 14.1 0.63 (0.43, 0.91)
1100 Patients 14.0 0.66 (0.46, 0.94)
1226 Patients 13.7 0.65 (0.46, 0.93)
Favours Reamed Favours Unreamed
1 5 100.5
Event Rate, % Relative Risk (95% CI)
50 Patients 20.0 2.65 (0.59, 11.86)
100 Patients 24.3 2.14 (0.84, 5.43)
200 Patients 18.1 1.08 (0.53, 2.20)
300 Patients 18.1 1.04 (0.58, 1.85)
400 Patients 18.4 1.07 (0.65, 1.76)
500 Patients 17.2 0.92 (0.58, 1.47)
600 Patients 15.8 0.81 (0.51, 1.26)
700 Patients 15.3 0.73 (0.48, 1.12)
800 Patients 14.7 0.65 (0.43, 0.99)
900 Patients 14.7 0.57 (0.40, 0.87)
1000 Patients 14.1 0.63 (0.43, 0.91)
1100 Patients 14.0 0.66 (0.46, 0.94)
1226 Patients 13.7 0.65 (0.46, 0.93)
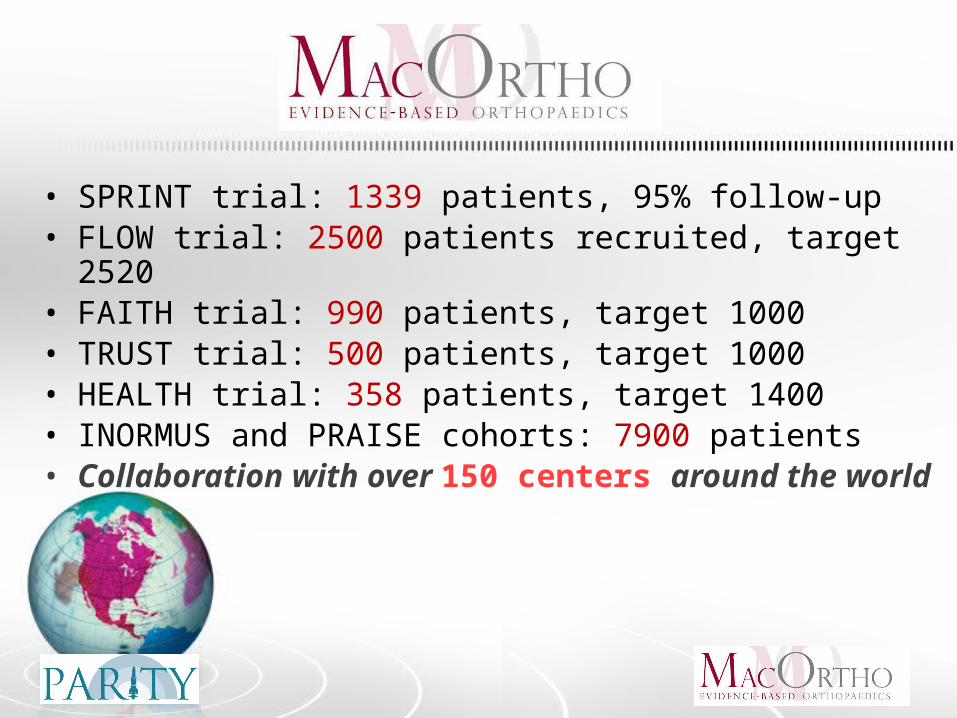
• SPRINT trial: 1339 patients, 95% follow-up• FLOW trial: 2500 patients recruited, target 2520• FAITH trial: 990 patients, target 1000• TRUST trial: 500 patients, target 1000• HEALTH trial: 358 patients, target 1400• INORMUS and PRAISE cohorts: 7900 patients• Collaboration with over 150 centers around the world
Preliminary Steps for a Surgical Trial
1. Find an important question
2. Systematic review
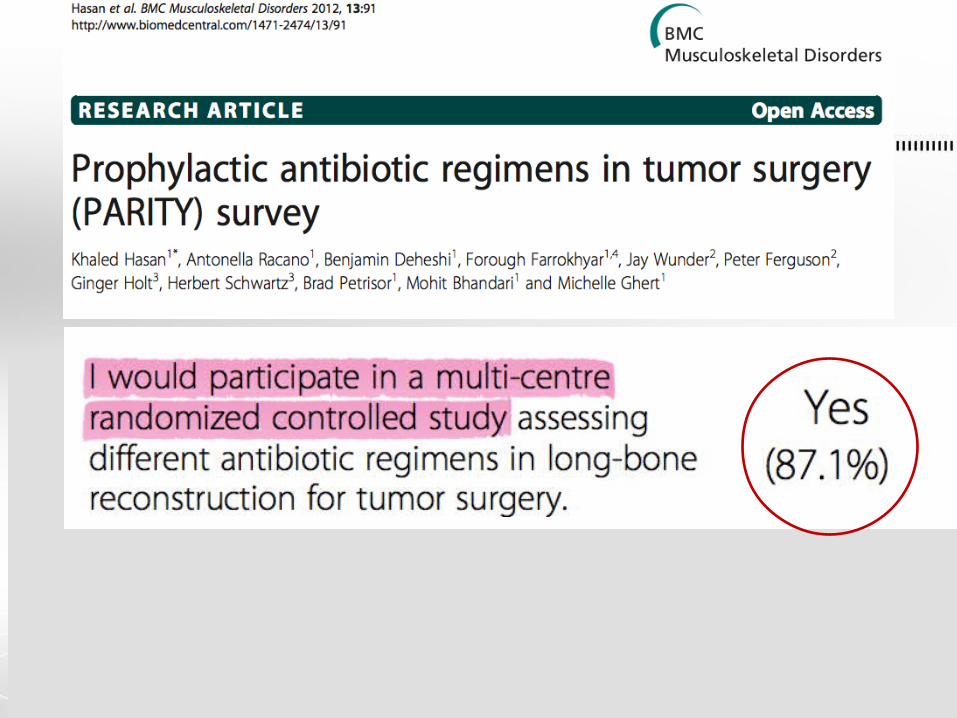
3. Survey the field
4. Publish a protocol
5. Apply for funding

