Embed Size (px)
Citation preview

Int J Anat Res 2015, 3(1):821-24. ISSN 2321-4287 821
Original Article
CLINICO-ANATOMICAL STUDY OF VARIATIONS IN ARTERIALSUPPLY OF ADULT HUMAN STOMACHSaif Omar *1, Md. Shakeb Ahmad 2,Nafees Fatima 3, Md. Arif Ansari 4.
ABSTRACT
Address for Correspondence: Dr. Saif Omar, Associate Professor, Department of Anatomy, KatiharMedical College, Katihar – 854105 Bihar, INDIA. Mobile No.: +919431229999E-Mail: [email protected]
Access this Article online
Quick Response code Web site:
*1 Associate Professor, Department of Anatomy, Katihar Medical College, Katihar, Bihar, India.2 Assistant Professor, Department of Surgery, Katihar Medical College, Katihar, Bihar, India.3 Senior Resident, Department of Anatomy, Indira Gandhi Institute of Medical Sciences, Patna,Bihar, India.4 Professor & Head, Department of Surgery, Katihar Medical College, Katihar, Bihar, India.
Anatomical variations in the arterial supply of adult human stomach have long baffled even the most experiencedsurgeons during surgical manipulation of the stomach. The stomach develops from the foregut hence its arterialsupply is derived from the coeliac trunk. The present study is aimed at observing the anatomical variations ofthe arteries supplying the stomach. This study has been conducted on fifty cadavers during routine dissections.The aberrant arteries observed have both embryological and clinical significance. A comprehensive knowledgeof the arteries nourishing the stomach along with their anomalies is vital for the surgeons to avoid iatrogeniccomplications during surgical manipulation involving the organ.KEYWORDS: Arterial, Foregut, Stomach, Anomalies, Complications.
INTRODUCTION
International Journal of Anatomy and Research,Int J Anat Res 2015, Vol 3(1):821-24. ISSN 2321- 4287
DOI: 10.16965/ijar.2014.499
Received: 01 Sep 2014Peer Review: 01 Sep 2014 Published (O):31 Jan 2015Accepted: 13 Jan 2015 Published (P):31 Mar 2015
International Journal of Anatomy and ResearchISSN 2321-4287
www.ijmhr.org/ijar.htm
DOI: 10.16965/ijar.2014.499
The stomach is a saclike dilatation of thealimentary canal [1]. In cadavers, the stomachis sickle shaped, the wider end being directedupwards and to the left [2]. From clinical expe-rience the arterial supply of the stomach haslong been postulated to be exceptionally rich[3]. In conventional textbooks the arterialsupply of stomach is by the coeliac trunk directlyor indirectly and the arteries reach the organalong its curvatures. The arteries are leftgastric artery branch of coeliac trunk and is theprincipal artery of the stomach; right gastricartery branch of common hepatic artery; shortgastric branches of splenic artery; left gastro-epiploic artery branch of splenic artery; right
gastroepiploic artery branch of gastroduodenalartery and posterior gastric artery occasionalbranch of splenic artery. Known to Walther [4]since 1740 and termed by Haller [5] in 1745 asthe posterior gastric branch, this artery and itssurgical importance have been at best ignoredand at worst neglected [6] in spite of severalpublications on variations of arterial supply ofthe stomach.
MATERIALS AND METHODS
Conventional cadaveric dissections for academicteaching of first year MBBS students wereperformed on 50 embalmed male cadavers agedbetween 25 to 65 years. After exposing theabdominal cavity and removing the peritonealfat, the coeliac trunk was located and each of

Int J Anat Res 2015, 3(1):821-24. ISSN 2321-4287 822
Saif Omar et al.. CLINICO-ANATOMICAL STUDY OF VARIATIONS IN ARTERIAL SUPPLY OF ADULT HUMAN STOMACH.
its three branches was individually examined.Emphasis was laid on arteries supplying thestomach with particular focus on occurrence ofposterior gastric branch of splenic artery.