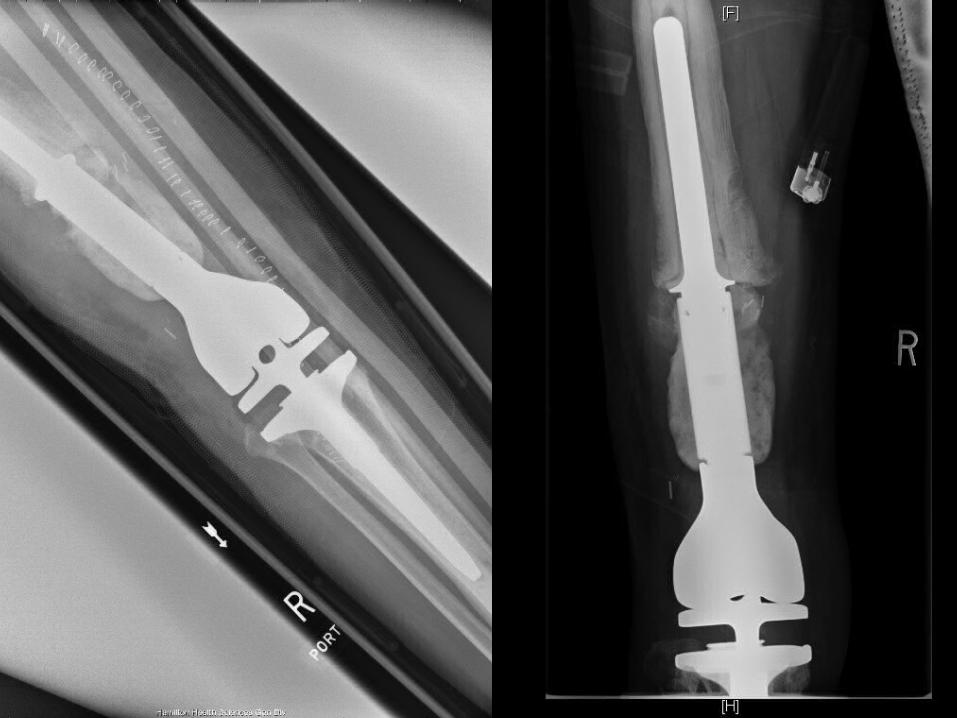
22 year-old male with sarcoma right femur







58year-old female




Clinical Question: PICO
PopulationInterventionComparisonOutcome

Preliminary Steps for a Surgical Trial
1. Find a question important to your field
2. Systematic review
3. Survey the field for practice and opinion
4. Publish a protocol
5. Apply for funding


Preliminary Steps for a Surgical Trial
1. Find an important question
2. Systematic review
3. Survey the field
4. Publish a protocol
5. Apply for funding

Length of Time Prophylactic Antibiotics Prescribed Following Long-bone Reconstruction
Type of Reconstruction 24 hrs 48 hrs 3-7 daysUntil Suction Drain Removed
Tumor prosthesis25 (35.7%)
13 (18.6%)
3 (4.3%) 29 (41.4%)
Allograft18 (26.5%)
13 (19.1%)
11 (16.2%)
26 (38.2%)
Allograft-prosthesis composite
17 (25.4%)
12 (17.9%)
9 (13.4%)
29 (43.3%)


Preliminary Steps for a Surgical Trial
1. Find an important question
2. Systematic review
3. Survey the field
4. Publish a protocol
5. Apply for funding

Patient screened and eligible and
provides informed consent
Randomization
Standard pre-op and intra-op antibiotics AND 24 hours post op antibiotics
Standard pre-op and intra-op antibiotics AND 5 days post op antibiotics
Follow-up one year
Follow-up one year
Study Design


Sample Size Calculation
• Infection rate: 10%• Superiority of long-term antibiotics:
– threshold of 5% for inferiority
• Estimated sample size of 920
Preliminary Steps for a Surgical Trial
1. Find an important question
2. Systematic review
3. Survey the field
4. Publish a protocol
5. Apply for funding

Writing Grants

Research Funding: Pilot (vanguard phase)

What you need to run RCTs
• Trials require: 1. The right question √
2. Centralized infrastructure
3. Collaborative network

What you need to run RCTs
• Trials require: 1. The right question √
2. Centralized infrastructure
3. Collaborative network
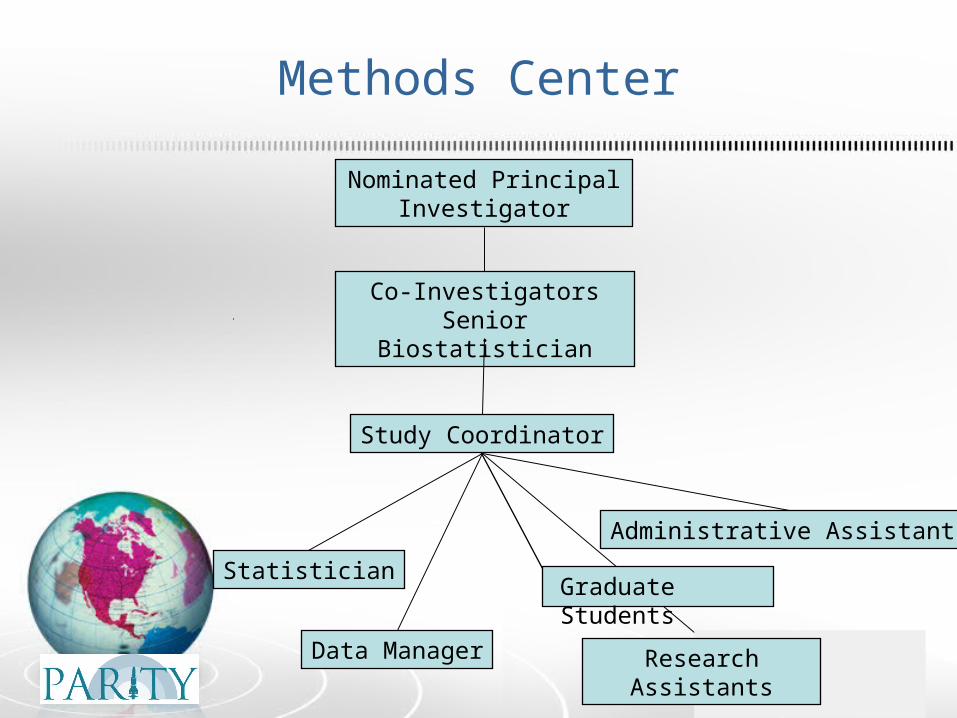
Methods Center
Nominated Principal Investigator
Co-InvestigatorsSenior Biostatistician
Statistician
Data Manager
Study Coordinator
Research Assistants
Administrative Assistants
Graduate Students