OBSERVATIONS
In all cases the coeliac trunk was given off asthe first anterior branch of abdominal aorta justinferior to the aortic hiatus of the thoraco-abdominal diaphragm and was found to lie atthe level of lower border of body twelfth thoracicvertebra. The coeliac trunk was trifurcated in allcases. In thirty eight cases (76%) it gave the“tripus halleri” or classical trifurcation ofcommon hepatic, left gastric and splenic arterieshaving a common point of origin and in twelvecases (24%) showed non classical trifurcationin which the left gastric artery demonstrated avariable pattern of origin. Variations in level ofthe coeliac trunk were not observed. In forty sixcases (92%) a single left gastric artery branchingfrom the coeliac trunk was observed and out ofthe remaining four cases in three cases (6%) theartery branched from the common hepatic arteryand in one case (2%) the artery revealed anaccessory left gastric artery branching directlyand independently from the abdominal aorta. Inforty nine cases (98%) the right gastric arterybranched from the common hepatic artery andonly in one case (2%) an accessory right gastricartery was observed to be branching directlyfrom the coeliac trunk. In all cases short gastricarteries branching classically from the splenicartery were observed. None of the casesrevealed any anomalies in the right and leftgastroepiploic arteries respectively. Posteriorgastric artery originated from the splenic arteryin twelve cases (24%).
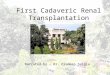
Fig. 1: Showing the Coeliac Trunk.
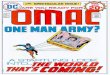
Fig. 2: Showing Branches of the Coeliac Trunk.
DISCUSSION
Until coeliac and mesenteric angiographyconfirmed that previously noted pronouncedvariations in arterial supply to the stomach andduodenum occur, these variations have notalways been adequately considered by theoperating surgeons. Arterial supply to thestomach comes predominantly from the coeliacaxis although intramural anastomoses exist withvessels of other origins at the two ends of thestomach. The coeliac trunk supplies the abdomi-nal part of oesophagus, stomach, duodenumupto major duodenal papilla, liver, pancreas, gallbladder and spleen. The common hepatic,splenic and left gastric arteries are consideredas the “main classic” branches of the coeliactrunk [7]. The coeliac trunk is the chief artery ofthe foregut. It supplies all the derivatives of theforegut that lie in the abdominal cavity. Theanatomical variations of the coeliac trunk aredue to unusual embryological development ofthe ventral splanchnic branches of the aorta [8].The formation of the aorta begins during the thirdweek of embryological development. Manysegmental arteries arise from the primitivedorsal aorta. As the embryo continues todevelop, most segmental arteries regress,except for the precursor of the segmental arter-ies to the three major mesenteric vessels. Thetenth segmental artery gives rise to the coeliactrunk [9]. The left gastric artery is the smallestbranch of the coeliac axis [10]. The left gastricartery may arise from the common hepaticartery or its branches. The most commonvariant is an origin from the left hepatic artery.

Int J Anat Res 2015, 3(1):821-24. ISSN 2321-4287 823
Saif Omar et al.. CLINICO-ANATOMICAL STUDY OF VARIATIONS IN ARTERIAL SUPPLY OF ADULT HUMAN STOMACH.
Other variants include a common origin with thecommon hepatic artery. Identification of anaberrant origin may be of importance duringsurgical mobilization of the upper stomach [10].In our study variations in origin of the leftgastric artery was observed in four cases (8%)out of which in one case an accessory leftgastric artery was also observed. Ishiqami K etal studied 118 patients with conventionalangiography for detection of an accessory leftgastric artery [11]. Result of this study revealedan accessory left gastric artery in 25 out of 118cases. According to Hollinshead W.H. [12] anaccessory left gastric artery is present in about11.5% of the population. It arises from the aortaindependently in about 4.5% of the population.The right gastric artery arises from the commonhepatic artery and its origin is often variant. Themost common alternative origins are from theleft hepatic, gastroduodenal or supraduodenalarteries [13]. An accessory right gastric arteryis present in about 1.45% of the population [7].In our study in only one case (2%) we observedthe presence of an accessory right gastric ar-tery. We did not observe any variations in rightand left gastroepiploic arteries. They were seento branch from gastroduodenal and splenicarteries respectively. The splenic artery is thelargest branch of the coeliac trunk. The splenicartery gives off five to six short gastric branchesand the left gastroepiploic artery. From themiddle part of its course the splenic artery maygive off a posterior gastric artery (PGA) to thestomach [14]. The high incidence and the widedistribution of the PGA to the stomach are insharp contrast with the absence of descriptionin most modern textbooks of anatomy. DiDio etal [15] found the PGA in 46% of their subjects.According to DiDio, the surgical importance ofthe posterior gastric arteries attributed to itsrelatively high incidence and the fact that itaugments the blood supply to the superior partof the posterior surface and to the fundus. Theartery has a deep and almost hidden origin fromthe splenic artery. Overlooking this vessel inparticular may cause postsurgical haemorrhageif this vessel is inadvertently transected duringsurgery [6]. In our study we observed PGA intwelve cases (24%) and all were observed tooriginate from the splenic artery. This artery may
be an important channel in cases where majorgastric arterial supply has been compromised.According to Loukas et al [16] the mostcommon origin of PGA was from the left gastricartery in 41.8% cases, from splenic artery in25.2% cases, double PGA in 22.4% cases andfrom coeliac trunk in 10.2% cases. Acoeliacographic study reported PGA in 55.7%cases [17]. Each artery supplying the stomachhas its own importance regarding variations. Thegastroepiploic arteries observed in our studywere least notorious.