Central Source of Information

Newsletter and website

Budgeting and Contracts
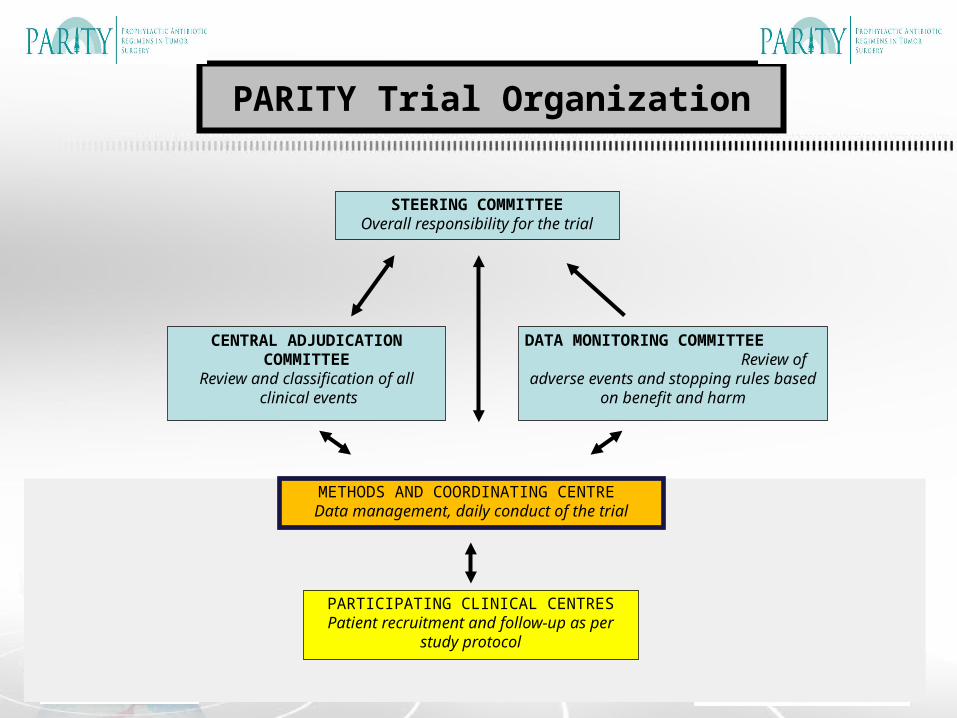
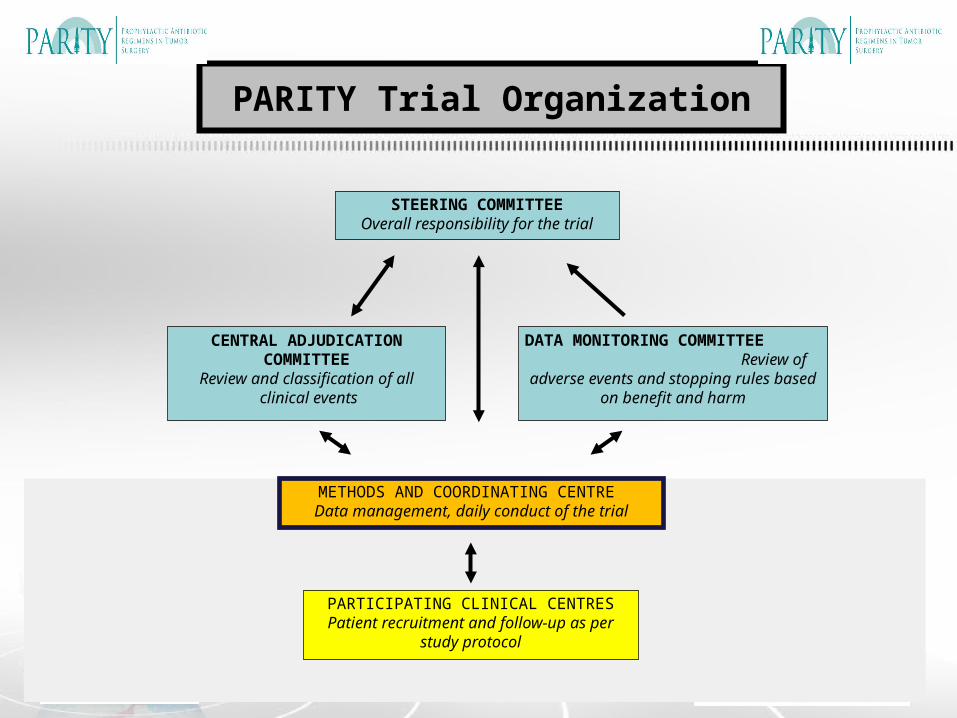
STEERING COMMITTEEOverall responsibility for the trial
CENTRAL ADJUDICATION COMMITTEE
Review and classification of all clinical events
DATA MONITORING COMMITTEE Review of adverse events and stopping rules based on benefit and harm
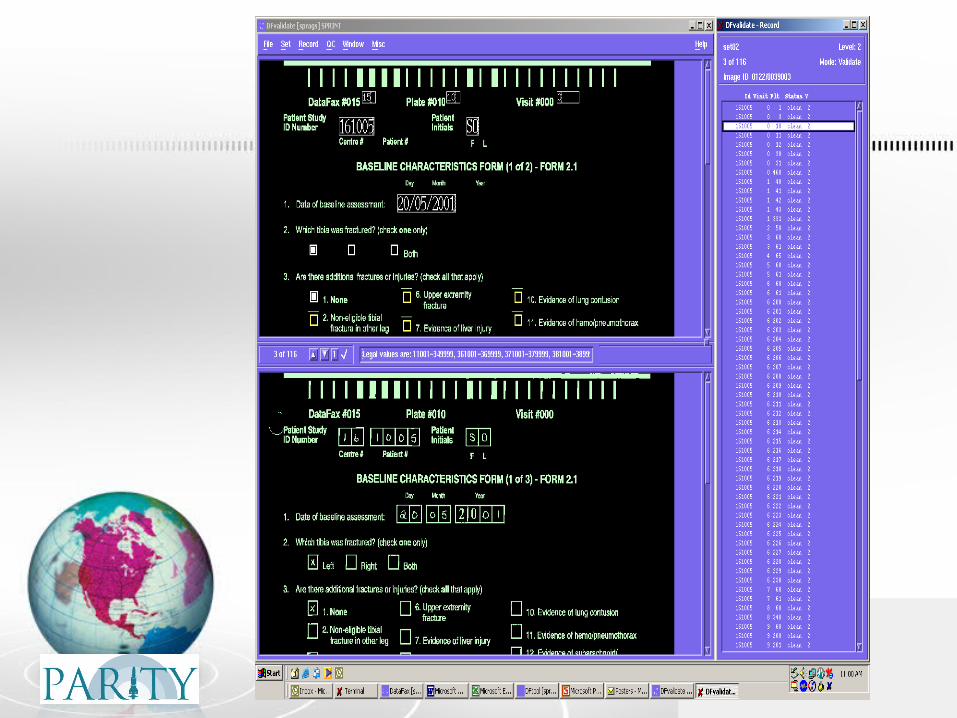
METHODS AND COORDINATING CENTRE Data management, daily conduct of the trial
PARTICIPATING CLINICAL CENTRES Patient recruitment and follow-up as per
study protocol
PARITY Trial Organization