CONCLUSION
As anatomists and surgeons we state that in ouropinion gastric arterial variations should not beoverlooked during abdominal surgeries involvingthe stomach. Many complications can beavoided with precise knowledge of theseaberrant arteries. While vascular anomalies areusually asymptomatic, they may becomeimportant in patients undergoing diagnosticangiography for gastrointestinal bleeding orcoeliac axis compression syndrome. Knowledgeof such variations can aid in the interpretationof angiographic studies.Acknowledgement: The authors wish toacknowledge the guidance and supervisionreceived from Dr. Vakil Ahmed, Professor ofAnatomy, Katihar Medical College.
[1]. Rosse C. Hollinshead’s textbook of anatomy, 5th
Edition, Lippincott – Raven, 1997, pp 553.[2]. Datta A.K. Essentials of human anatomy, 8th Edition,
Vol-1, Current Books International, pp 188.[3]. Brown R.J. Arterial supply of human stomach. AMA
Arch Surg. 1952;64(5):616-621.[4]. Walther A.F. De Vena Portae. Lipsiae, 1740.[5]. Haller A. Icones Anatomicae Quibus Praecipue
Aliquae Partes Corporis Humani DelineataeProponuntur et Arteriarum Potissimum HistoriaContinetur. Fasciculus II. Gottingae: Vandenhoeck,1745.
[6]. Suzuki K. Incidence and surgical importance of theposterior gastric artery. Ann. Surg. Feb. 1978. Vol187(2): 134-136.
[7]. Salve V.M. Multiple variation of branches ofabdominal aorta. Kathmandu Univ Med J 2011;33(1):72-76.
[8]. Chiang K. Angiographic evaluation of hepatic arteryvariations in 405 cases. Chin J Radiol 2005; 30:75-81.
Conflicts of Interests: None
REFERENCES

Int J Anat Res 2015, 3(1):821-24. ISSN 2321-4287 824
Saif Omar et al.. CLINICO-ANATOMICAL STUDY OF VARIATIONS IN ARTERIAL SUPPLY OF ADULT HUMAN STOMACH.
How to cite this article:Saif Omar, Md. Shakeb Ahmad, Nafees Fatima, Md. Arif Ansari.CLINICO-ANATOMICAL STUDY OF VARIATIONS IN ARTERIALSUPPLY OF ADULT HUMAN STOMACH. Int J Anat Res2015;3(1):821-824. DOI: 10.16965/ijar.2014.499
[9]. Lin P.H. Embryology, anatomy and surgical exposureof the great abdominal vessels. Surg. Clin. NorthAm. 2000 Feb; 80(1):417-33.
[10]. Standring S. Gray’s Anatomy, 39th Edition: ElsevierChurchil l Livingstone 2005. Stomach andabdominal oesopgahus:1146.
[11]. Ishiqami K. Accessory left gastric artery from lefthepatic artery shown on MDCT and conventionalangiography. AJR Am J Roentgenol 2006;187(4):1002-1009.
[12]. Hollinshead W.H. Anatomy for surgeons. Vol:2, 2nd
Edition, New York, Harper & Row Publisher,1961:590.
[13]. Standring S. Gray’s Anatomy, 39th Edition: ElsevierChurchil l Livingstone 2005. Stomach andabdominal oesopgahus:1148.
[14]. Sinnatamby C.S. Last’s anatomy: regional andapplied. 11th Edition. London: Churchill Livingstone2006:251.
[15]. DiDio L.J. Posterior gastric artery and itssignificance as seen on angiograms. Am J Surg 1980Mar;139(3):333-337.
[16]. Loukas M. The clinical anatomy of posterior gastricartery revisited. Surg Radiol Anat 2007Jul;29(5):361-366.
[17].Okabayashi T. Posterior gastric artery inangiograms and its surgical importance.Hepatogastroenterology 2005 Jan-Feb;52(61):298-301.