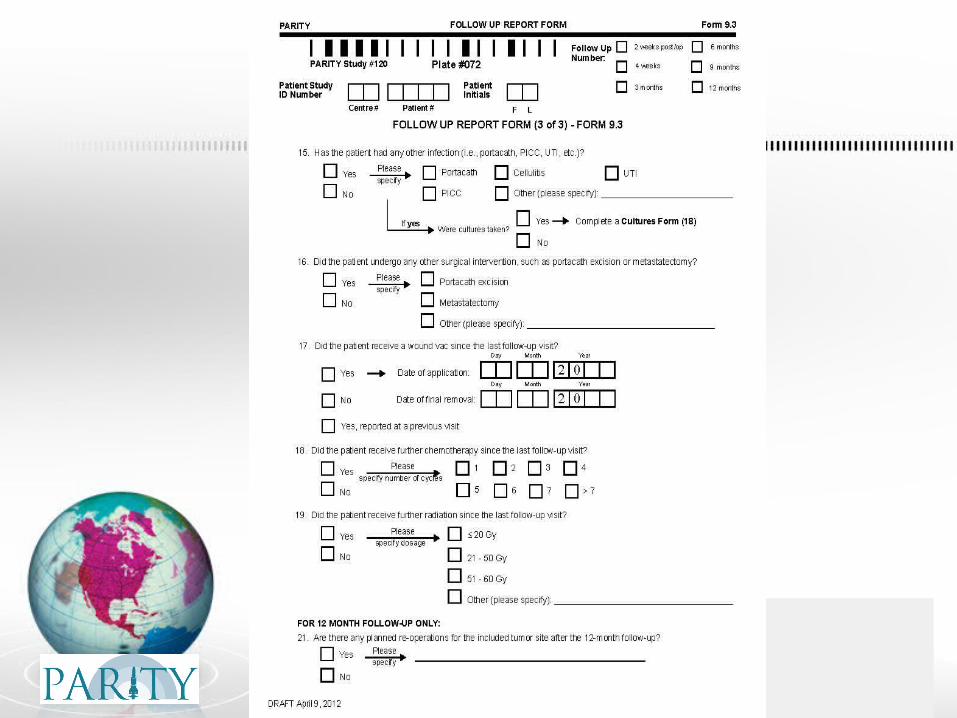

Adjudication

Methods Center Personnel
Nominated Principal Investigator
Co-InvestigatorsSenior Biostatistician
Statistician
Data Manager
Study Coordinator
Research Assistants
Grants Administrator
Graduate Students

Principal Investigator
Nominated Principal Investigator
Co-InvestigatorsSenior Biostatistician
Statistician
Data Manager
Study Coordinator
Research Assistants
Grants Administrator
Graduate Students
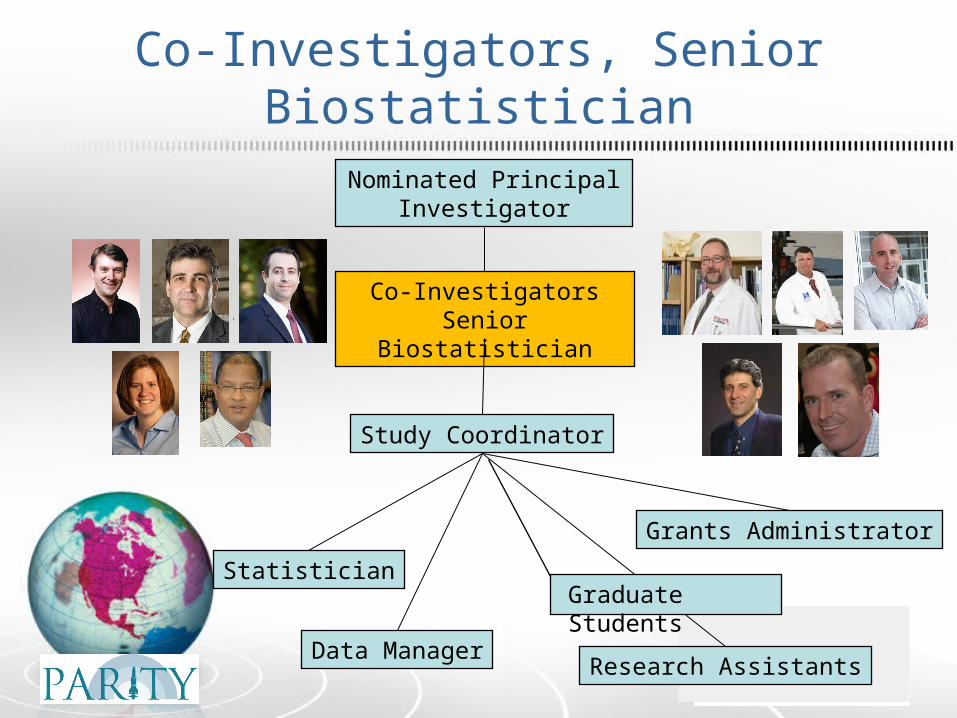
Co-Investigators, Senior Biostatistician
Nominated Principal Investigator
Co-InvestigatorsSenior Biostatistician
Statistician
Data Manager
Study Coordinator
Research Assistants
Grants Administrator
Graduate Students
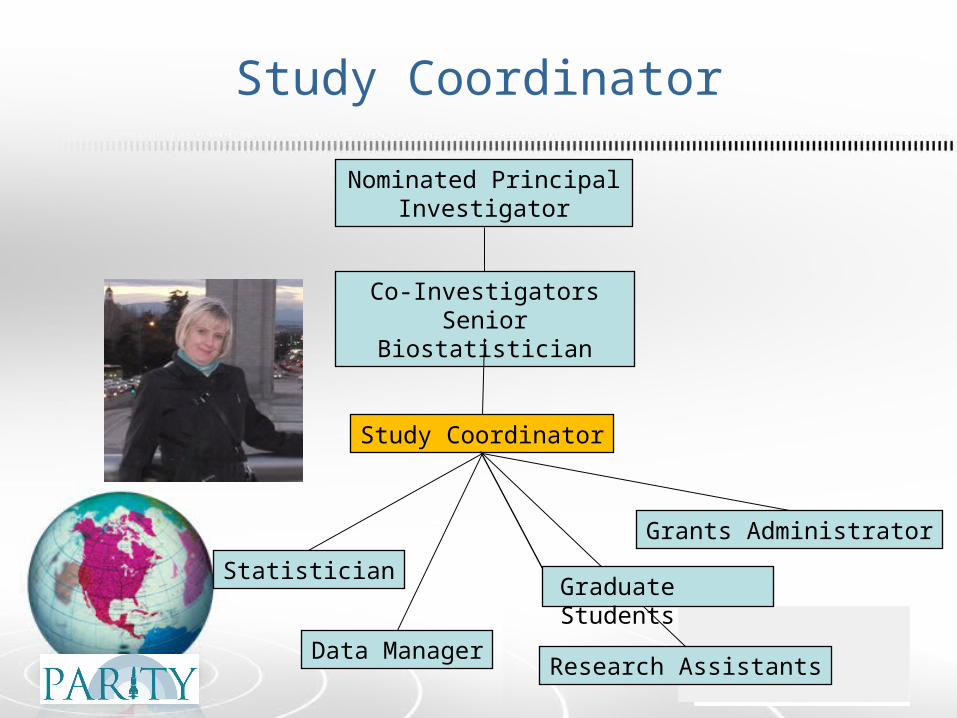
Study Coordinator
Nominated Principal Investigator
Co-InvestigatorsSenior Biostatistician
Statistician
Data Manager
Study Coordinator
Research Assistants
Grants Administrator
Graduate Students

Statistician
Nominated Principal Investigator
Co-InvestigatorsSenior Biostatistician
Statistician
Data Manager
Study Coordinator
Research Assistants
Grants Administrator
Graduate Students

Data Manager
Nominated Principal Investigator
Co-InvestigatorsSenior Biostatistician
Statistician
Data Manager
Study Coordinator
Research Assistants
Grants Administrator
Graduate Students

Graduate Students
Nominated Principal Investigator
Co-InvestigatorsSenior Biostatistician
Statistician
Data Manager
Study Coordinator
Research Assistants
Grants Administrator
Graduate Students

Research Assistants
Nominated Principal Investigator
Co-InvestigatorsSenior Biostatistician
Statistician
Data Manager
Study Coordinator
Research Assistants
Grants Administrator
Graduate Students

Grants Administrator
Nominated Principal Investigator
Co-InvestigatorsSenior Biostatistician
Statistician
Data Manager
Study Coordinator
Research Assistants
Grants Administrator
Graduate Students
What you need to run RCTs
• Trials require: 1. The right question √
2. Centralized infrastructure √
3. Collaborative network

What you need to run RCTs
• Trials require: 1. The right question √
2. Centralized infrastructure √
3. Collaborative network

STEERING COMMITTEEOverall responsibility for the trial
CENTRAL ADJUDICATION COMMITTEE
Review and classification of all clinical events
DATA MONITORING COMMITTEE Review of adverse events and stopping rules based on benefit and harm
METHODS AND COORDINATING CENTRE Data management, daily conduct of the trial
PARTICIPATING CLINICAL CENTRES Patient recruitment and follow-up as per
study protocol
PARITY Trial Organization

International PARITY Sites

PARITY Investigators
Michelle Ghert, Benjamin Deheshi, Gita Sobhi, Peter Ferguson, Jay Wunder, Robert Turcotte, Joel Werier, Paul Clarkson, Marc Isler, R. Lor Randall, Ginger Holt, Megan Anderson, John Healey, Marcos Galli, Rob Grimer, Tom Scharschmidt, Ed Chang, Benjamin Miler, Norbert Dion, Sevan Hopyan, Rob Pollock, Graig Gerrand, William Aston, Max Gibbons, John Abraham, Tessa Balach, Paul Cool. Minna Laitinen, Yair Gortzak, Yoshihiro Nishida, Tabu Gokita, Doran Frantzen, Leonard Marais, Matthew DiCaprio, Felix Cheung, Howard Rosenthal, Ernest Conrad, Timothy Damron, Joseph Benevenia, Mark Gebhardt, Sophie Mottard, Nathan Evaniew, Antonella Racano, Sheila Sprague, Marilyn Swinton, Dianne Bryant, Lehana Thabane, Gordon Guyatt, Mohit Bhandari

Dec '12 Jan '13 Feb Mar Apr May Jun Jul
0
5
10
15
20
25
30
35
Cumulative Enrollment

Paradigm shift from Level IV to Level I Evidence
Take Home Points
• Trials require: 1. The right question
2. Centralized infrastructure
3. Collaborative network• Collaboration is the foundation of RCTs, without
which the endeavour will collapse

Thank-you